
Abstract
Introduction:
Laparoscopic cholecystectomy (LC) during index hospitalization for gallstone pancreatitis is standard in adult populations. The objective of this study was to evaluate trends in use of LC and endoscopic retrograde cholangiopancreatography (ERCP) for children with gallstone pancreatitis.
Materials and Methods:
This retrospective cohort study used the Kids' Inpatient Database, spanning 2000–2019, to identify patients aged 18 years or younger with a principal diagnosis of gallstone pancreatitis. The Mann–Kendall trend test was used to assess trends over time.
Results:
Gallstone pancreatitis occurred in 5028 patients. The rate of LC during index hospitalization ranged from 55.4% to 63.8% (P = .76). Trends demonstrate that LC occurred on average hospital day 4.6 in 2000 and decreased to 3.4 in 2019 (P < .01). Among those undergoing LC, average length of stay (LOS) decreased from 6.8 days in 2000 to 5.1 days in 2019 (P < .01). The rate of ERCP alone decreased from 24.8% in 2000 to 14.0% in 2019 (P = .23). For those undergoing ERCP, average hospital day of ERCP decreased from 3.3 in 2000 to 2.3 in 2019 (P = .07). The rate of undergoing both an ERCP and LC decreased from 19.0% in 2000 to 8.5% in 2019 (P = .13). For patients who underwent either LC or ERCP, average LOS decreased from 7.0 days in 2000 to 5.1 days in 2019 (P < .01). For patients who did not undergo a procedure, average LOS decreased from 5.7 days in 2000 to 4.0 days in 2019 (P = .13).
Conclusion:
The proportion of LC performed during index hospitalizations for children with gallstone pancreatitis has been stable for two decades. However, trends indicate that interventions are occurring earlier, and LOS is becoming shorter.
Introduction
Acute pancreatitis is not common in the pediatric population occurring at a rate of 3–13 cases per 100,000 children per year, but the incidence has been increasing over the last decade.1–5 The most common etiology of acute pancreatitis in children is biliary disease, such as gallstones or microlithiasis, accounting for up to 30% of all cases.1,6
In the adult population, patients who presented with acute gallstone pancreatitis had a risk of recurrence up to 11.1% in those who underwent only endoscopic retrograde cholangiopancreatography (ERCP) and up to 22.7% for those who had no intervention. 7 Therefore, in adults who present with mild, self-limited gallstone pancreatitis, the recommendation is to undergo cholecystectomy during the same hospitalization to prevent recurrent episodes.8–10
Laparoscopic cholecystectomy (LC) during index hospitalization for the pediatric population is not as well-studied as in adults, but the literature in the pediatric population is in concordance with the adult literature in that there are high recurrence rates of gallstone pancreatitis without cholecystectomy. A single-center study in pediatric patients by Badru et al. found a gallstone pancreatitis recurrence rate of 31% for patients who did not undergo cholecystectomy during index hospitalization. 3 Another more recent study out of the United Kingdom found an absolute risk reduction of 57.5% for readmission for gallstone pancreatitis if pediatric patients underwent cholecystectomy within 2 weeks of diagnosis. 4 The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Pancreas Committee released guidelines in 2018 recommending cholecystectomy before discharge in pediatric patients with mild, acute gallstone pancreatitis. 11
The objective of this study was to describe the use of LC and/or ERCP during index hospitalization for gallstone pancreatitis over time. In addition, we aimed to evaluate factors associated with the timing of LC and/or ERCP during index hospitalization over time.
Materials and Methods
Data source
The Kids' Inpatient Database (KID) spanning from 2000 to 2019 was used for this analysis. KID is part of a family of databases developed for the Health care Cost and Utilization Project, which is sponsored by the Agency for Healthcare Research and Quality. 12 This database was developed through a Federal-State-Industry partnership to inform decision making at the national, state, and community levels. KID is the largest publicly-available all-payer pediatric inpatient care database in the United States. Data are available every 3 years and contain data from about three million pediatric (age 20 or younger) discharges per year. 12
Study population
This retrospective cohort study included patients aged 18 years or younger with a principal diagnosis of gallstone pancreatitis. Patients with gallstone pancreatitis were identified using International Classification of Diseases ninth (ICD-9) or 10th editions (ICD-10) that either identified biliary pancreatitis or acute pancreatitis with a concomitant code for cholelithiasis, cholecystitis, or biliary colic (Supplementary Table S1). Patients were excluded if they had acute pancreatitis for any other cause other than biliary or if they underwent LC on day of admission. The Ann and Robert H. Lurie Children's Hospital of Chicago's Institutional Review Board (IRB) approved this study (IRB No. 2022-5318).
Outcome variables
Primary outcomes of interest were rates of LC or ERCP performed during the same hospitalization over time. As stated, LC performed on day of admission was excluded because it was thought these patients had previously been diagnosed with gallstone pancreatitis and were therefore receiving a scheduled, interval cholecystectomy. Procedures were identified using ICD-9 and ICD-10 codes (Supplementary Table S2). Secondary outcomes of interest were trends in the timing of LC and ERCP during the hospitalization, and overall length of stay (LOS).
Covariates
Data were extracted for sex, age, hospital region, hospital type, bedsize, and insurance status from KID. Sex was a binary variable, either female or male. Age was collected as a continuous variable in years. Hospital region was a categorical variable defined as Northeast, Midwest, South, and West. The region was determined based on the American Hospital Association (AHA) Annual Survey of Hospitals. Hospital type was defined as rural nonteaching, urban nonteaching, or urban teaching. This was determined based on the AHA Annual Survey of Hospitals. Teaching hospitals have an approved residency program or membership in the Council of Teaching Hospitals. 12
Bedsize was defined as small, medium, or large based on the number of short-term acute beds in a hospital. Small was defined as 1–49 beds for a rural hospital, 1–99 for urban nonteaching, and 1–299 for urban teaching. Medium was defined as 50–99 beds for a rural hospital, 100–199 for urban nonteaching, and 300–499 for urban teaching. Large was defined as 100+ beds for a rural hospital, 200+ for urban nonteaching, and 500+ for urban teaching. 12 Insurance status was a categorical variable defined as Medicare, Medicaid, private insurance, self-pay, or other. Other included worker's compensation, Civilian Health and Medical Program of the Uniformed Services, Title V, and other government programs. 12
Statistical analysis
Categorical variables were reported as number and percentage. Continuous variables were reported as median with interquartile range (IQR) or mean with standard deviation. Differences among groups were evaluated with chi-squared or Fisher's exact tests for categorial variables and Wilcoxon rank-sum tests for continuous variables. The Mann–Kendall trend test was used to assess for statistically significant trends over time. Multivariable logistic regressions were performed to evaluate the association of undergoing LC, ERCP, both, or no procedure based on sex, age, hospital region, type, bed size, and insurance status. Covariates were included in the multivariable regressions if they were found to be significant on univariate analyses, with the exclusion of race as there was high rate of missing data. All analyses were conducted using SAS version 9.4 (Cary, NC, USA). The level of significance was set to P < .05.
Results
Patient demographics
Among 5028 patients with gallstone pancreatitis, the median age was 16 years (IQR: 14–17). The majority of patients (76.2%) were female. Of the patients, 36.1% were White, 32.8% Hispanic, and 10.4% Black. Most patients were treated at an urban teaching hospital (63.9%) in either the South (34.1%) or West (32.0%). Overall, 2,315 (46.0%) of patients underwent LC only, 325 (6.5%) had only an ERCP, 653 (13.0%) had both LC and ERCP, and 1735 (35.5%) patients had no procedure during their index hospitalization for gallstone pancreatitis (Table 1).
Patient Demographics by Procedure During Index Hospitalization for Gallstone Pancreatitis
ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy.
Rates of procedures over time
From 2000 to 2019, the rate of LC during index hospitalization ranged from 55.4% to 63.8% with no statistically significant trend over time (P = .76). The rate of ERCP alone decreased from 24.8% in 2000 to 14.0% in 2019, but was not statistically significant (P = .23). The rate of undergoing both an ERCP and LC decreased from 19.0% in 2000 to 8.5% in 2019, but was also not statistically significant (P = .13; Fig. 1).

Rates of intervention .(LC, ERCP, or both) during the index hospitalization for gallstone pancreatitis over time. ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy.
Hospital day of procedure and LOS trends
Trends demonstrated that LC occurred on average hospital day 4.6 in 2000 and decreased to 3.4 in 2019 (P < .01). Among those undergoing LC, average LOS decreased from 6.8 days in 2000 to 5.1 days in 2019 (P < .01). For patients undergoing ERCP, average hospital day of ERCP decreased from 3.3 in 2000 to 2.3 in 2019 (P = .07), and average LOS decreased from 7.2 days in 2000 to 5.2 days in 2019 (P = .13). For the 3293 (65.5%) patients who underwent either LC or ERCP, average LOS decreased from 7.0 days in 2000 to 5.1 days in 2019, P < .01. For patients who did not undergo a procedure, average LOS decreased from 5.7 days in 2000 to 4.0 days in 2019 (P = .13).
Features associated with undergoing LC or ERCP
Patients had higher odds of undergoing LC if they were female (odds ratio: 1.33 [95% confidence interval: 1.16–1.52]) compared to male. Patients also had higher odds of undergoing LC if they were older in age (1.10 [1.08–1.12]). There were lower odds of undergoing LC in the Northeast (0.71 [0.59–0.85]) or Midwest (0.76 [0.64–0.90]) compared to the West. Patients also had lower odds of undergoing LC in rural nonteaching hospitals (0.76 [0.61–0.94]) compared to urban teaching hospitals, or if they were treated at a small (0.72 [0.60–0.86]) compared to a large hospital. Finally, patients had lower odds of LC if they had private insurance (0.87 [0.76–098]) compared to public insurance (Fig. 2a).
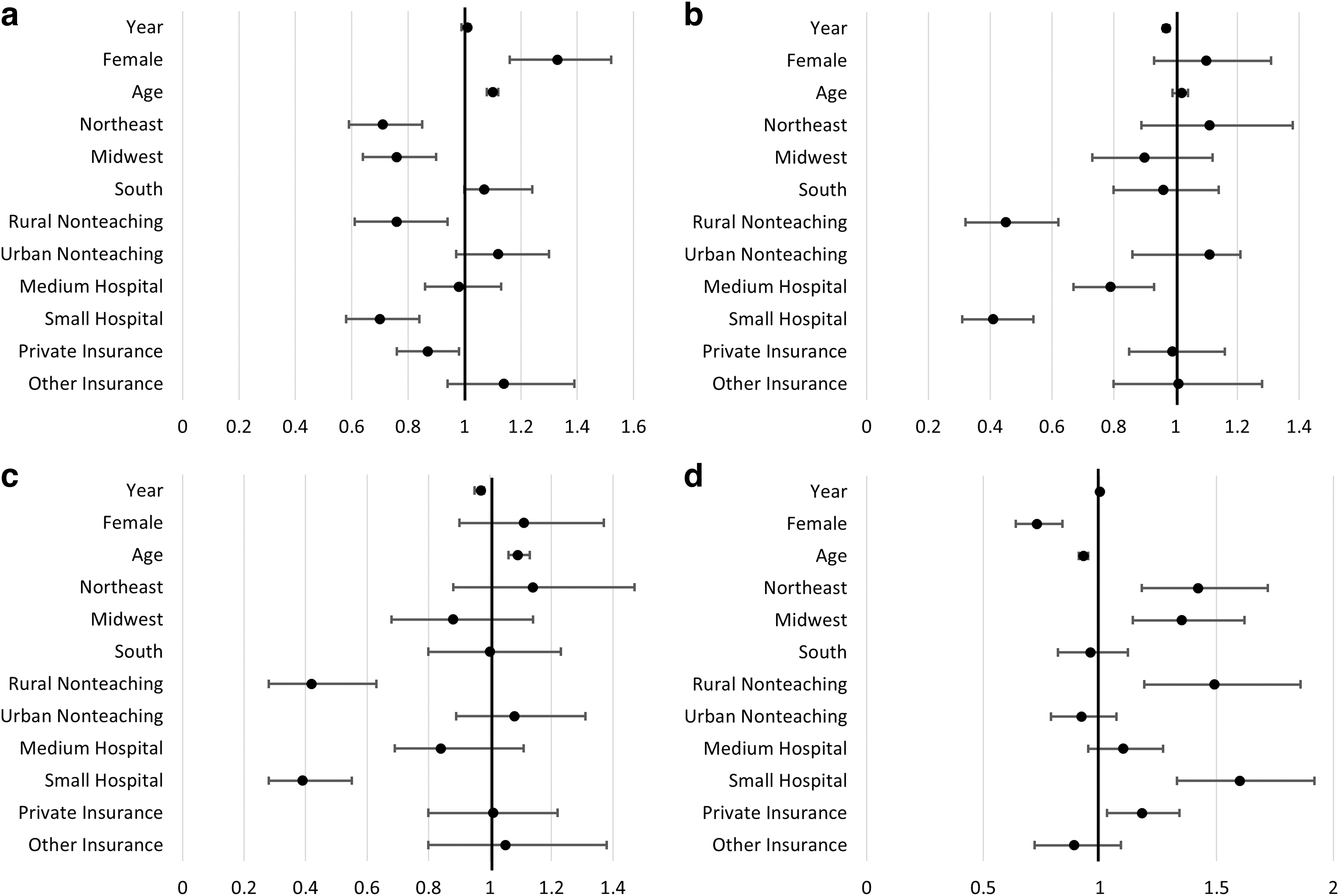
Multivariable logistic regressions evaluating the odds of undergoing
Patients had lower odds of undergoing ERCP if they were treated at a rural nonteaching hospital (0.45 [0.32–0.62]) compared to urban teaching hospitals, or if they were treated at a small (0.41 [0.31–0.55]) or medium (0.79 [0.67–0.94]) hospital compared a large hospital (Fig. 2b).
There were higher odds of undergoing both LC and ERCP if the patient was older in age (1.09 [1.06–1.13]). There were lower odds of undergoing both LC and ERCP if patients were treated at a rural nonteaching hospital (0.42 [0.28–0.63]) compared to an urban teaching hospital or small hospital (0.39 [0.27–0.54]) compared to a large hospital (Fig. 2c).
Patients had lower odds of undergoing no procedure if they were female (0.73 [0.64–0.84]) compared to male. Patients also had lower odds of no procedure if they were younger in age (0.93 [0.91–0.95]). There were higher odds of undergoing no procedure if the patient was treated in the Northeast (1.42 [1.18–1.72]) or Midwest (1.35 [1.14–1.62]) compared to the West. Patients also had higher odds of no procedure in rural nonteaching hospitals (1.49 [1.19–1.86]) compared to urban teaching hospitals and at small hospitals (1.60 [1.33–1.93]) compared to large hospitals. Finally, patients had higher odds of no procedure if they had private insurance (1.18 [1.03–1.34]) compared to public insurance (Fig. 2d).
Discussion
Our study shows that the rate of LC for gallstone pancreatitis during index hospitalization has not changed over the last two decades. The rates of ERCP alone or both LC and ERCP have been decreasing over time, however, this was not a statistically significant trend. When LC or ERCP were performed, they occurred earlier in the hospital stay, and this trend was significant. Overall, LOS has decreased for all patients, however, the trend of decreased LOS over time was significant for patients undergoing either LC or ERCP but was not significant for patients who had neither of these interventions.
Finally, we found that females as compared to males, and patients older in age, were more likely to undergo LC during index hospitalization. Patients were less likely to undergo LC during index hospitalization if they lived in the Northeast or Midwest compared to the West, or if they were treated at a rural nonteaching hospital compared to an urban teaching hospital or small compared to large hospital. In addition, patients with private insurance compared to public were less likely to have a LC during index hospitalization.
Our study showed that 46% of patients underwent LC during the index hospitalization, which was similar to a single-center study in pediatric patients that reported a rate of 39.6%. 3 In comparison, a study out of the United Kingdom of 670 pediatric patients admitted with gallstone pancreatitis found a lower rate of LC during index hospitalization at 11.8%. 4 The rate of LC within 2 weeks of diagnosis was 26%, but overall, 20.3% of patients never had a LC. However, in that study, half of the patients who never had a LC did undergo ERCP, meaning only 10% of patients had no intervention. 4
Our study found that 35.5% of patients had no intervention for their gallstone pancreatitis, but this is difficult to compare to the 10% from the United Kingdom study because they had a median follow-up time of about 6 years, while we only evaluated the index hospitalization. The recommendation from NASPGHAN to perform LC during index hospitalization in the pediatric population was released toward the end of our study period, but the rate of LC during index hospitalization for gallstone pancreatitis has been stable for two decades. As more literature is published describing the benefits of LC during index hospitalization, we hope this will lead to more provider awareness and may improve timely management of children with gallstone pancreatitis.
As for ERCP, NASPGHAN reported that it is indicated for biliary pancreatitis but depends on local expertise. 11 Per published literature, ERCP alone is not sufficient in preventing recurrent gallstone pancreatitis.3,4 Our study shows low rates of ERCP utilization overall, which could be related to lack of pediatric expertise available, or the knowledge that treating gallstone pancreatitis with ERCP alone is not sufficient. However, the retrospective nature of this study only allows speculation on why ERCP is not common.
Multiple studies from the adult literature have shown that early cholecystectomy, typically within 48–72 hours of admission, leads to a significantly shorter LOS.13–17 Our findings in the pediatric population are congruent with the adult literature as we found that LC is occurring significantly earlier during the index hospitalization and there is a significant decrease in the trend of LOS over time. In addition to shorter LOS, the adult literature describes lower rates of ERCP usage when early cholecystectomy is performed.14,16 While the trend was not statistically significant, there was a decrease in the overall rate of ERCP use over time in our study. If these findings are similar to the adult literature, maybe the decreasing rate of ERCP use is related to the trend in earlier cholecystectomy.
Similar to our study, Blundell et al. found that adult females were more likely to undergo LC during index hospitalization for gallstone pancreatitis compared to males. 18 This study also found that patients with private insurance were less likely to undergo LC during index hospitalization. 18 This is congruent with our findings but may not be comparable as the Blundell et al. study was performed in Australia where there is universal health care with the option of private insurance coverage. In that setting, patients with private insurance may initially be treated at a public hospital but choose to have an interval LC at a private hospital. In addition, they found that patients were less likely to undergo index LC if they were treated at a low or medium volume hospital. 18
Although not a perfect comparison to our study as they looked at surgical volume rather than bedsize, this is in agreement with our findings and likely related to smaller hospitals having fewer resources and less access to surgeons. Another retrospective study by Chouairi et al. used the Nationwide Inpatient Sample Database and looked at patients undergoing LC during index hospitalization after having an ERCP for gallstone pancreatitis. 19 They also found that females were more likely to undergo LC. In contrast to our study, they found that patients younger in age were more likely to undergo LC. 19 However, this study was in the adult population, so the younger patients are likely similar to the adolescents in our study. In the adult population, the lower likelihood of undergoing LC as patients get older may be associated with higher rates of comorbidities.
Moreover, this study found that index hospitalization LC was less likely at urban teaching hospitals, which is the opposite of what we found. For adults, urban teaching hospitals may be more likely to see higher acuity patients with more comorbidities who are not great candidates for surgery during index hospitalization. For children, urban teaching hospitals are more likely to be tertiary care centers with greater access to pediatric surgery than rural nonteaching hospitals. Finally, our study found disparities in index LC based on geographic location. This indicates that practice patterns vary based on factors not related to patients' health conditions.
Our study is not without limitations. First, this was a retrospective study using a large administrative database, which inherently has limitations such as missing data and the inability to account for clinical decision making. Second, as this is an administrative database, it is difficult to elucidate if the gallstone pancreatitis was mild or severe that could influence the decision to perform an index versus interval cholecystectomy. Third, ERCP data may not be fully captured, therefore rates of ERCP may be underestimated. For example, at our freestanding children's hospital, there are no pediatric interventional gastroenterologists who perform ERCP, and our patients must be transferred across the street to the adult hospital for ERCP and transferred back to the children's hospital for cholecystectomy. The ERCP performed at the adult hospital may not be uniformly captured by all sites contributing data in this administrative database.
Finally, as KID is a sampling of pediatric discharges every 3 years, we could not evaluate rates of recurrent gallstone pancreatitis in those who did not undergo index cholecystectomy or ERCP.
Conclusions
The proportion of LC performed during index hospitalizations for children with gallstone pancreatitis has been stable for two decades. However, trends indicate that among those who undergo either LC or ERCP, interventions are occurring earlier in the hospital stay and LOS is becoming shorter. Focused efforts, including surgical provider education, may improve timely management for children with gallstone pancreatitis.
Footnotes
Authors' Contributions
A.J.R., L.H., Y.T., and M.V.R. completed the conceptualization, formal analysis, drafting, approval, and accountability. G.A.S. and A.H. contributed to critical review, approval, and accountability.
Disclosure Statement
No competing financial interests exist.
Funding Information
A.J.R. is supported on a training grant by the National Cancer Institute. Surgical Multispecialty Access to Research in Residency Training (SMART; Grant No. R38 CA245095).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.