
Abstract
Background:
Portal veinous system thrombosis (PVST) is a common complication after laparoscopic splenectomy plus esophagogastric devascularization (LSED). Anticoagulation therapy was still in debate in LSED perioperation. This study aimed to determine the postoperative risk factors of PVST, the efficacy and safety of the anticoagulation therapy after LSED procedure, and the potential impact of anticoagulation on patients' liver function and overall survival (OS).
Methods:
Three hundred patients who underwent LSED were retrospectively enrolled and analyzed in the study. The characteristics of patients, perioperative parameters, risk of PVST, and long-term follow-up data were recorded and analyzed.
Results:
One hundred eighty six of 300 patients received perioperative anticoagulation therapy (p-AT) postoperation, while 114 patients did not receive p-AT (non-p-AT). The non-p-AT group had more intraoperative blood loss, PVST, longer abdominal drain days, and postoperative hospital stays separately compared with the p-AT group. No significant difference of postoperative complications was found between the two groups. In the 1-year follow-up postoperation, both groups had great improvement in hypersplenism and the portal vein hemodynamics. During the 10-year follow-up period, the incidence of PVST was significantly higher in the non-p-AT group than in the p-AT group. Anticoagulation therapy, sex, variceal hemorrhage history, portal vein diameter, and portal vein velocity were the independent prognostic factors determined by the Cox regression analysis for PVST. The thrombosis-free survival rate (P = .002), recurrent hemorrhage-free survival rate (P < .01), and the OS rate (P < .01) were significantly lower in the non-p-AT group than in the p-AT group.
Conclusions:
The initiate use of anticoagulation therapy in postoperation of LSED is effective and safe in cirrhotic patients. The anticoagulation therapy after LSED will help decrease portal vein thrombosis, the rebleeding rate, and extend the OS of the patients, especially among women, with variceal hemorrhage history, high portal vein diameter, and low portal vein velocity.
Introduction
Laparoscopic splenectomy plus esophagogastric devascularization (LSED) has been proved to be a safe and minimal surgical trauma for decompensated cirrhotic patients with portal hypertension (PHT) in China and Japan. LSED could effectively decrease the risk of esophagogastric variceal bleeding/rebleeding, eliminate the hypersplenism, and improve the liver function.1–4 Portal veinous system thrombosis (PVST) in patients with cirrhosis is a common event with prospective incidence rates from 3.7% to 4.6% at 1 year5,6 and a range from 2% to 26% in patients awaiting liver transplantation. 7
The development of PVST in cirrhosis is associated with the low flow state of PHT, and some studies indicated that PVST was associated with the decreased survival in cirrhotic patients.8,9 It is reported that the incidence of PVST was 30%–64% after open or laparoscopic splenectomy and azygoportal disconnection, 10 and the incidence of PVST was higher in patients who underwent laparoscopic splenectomy than open splenectomy. 11 And PVST may lead to liver function deterioration, increase the portal pressure, and the risk of variceal bleeding even may cause intestinal edema and necrosis.
Severe PVST may also affect future liver transplantation. The benefit and risk of anticoagulation therapy used in cirrhotic patients with PHT were still in debate, especially during the period of perioperation. Therefore, our study aimed to determine the efficiency and safety of perioperative anticoagulation therapy (p-AT), to analyze the risk of PVST postoperation, and to estimate the effect of anticoagulation therapy on liver function, portal vein system hemodynamics, and overall survival (OS) in cirrhotic patients with PHT after LSED procedure.
Methods
Participants and surgical criteria
Three hundred sixty-four patients diagnosed with cirrhotic PHT underwent LSED from May 2011 to November 2020 in our department were retrospectively reviewed. Twenty-three patients diagnosed of liver cancer before operation, 11 patients diagnosed of PVST before operation, and 16 patients with poor data integrity were excluded. One patient died within 1 month after surgery, 11 patients lost follow-up within 3 months, and finally 300 patients were totally included (Fig. 1). All baseline patient data are summarized in Table 1. Child–Pugh classification and model for end-stage liver disease (MELD) score were used for the assessment of liver function preoperation.
Flowchart illustrating the number of patients who entered the study and the detailed patient-screening process.
The Baseline Patient Data
Bold value demonstrated its statistically difference.
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; HVPG, hepatic venous pressure gradient; MELD, model for end-stage liver disease; non-p-AT, nonperioperative-anticoagulation therapy; p-AT, perioperative anticoagulation therapy; PLT, platelet; PT, prothrombin time; RBC, red blood cells; TBIL, total bilirubin; WBC, white blood cells.
Hepatic venous pressure gradient (HVPG) and endoscopy were measured for the assessment of the risk of esophagogastric variceal bleeding. The portal vein hemodynamics data were measured by ultrasound. The size and diameter of spleen were measured by Multidetector row computed tomography (CT). Portal vein thrombosis was diagnosed by CT and ultrasound.
The surgical inclusion criteria were as follows: (1) cirrhosis with a history of variceal hemorrhage (hematemesis and melena); (2) cirrhosis with no history but a high risk of variceal hemorrhage (simultaneous grade III esophageal varices, blue varices, or cherry red spots from bleeding varices diagnosed by endoscopy, severe hypersplenism [white blood cell count <2.0 × 109/L and platelet count <50 × 109/L]); (3) high HVPG >12 mmHg. 12 Patients with severe liver dysfunction (Child–Pugh class C), PVST diagnosed preparation, and hepatocellular carcinoma were excluded. This study was approved by the Ethical Committee of Tangdu Hospital (approval no.: 202011-32).
Preoperative evaluation and surgical procedure
Multidetector row CT and Doppler ultrasound were performed to evaluate portal vein hemodynamics data, portosystemic collateral vessels, and spleen size. “Five-trocar” method of LSED operation was performed, and the specific operation steps were the same as described in our previous article. 2
The patients were encouraged to drink small amounts of water after recovery from anesthesia, and a semiliquid to soft-food diet was gradually introduced. Enoxaparin (0.4 IU twice daily) was subcutaneously injected within postoperative 48 hours if no obvious bloody abdominal drainage was observed, and the peripheral red blood cell count and coagulation function were stable.
Operative outcomes and complications
Operative outcomes including operation time, blood loss volume, conversion to open operation, postoperative hospital stay, and abdominal drain day were recorded. Postoperative complications, including intra-abdominal hemorrhage, abdominal infection, pancreatic fistula, severe ascites, encephalopathy, and reoperation, were also assessed. Postoperative morbidity was assessed according to the Clavien–Dindo classification, 13 and ≥ grade III complications were defined as serious complications.
Follow-up
All patients received anticoagulation therapy (Rivaroxaban [Bayer, AG], 15 mg, p.o., q.d.) for ∼3 months after discharge. All patients who underwent LSED would receive routine follow-up examinations. Long-term follow-up was performed using telephone or in the inpatient/outpatient departments; the last follow-up occurred on December 31, 2021. The follow-up examination included blood routine examination, coagulation function, liver function, abdominal ultrasonography, and CT. One of the primary endpoints was OS, defined as the time from surgery to death from any cause.
The other primary endpoint was recurrent hemorrhage-free survival (RHFS), defined as the time from surgery to first postoperative esophagogastric variceal bleeding. Thrombosis-free survival (TFS) was defined as the time from surgery to first diagnosed as PVST formation. Patients who died of other causes or were alive at the last follow-up date were counted as censored observations.
Statistical analysis
Continuous variables with normal distribution are expressed as mean ± standard deviation (SD), and those with non-normal distribution are expressed as the median (Q1, Q3). Normal and non-normal variables were compared using Student's t-test and the Mann–Whitney U test, respectively. Categorical variables were compared with chi-square or Fisher's exact test. The Kaplan–Meier method was used to estimate time-to-event distributions, and the log-rank test was used for comparison. Cox proportional hazard models were used to estimate the hazard ratio between the two groups.
A prognostic nomogram was formulated to the prediction of portal vein thrombosis incidence. To evaluate the prediction accuracy of the nomogram, the time-dependent receiver operating characteristic (ROC) curve, the c-index, and calibration plot were used. All data analyses were performed using SPSS 26.0 (IBM SPSS, Chicago, IL) and R software (version 4.1.2). P values were considered statistically significant at the 0.05 level.
Results
Basic characteristics of patients
One hundred eighty six of 300 patients received p-AT postoperation while 114 patients did not receive p-AT. More patients in p-AT group have history of upper gastroenterological bleeding compared with those in nonperioperative-anticoagulation therapy (non-p-AT) group (P = .003). No significant difference in other data including age, sex, body mass index, etiology, MELD score, Child–Pugh classification, blood sampling laboratory text, or hemodynamics data was found preoperation between the two groups (Table 1).
Perioperative outcomes and complications
The non-p-AT group had more intraoperative blood loss (400 [300, 450] versus 300 [200, 450]), longer abdominal drain days (5 [4, 6] versus 4 [2, 5]), and postoperative hospital stays (8 [7, 10] versus 8 [7, 9]) separately compared with the p-AT group (P = .003, P = .001, and P = .002, separately). The incidence of PVT in the non-p-AT group was much higher than that of PVT in the p-AT group (20.2% versus 8.1%, P = .002). No significant difference in postoperative complications was found between the non-p-AT group and p-AT group (Table 2).
Perioperative Data and Complications
Bold value demonstrated its statistically difference.
Grade IIIa: nonanticoagulation group (2), 2 patients received gastroscopic hemostasis; anticoagulation group (1), 1 patient received gastroscopic hemostasis.
Grade IIIb: nonanticoagulation group (4), 4 patients underwent relaparotomy for intra-abdominal bleeding; anticoagulation group (5), 5 patients underwent relaparotomy for intra-abdominal bleeding.
Grade IVa: nonanticoagulation group (2), 1 patient needed ICU management due to the renal failure and 1 patient due to the pulmonary embolism; anticoagulation group (2), 1 patient needed ICU management due to the hypotension and shock, and 1 patient due to the liver failure.
Grade IVb: nonanticoagulation group (1), 1 patient needed ICU management due to the hepatorenal syndrome; anticoagulation group (1), 1 patient needed ICU management due to the hepatorenal syndrome.
Grade V: nonanticoagulation group (2), 1 patient died of septic shock and 1 patient died of intra-abdominal bleeding within 1 month; anticoagulation group (1), 1 patient died of intra-abdominal bleeding postdischarge within 1 month.
LSED, laparoscopic splenectomy plus esophagogastric devascularization; non-p-AT, nonperioperative-anticoagulation therapy; p-AT, perioperative anticoagulation therapy.
Comparison between preoperative and postoperative data within 1 year
In the 1-year follow-up after operation, the hypersplenism in patients of the two groups was significantly improved compared with that before operation. In the p-AT group, liver function and coagulation function including alanine aminotransferase, aspartate aminotransferase, albumin, total bilirubin, and prothrombin time were significantly improved after operation.
The portal vein hemodynamics in both the groups postoperation including portal vein diameter, portal vein velocity, portal vein flow, superior mesenteric vein diameter, and superior mesenteric vein flow were all significantly improved compared with those before operation. However, the Child–Pugh classification was not greatly changed compared with that before operation (Table 3).
Preoperative and Postoperative Data in Patients of Different Groups
Bold value demonstrated its statistically difference.
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; non-p-AT, nonperioperative-anticoagulation therapy; p-AT, perioperative anticoagulation therapy; PLT, platelet; PT, prothrombin time; RBC, red blood cells; TBIL, total bilirubin; WBC, white blood cells.
Long-term follow-up
Two hundred seventy three of 300 patients (91%) were followed up with a median duration of 76.6 months (range: 1.0–129.1 months). One hundred four of the 114 patients (91.2%) in the non-p-AT group were followed up with a median duration of 87.13 months (61.70–112.73 months). In the p-AT group, the follow-up rate was 90.9% (169/186), with a median follow-up time of 69.80 months (46.23–89.47 months). During the follow-up period, 37 cases in the non-p-AT group and 16 in the p-AT group showed recurrent esophagogastric variceal hemorrhage, and there were significant differences between the two groups (P < .01).
Fifty-three cases in the non-p-AT group developed PVST, including 45 cases with portal vein thrombosis, 28 cases with splenic vein thrombosis (8 cases with splenic vein thrombosis alone), and 5 cases with superior mesenteric vein thrombosis. And in the p-AT group, 58 cases developed PVST, including 39 cases with portal vein thrombosis, 30 cases with splenic vein thrombosis (19 cases with splenic vein thrombosis alone), and 4 cases with superior mesenteric vein thrombosis. The incidence of PVST, portal vein thrombosis, and splenic vein thrombosis was significantly different between the two groups (P = .008, P = .001, P = .038).
The 1-, 3-, 5-, and 10-year TFS rates were 89.5%, 70.2%, 58.2%, and 50.8% in the non-p-AT group, respectively, versus 94.6%, 81.5%, 72.1%, and 67.5% in the p-AT group, respectively (Fig. 2A). The 1-, 3-, 5-, and 10-year RHFS rates were 85.4%, 71.9%, 66.0%, and 61.4% in the non-p-AT group, respectively, versus 94.6%, 92.4%, 92.4%, and 92.4% in the p-AT group, respectively (Fig. 2B). The 1-, 3-, 5-, and 10-year OS rates were 94.7%, 92.8%, 88.4%, and 83.2% in the non-p-AT group, respectively, versus 98.4%, 97.8%, 97.8%, and 97.8% in the p-AT group, respectively (Fig. 2C). The TFS rate (P = .002), RHFS rate (P < .01), and the OS rate (P < .01) were significantly lower in the non-p-AT group than in the p-AT group.

The Kaplan–Meier survival curve of patients with and without perioperative anticoagulation.
The risk factors and prediction of PVST in patients after LSED operation
Not receiving p-AT, cirrhosis due to HBV, low platelet count, wide portal vein diameter, and low blood velocity in the portal and splenic veins by univariate analyses were shown to be associated with worse TFS. On multivariate analysis, p-AT, sex, variceal hemorrhage history, portal vein diameter, and portal vein velocity were the independent prognostic factors for TFS (Table 4).
Prognostic Factors for Thrombosis-free Survival of Patients with LSED Procedure
Bold value demonstrated its statistically difference.
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CI, confidence interval; HR, hazard ratio; MELD, model for end-stage liver disease; LSED, laparoscopic splenectomy plus esophagogastric devascularization; PLT, platelet; PT, prothrombin time; RBC, red blood cells; TBIL, total bilirubin; WBC, white blood cells.
A nomogram for predicting TFS was constructed using the five significant prognostic factors determined by the Cox regression analysis (Fig. 3A). The time-dependent ROC curve of the nomogram at 6 months, 1, 3, and 5 years is presented in Figure 3B, with an area under the receiver operating characteristic curve of 0.708 (95% confidence interval [CI]: 0.673–0.743), 0.686 (95% CI: 0.651–0.721), 0.714 (95% CI: 0.683–0.745), and 0.699 (95% CI: 0.664–0.734). The nomogram yielded an averaged concordance index of 0.719 (95% CI: 0.660–0.778). The calibration curve showed good agreement among the estimations with the nomogram and actual observations (Fig. 3C).
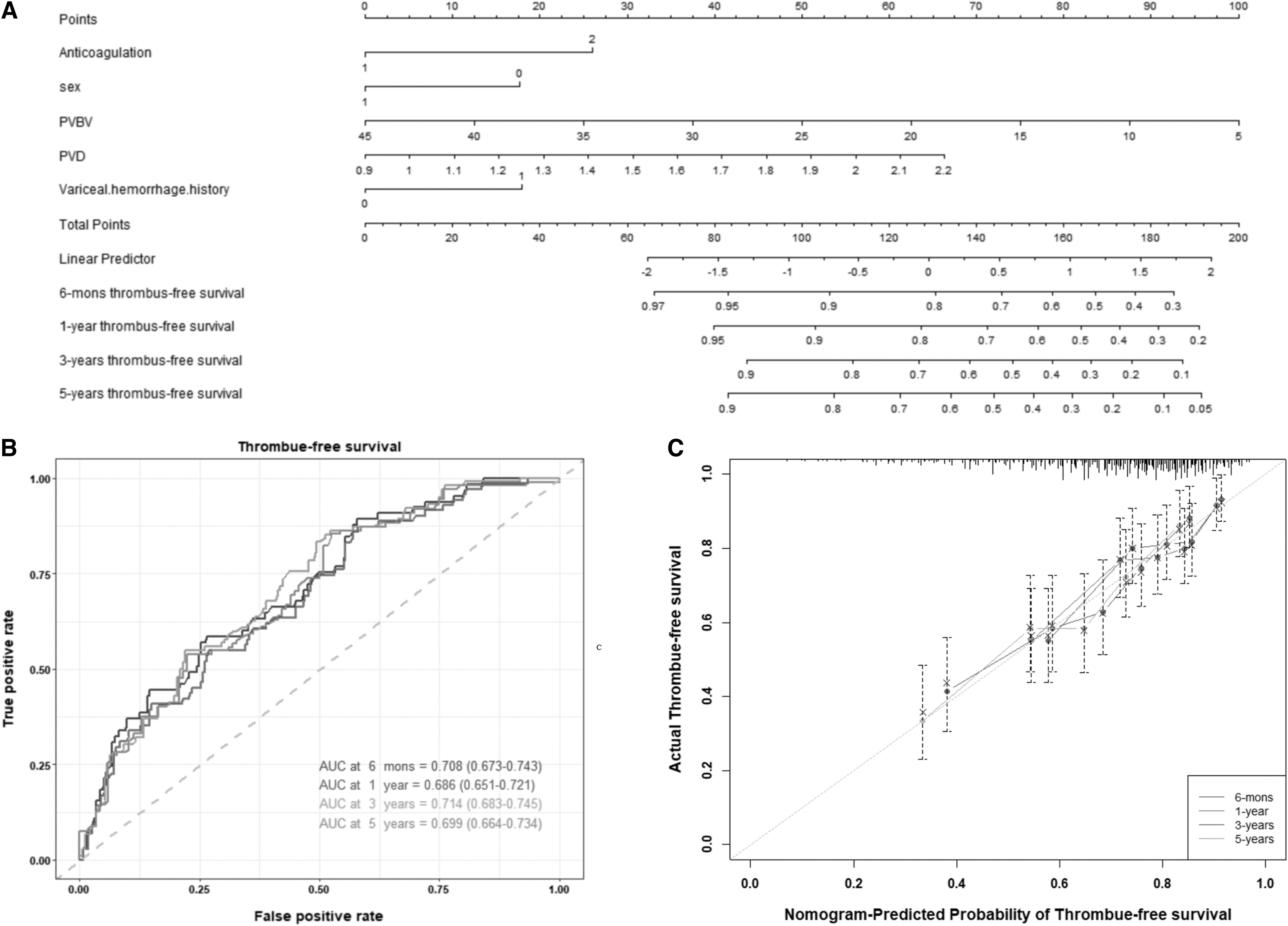
Predictive model effect verification and nomogram construction.
Discussion
PVST after splenectomy has been one of the problems concerned about. The incidence of PVST varies differently from 5% to 63%. 14 And anticoagulation is a common method to treat thrombosis, but the safety and efficiency of anticoagulation used in LSED perioperation has been few reported. Our retrospective study proved that the initial use of anticoagulation therapy perioperation of LSED is safe and could significantly decrease the incidence of PVST postoperation. It also contributed to the improvement of liver function and portal vein hemodynamics, and finally increased the OS.
LSED is a popular minimal invasive treatment for PHT in China and Japan for several reasons. Splenectomy alleviated the hypersplenism, and would decrease the portal inflow and pressure.15,16 In our study, improvement in hypersplenism postoperation was observed among patients in both the groups. And with the decrease of portal vein blood flow after splenectomy, the portal vein diameter significantly decreased, indicating the portal vein hemodynamics greatly improved. Laparoscopic devascularization eliminated the abnormal varices around the gastroesophageal fundus, thereby effectively reducing the esophagogastric rebleeding.
In addition, splenomegaly generates a lot of cytokines that accelerate liver fibrosis and liver function deterioration. Splenectomy will also help liver function improvement and decrease the incidence of liver cancer.17–20 Therefore, the liver function and portal vein hemodynamic were greatly improved postoperation in both groups.
The decrease of blood flow, hypercoagulable state, and vascular damage are the risk factors for Virchow's triad of intravascular thrombosis. Despite with a low level of platelet and poor coagulation function, patients with cirrhosis are not “autoanticoagulated” as previously we thought, but have more proportion to develop PVST than people without cirrhosis. 8 And the decrease of blood flow and vascular damage may be the main reasons contributing to PVST formation in cirrhotic patients. When having to deal with the upper gastrointestinal bleeding, endoscopic sclerotherapy, TIPS, splenectomy and portosystemic-shunt or devascularization all contribute to PVST postoperation due to venous injury and by altering portal venous flow.
Even the use of nonselective β receptor blockers was reported as a promotor for the development of PVST. 21 After LSED procedure, due to the venous injury, the portal vein blood flow decreased (because of the decrease of portal vein blood flow and the unchanged hepatic resistance, data shown in Table 3) and the platelet count increased in peripheral blood, and the application of anticoagulation became necessary to prevent the occurrence of PVST. However, anticoagulation therapy in patients with PHT has been debated for mainly concern about the increase of upper gastrointestinal hemorrhage, let alone its application used in perioperation of LSED.
It was reasonable to worry about this problem in the past. However, compared with the traditional open surgery, laparoscopic surgery has the characteristics of delicate operation, accurate anatomical operation, less intraoperative bleeding, and complete hemostasis, which greatly reduced the risk of postoperative abdominal bleeding.2,22 Therefore, the confidence and safety of p-AT were greatly strengthened.
This study also proved that anticoagulation therapy after LSED operation did not increase the postoperative complications including intra-abdominal bleeding. Furthermore, anticoagulation therapy decreased the formation of portal vein thrombosis leading to the improvement of portal vein system, and contributed to the less abdominal drain day and less postoperative discomfort, and finally shortened the hospital stay.
This study demonstrated several risk factors for PVST after LSED procedure. Patients without perioperative prophylactic anticoagulant therapy have a significantly increased risk of PVT in the future, even though the non-p-AT group also received anticoagulation therapy for 3 months after discharge. Early anticoagulant therapy is in accordance with the prevention principles of peripheral venous thrombosis. 23 Enoxaparin, usually used in preventing and treating peripheral venous thrombosis, was also shown to be safe and effective in PVT in cirrhotic patients, and was appeared to improve liver function and improve survival. 24
In this study, the initiation of perioperative anticoagulation was shown safe and effective in preventing PVT. Although the risk does not differ by sex in venous thromboembolism, 25 women after LSED are more likely to form PVST. Although there are no reports that women are more likely to develop PVST, it is well established that estrogen can increase the risk of both arterial and venous thrombosis. 26 And some reports showed that women taking estrogen-containing pills had an increased venous thrombosis in the mesenteric vasculature and portal vein.27,28
The decrease in estrogen clearance caused by liver cirrhosis may lead to more estrogen in women with liver cirrhosis than in men, and thus women may be more prone to thrombosis, but further research is needed. Having variceal hemorrhage history, large portal vein diameter, and low portal vein velocity are the risk factors increasing the occurrence of PVST postoperation. In fact, these three risk factors are associated with the degree of cirrhosis and PHT.
Although the prevalence of PVST in cirrhosis varies among studies, it increased in parallel with the severity of cirrhosis according to the epidemiological results. It was reported that ∼10% in patients with compensated cirrhosis, 17% in patients with Child B/C cirrhosis, and up to 26% in liver transplant candidates were observed developing PVST. 29 And these five significant prognostic factors were consistent with the nomogram and actual observations.
In our follow-up analysis, the LSED procedure combined with the p-AT contributed to the decrease of the 1-, 3-, 5-, and 10-year TFS, RHFS, and OS. Studies indicated that increased intrahepatic resistance in liver cirrhosis usually leads to the occurrence of microthrombosis in hepatic sinuses.30,31 And there is no doubt that microthrombi will lead to the increase of portal pressure and aggravate intrahepatic ischemia and hypoxia, eventually accelerating hepatocellular necrosis and fibrogenesis.
It was reported 32 that anticoagulation therapy contributed to liver function and renal function improvement in cirrhotic patients. Besides that, enoxaparin could reduce the bacterial translocation by improving intestinal microcirculation. The liver function in p-AT group was improved more obviously postoperation within 1 year. Therefore, anticoagulation represents a safe, effective, and reliable option for patients with cirrhosis PVT, even those with poor liver function.
Limitation
The main limitation of this article is a single-center, retrospective study design.
Conclusion
The initial use of p-AT in LSED procedure is effective, safe, and necessary in cirrhotic PHT patients. No p-AT, women, variceal hemorrhage history, high portal vein diameter, and low portal vein velocity are the risk factors of PVST after postoperation. The p-AT after LSED procedure will help decrease portal vein thrombosis, the rebleeding rate, and extend the OS of the patients.
Footnotes
Authors' Contributions
D.W. contributed to conceptualization, writing—review and editing, and supervision. X.C. and L.L. were involved in software, data curation, writing—original draft, writing—review and editing, and visualization. T.Y., B.H., and Y.C. carried out data curation and writing—review and editing. J.L. took charge of writing—review and editing. J.Y. was in charge of conceptualization, methodology, software, formal analysis, writing—review and editing, and visualization.
Disclosure Statement
No competing financial interests exist.
Funding Information
The article is supported by the National Natural Science Foundation of China (81700533), the Key Research and Development Program of Shaanxi Province, China (2017SF-116), and the Youth Independent Innovation Science Foundation of Tangdu Hospital (2023CTDQN008).