
Abstract
Background:
Postoperative gastrointestinal fistula (PGF) is one of the main causes of abdominal infection and perioperative death. This study was designed to investigate the risk factors of PGF, anastomotic fistula (AF), and duodenal stump fistula (DSF) for patients who underwent radical distal gastrectomy.
Materials and Methods:
In this retrospective observational study, 2652 gastric cancer cases who received radical distal gastrectomy from 2010 to 2020 were selected as research subjects. Subsequently, we adopted the univariate and multivariate logistic regression analysis as statistical method to screen the risk factors for PGF, AF, and DSF, respectively.
Results:
In univariate analysis, gender (P = .022), operative time (P = .013),
intraoperative blood loss (P < .001), tumor diameter (P = .002), and tumor stage (P < .001) were related to PGF. Multivariate logistic regression analysis identified the male (odds ratio [OR] = 2.691, P = .042), massive intraoperative hemorrhage (OR = 1.002, P = .008), and advanced tumor (OR = 2.522, P = .019) as independent predictors for PGF. Moreover, diabetes (OR = 4.497, P = .008) and massive intraoperative hemorrhage (OR = 1.003, P = .010) were proved to be associated with AF, while massive intraoperative hemorrhage (OR = 1.001, P = .050) and advanced tumor (OR = 6.485, P = .005) were independent risk factors of DSF.
Conclusions:
The gender, intraoperative hemorrhage, tumor stage, and diabetes were expected to be used as predictors of PGF for radical distal gastrectomy.
Introduction
At present, the comprehensive treatment based on radical surgery is the main therapy mode for gastric cancer patients to obtain ideal prognosis.1,2 With the continual progress of perioperative techniques and surgical instruments, the surgical effect for gastric cancer has improved significantly, but early postoperative complications such as postoperative bleeding, digestive tract fistula, and abdominal infection are still common. 3 Postoperative gastrointestinal fistula (PGF), including anastomotic fistula (AF) and duodenal stump fistula (DSF), is one of the main causes of abdominal infection and perioperative death. In addition, the occurrence of PGF can significantly prolong hospital stay, increase hospitalization expense, and affect long-term efficacy.4–7
According to previous studies, the incidence of PGF for gastric cancer surgery varied greatly (0%–15.0%).8,9 The fever, abdominal pain, peritoneal irritation, and even septic shock caused by intraperitoneal infection were the main clinical manifestations of PGF. PGF could be diagnosed by computerized tomography, gastrointestinal endoscopy, or gastroenterography examination combined with clinical manifestations. Moreover, the cause of PGF was complex and multifaceted, and the following etiologies may work: (1) impaired intestinal blood flow around the anastomosis, (2) infection around the anastomosis or in the abdominal cavity, (3) excessive anastomotic tension or twisted bowel, and (4) poor nutritional status and poor tissue regeneration ability of patients.5,10
At present, the risk factors of PGF are still not very clear. Liu's study revealed that serum C-reactive protein and albumin on postoperative day 4, neutrophil/lymphocyte ratio, and systemic immune-inflammatory index with significant relevance to postoperative AF show that perioperative immunonutritional index could act as an indicator for AF. 11 Xing et al. found that age and alcohol consumption were independent risk factors of AF, 5 while Tu's study showed that AF was more prevalent in patients with age ≥65 years, hemoglobin ≤8.0 g/dL, and malnourishment. 9 Moreover, in Orsenig's study, heart disease, liver cirrhosis, bio-humoral nutritional status impairment, blood losses >300 mL, and absence of manual reinforcement over duodenal stump were found to be independent risk factors for DSF development. 12 Published studies, however, covered all types of gastrectomy and included few participants, and detailed analysis that performed solely for distal subtotal gastrectomy was lacking.5,7,9,13 This retrospective observational study was designed to investigate the risk factors of PGF, AF, and DSF by analyzing the case data from the First Medical Center of Chinese People's Liberation Army (PLA) General Hospital.
Materials and Methods
Study participants
Gastric cancer cases treated at the First Medical Center of the Chinese PLA General Hospital from January 2010 to December 2020 were screened. Related cases meeting the following criteria were selected as research subjects: (1) age ≥16 years; (2) no evidence of tumors invading the adjacent organs or distant metastasis; (3) underwent radical distal gastrectomy, whatever open, laparoscopic, or robot-assisted surgery; and (4) a histologically confirmed adenocarcinoma of the stomach. The study was reviewed and approved by the Medical Ethics Committee of the First Medical Center of the Chinese PLA General Hospital.
Data collection and outcome evaluation
The case data needed to be collected were as follows: gender, age, body mass index (BMI), preoperative level of hemoglobin (HGB) and albumin (ALB), disease course, neoadjuvant chemotherapy application, preoperative pyloric obstruction (diagnosed according to gastroscopy or upper gastroenterography, combined with clinical symptoms), diabetes, significant preoperative weight loss, abdominal operation history, preoperative American society of Anesthesiologists (ASA) score, operative time, intraoperative bleeding, surgical approach, application of jejunum nutrition tube and intraperitoneal chemotherapy drug, transfer to intensive care unit, tumor diameter, and tumor stage (based on eight tumor node metastasis classification staging standard of gastric cancer).
The diagnosis of PGF relied mainly on radiological and/or clinical findings. In the present study, patients diagnosed as PGF meet at least the condition (1) + (2): (1) digestive tract angiography showed that the contrast medium flowed into the abdominal cavity through the fistula, or a fistula was seen using gastrointestinal endoscopy; (2) leakage of intestinal fluid or turbid content from the surgical drain; and (3) accompanied by clinical symptoms such as fever, abdominal pain, peritoneal irritation, elevated leukocyte count, or septic shock.
Statistical analyses
All statistical analyses were performed using SPSS software (version 26.0). For continuous variables, column diagrams were drawn to test the normal distribution, and mean ± standard deviation or median (interquartile range) was calculated to illustrate the data, while independent-samples t-test or Mann–Whitney U test was used for intergroup comparison. Categorical data were depicted as numbers (percentages) and compared using the two-sided Chi squared test. Subsequently, univariate and multivariate binary logistic regression analyses were conducted to determine the predictors of PGF, AF, and DSF, respectively, and variables with a P < .1 in the univariate analysis would be included in the multivariate analysis. Variables with a P < .05 in the multivariate analysis were considered as independent predictors.
Results
Patient characteristics
After screening, 2997 in-hospital cases at the study center between January 2010 and December 2020 were retrieved using the electronic medical records system.
Of these patients, 187 underwent palliative surgery or combined with other organ resection, 7 died during hospitalization, and 151 had incomplete or no cancerous pathological reports. Ultimately, 2652 cases were selected as research subjects in this analysis.
There were 1834 males and 818 females, with a mean age of 57.68 (range: 17–89) years. PGF was diagnosed in 37 (1.4%) patients during postoperative hospitalization, containing 14 AF and 23 DSF cases. Of the 37 patients, 31 patients recovered with conservative treatment, 6 patients underwent surgery, and no patient died in hospital. Subsequently, 2652 cases were divided into the PGF (n = 37) and control group (n = 2615) for further analysis (Fig. 1). Compared with the control group, the PGF group tended to have two or more abdominal drainage tubes (51.4% versus 27.8%, [P = .002]), and experience prolonged gastrointestinal decompression time (5[4, 6] days versus 5[3, 6] days, [P = .054]).
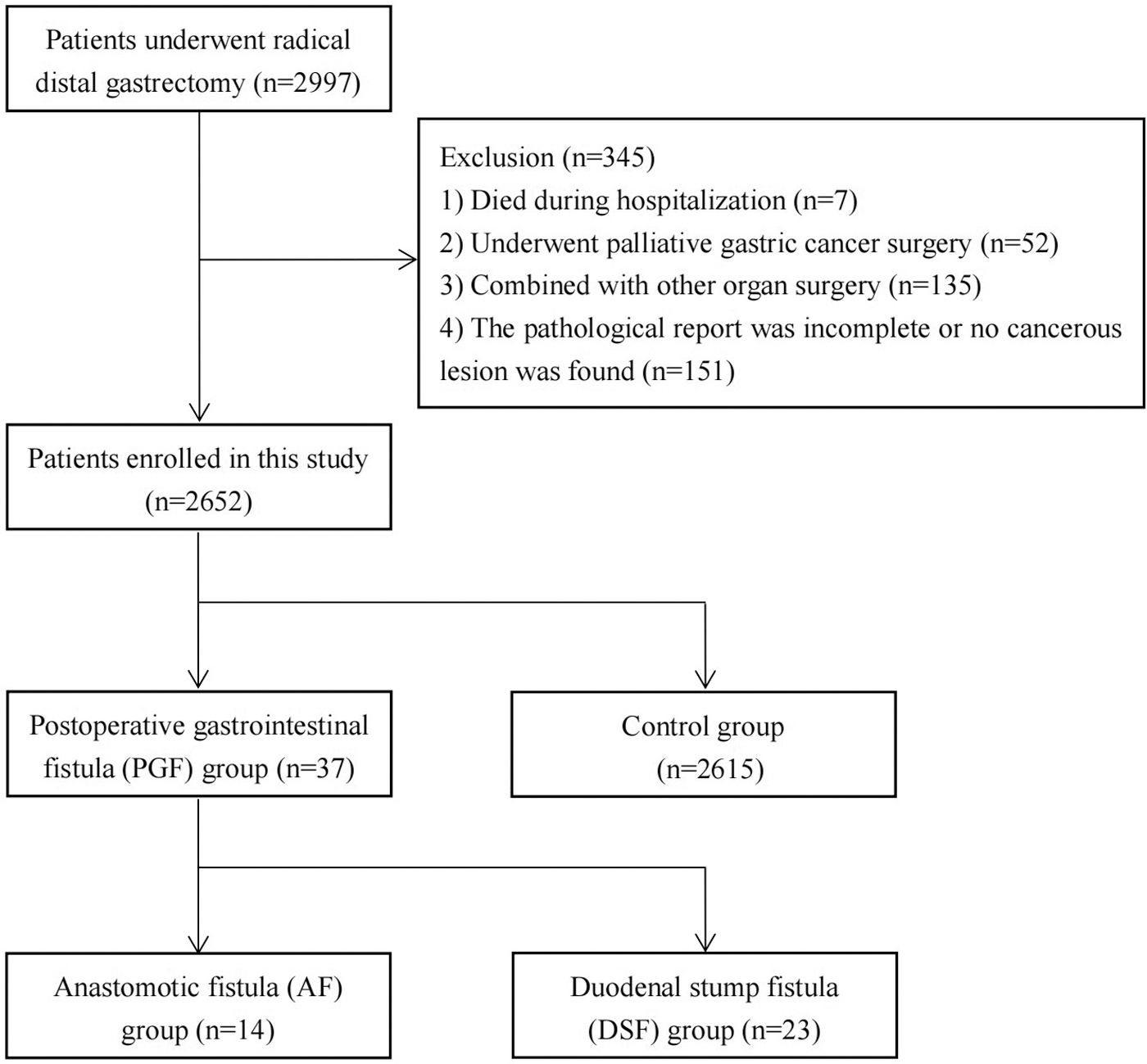
The flowchart of patient selection.
Univariate analysis for PGF
Univariate analysis showed that gender (P = .022), operative time (P = .013), intraoperative blood loss (P < .001), tumor diameter (P = .002), and tumor stage (P < .001) were predictive factors for PGF (Table 1). Based on clinical experience and literature reports, continuous variables such as age, BMI, and preoperative HGB and ALB levels were transformed into dichotomous outcomes. The converted variable results were as follows: age (>65 or ≤65 years), BMI (>28 or ≤28 kg/m2), preoperative HGB level (≤90 or >90 g/day), and preoperative ALB level (<35 or ≥35 g/day). In addition, receiver operating characteristic curves for operative time, intraoperative blood loss, and tumor diameter were drawn, then dichotomous outcomes, including operative time (>199.5 or ≤199.5 minutes), intraoperative blood loss (>270 or ≤270 mL), and tumor diameter (>4.9 or ≤4.9 cm), were obtained based on cutoff values. In this study, intraoperative blood loss >270 mL was considered as massive hemorrhage. Of these converted variables, operative time (>199.5 or ≤199.5 minutes; P = .024), intraoperative blood loss (>270 or ≤270 mL; P < .001), and tumor diameter (>4.9 or ≤4.9 cm; P < .001) were still associated with PGF.
Characteristics of Included Patients in Postoperative Gastrointestinal Fistula Group and Control Group
Bold values indicate a statistical difference (P < .05).
Data are reported as numbers (percentage), mean ± standard deviation, or the median (quartile).
ALB, albumin; BMI, body mass index; HGB, hemoglobin; ICU, intensive care unit; PGF, postoperative gastrointestinal fistula.
Multivariate analysis for PGF
A multivariate binary logistic regression model was constructed based on variables before converting (gender, operative time, intraoperative blood loss, tumor diameter, and tumor stage), and analysis results revealed that the male (odds ratio [OR] = 2.691, P = .042), massive intraoperative bleeding (OR = 1.002, P = .008), and advanced tumor (OR = 2.522, P = .019) were independent risk factors of PGF (Table 2).
Multivariate Analysis of Risk Factors Associated with Postoperative Gastrointestinal Fistula
Bold values indicate a statistical difference (P < .05).
CI, credible interval; OR, odds ratio.
Logistic regression analysis for AF and DSF
Of the 37 PGF cases, 14 were AF cases (Billroth I anastomosis), and 23 were DSF cases (Billroth II or Roux-en-Y gastrojejunostomy). Subsequently, we investigated the risk factors of AF and DSF, respectively. Univariate analysis based on 1079 Billroth I anastomosis cases revealed that diabetes (OR = 4.727, P = .006) and intraoperative blood loss (OR = 1.003, P = .008) were associated with AF. Multivariate analysis showed that diabetes (OR = 4.497, P = .008) and massive intraoperative hemorrhage (OR = 1.003, P = .010) were also the independent risk factors (Table 3).
Univariate and Multivariate Logistic Analyses of Risk Factors for Anastomotic Fistula (Billroth I)
Bold values indicate a statistical difference (P < .05).
ALB, albumin; BMI, body mass index; CI, credible interval; HGB, hemoglobin; ICU, intensive care unit; OR, odds ratio.
Moreover, univariate and multivariate logistic regression analyses for DSF were performed using the 1573 Billroth II or Roux-en-Y gastrojejunostomy cases. Univariate analysis identified the operative time (OR = 1.009, P = .006), intraoperative blood loss (OR = 1.002, P = .003), tumor diameter (OR = 1.276, P = .001), and tumor stage (OR = 8.756, P < .001) as predictors, while multivariate analysis showed that massive intraoperative hemorrhage (OR = 1.001, P = .050) and advanced tumor (OR = 6.485, P = .005) were independent risk factors (Table 4).
Univariate and Multivariate Logistic Analyses of Risk Factors for Duodenal Stump Fistula (Roux-en-Y and Billroth II)
Bold values indicate a statistical difference (P < .05).
ALB, albumin; BMI, body mass index; CI, credible interval; HGB, hemoglobin; ICU, intensive care unit; OR, odds ratio.
Discussion
PGF, as one of the most common and serious complications of gastrectomy, has multifactorial etiologies. The improvement of preoperative preparation and surgical skills are the keys to prevent the occurrence of PGF.11,12,14 In this study, risk factors associated with PGF, AF, and DSF were identified, aiming to provide a basis for clinical practice. As analysis results showed, male, massive intraoperative hemorrhage, and advanced tumor tended to be the independent risk factors of PGF. Furthermore, diabetes and massive intraoperative hemorrhage were proved to be associated with AF, while massive intraoperative hemorrhage and advanced tumor were independent risk factors of DSF.
Tumor necrosis factor can be released in large quantities during tumor growth, which enhances local inflammatory response. Advanced tumors are accompanied by extensive expansion area and more serious inflammatory reaction, and this could be an important reason for the occurrence of PGF. 15 Besides, advanced cancers (stage III-IV A) are associated with deeper invasion and more lymph node metastases, resulting in increased difficulty in tumor resection, lymph node dissection, and digestive tract reconstruction. Excessive resection of the digestive tract may lead to excessive tension and delayed healing of anastomosis after reconstruction.16,17 Difficult surgery is usually accompanied by enlarged tissue damage, prolonged operation time, and increased intraoperative blood loss. The prolonged exposure time may increase the risk of intestinal edema and infection, and the enlarged tissue damage also increases the possibility of postoperative local infection and gastrointestinal nutrient vascular injury, thus increasing the risk of anastomotic leakage. 18 Furthermore, the application of an abdominal drainage tube can not only lead to gastrointestinal edema, spasm, or paralysis through stimulating effect but also increase the probability of abdominal infection due to foreign body effect and reflux of drainage fluid.
Massive intraoperative bleeding is another important risk factor of PGF. On the one hand, massive hemorrhage during an operation could cause ischemia of the gastrointestinal canal around anastomosis and duodenal stump, resulting in delayed healing and even gastrointestinal necrosis. On the other hand, anemia, hypoproteinemia, and malnutrition easily lead to tissue edema and infection, which was not conducive to granulation tissue growth.9,12 For these reasons, massive hemorrhage increases the risk of PGF. According to previous studies, patients with diabetes were also more likely to develop PGF after gastrointestinal surgery. The following reasons could contribute to this phenomenon. First, diabetic patients are in an immune-stress state for a long time due to systemic inflammatory reaction, the body's resistance is decreased, and the phagocytosis ability of cells is weakened, leading to slow regeneration of anastomotic granulation tissue. Second, diabetic patients are often accompanied by microangiopathy and then causes increased wound exudation, infection, and delayed healing. Third, owing to surgical stimulation, postoperative fasting, and parenteral nutrition support, the blood glucose fluctuation of diabetic patients is large, which is also not conducive to the healing of anastomosis.19,20 In addition, this analysis showed that postoperative gastroparesis syndrome was more common in male patients, and discrepancies in hormone levels, lifestyle habits, and adherence may play roles.20,21
Before radical gastrectomy, therefore, it is necessary to conduct a comprehensive investigation on the clinical data of patients and carefully evaluate the tumor stage. 22
For patients with underlying diseases such as diabetes and malnutrition, the physical quality should be actively improved during the perioperative period. For diabetic patients with unsatisfactory blood glucose control, preoperative endocrinology consultation should be requested to adjust medication, perioperative blood glucose changes should be closely monitored, and the dosage of parenteral nutrition insulin should be appropriately increased. For patients with poor nutritional status and need to fast, nutritional assessment (NRS 2002 score) should be carried out before surgery, and nutrients and electrolytes needed by the body should be timely supplemented through parenteral nutrition. In addition, serum potassium ion levels should be paid special attention. Although no correlation was found between preoperative HGB or ALB levels with PGF, perioperative anemia or hypoalbuminemia should be corrected in time to improve body tolerance and promote anastomotic and wound healing. The operation should be carried out under the condition of stable control of underlying diseases and good nutritional status. Furthermore, prudent surgical manipulation should be taken to prevent unnecessary damage to blood vessels and nerves, thus reducing intraoperative bleeding and shortening operation time. 23 After surgery, the indwelling of the abdominal drainage tube should be minimized, and the anti-inflammatory and anti-infection treatment should be emphasized to promote tissue healing and reduce the risk of PGF. In this study, patients received routine intravenous antibiotics and regular blood routine examination, and the antibiotic grades were adjusted based on blood test results. If necessary, abdominal drainage was sent for bacterial culture and then adjusted the antibiotic regimen according to the results of bacterial culture. Besides, the drainage bag was replaced daily, and the surgical incision was disinfected and changed regularly to avoid abdominal infection.
In this study, 31 PGF patients recovered with conservative treatment, and 6 underwent surgery. The therapeutic method of PGF includes conservative, surgical, and endoscopic treatment. With the continuous innovation of diagnosis and treatment technology and concept, conservative treatment has achieved satisfactory therapeutic effect and has become the main treatment mode of PGF, including smooth drainage and infection control, control of digestive tract leakage, and reasonable nutritional support. For PGF cases that are difficult to heal with conservative treatment, fistula repair, closure or digestive tract reanastomosis should be performed by surgical or endoscopic treatment. In addition, PGF cases with large fistula diameter are often accompanied by a large amount of digestive fluid leakage, which can result in serious abdominal infection and make the patient's condition deteriorate rapidly in a short time. For the above cases, reoperation should be performed to repair the fistula, remove the abdominal fiber tissue diaphragm, and thoroughly irrigate the abdominal cavity, so as not to miss the best treatment opportunity to lead to the deterioration of the patient's condition or even death.6,7,23
Although we collected abundant cases of radical distal gastrectomy and investigated the predictors of PGF, AF, and DSF, there remain limitations. First, management and technical difference in retrospective observational study limited the level of evidence. Second, because PGF is clinically rare, a limited number of PGF cases were included, reducing the power of the analysis. In the future, multicenter prospective studies with large sample are supposed to be conducted.
Conclusions
Male, massive intraoperative hemorrhage, and advanced tumor were risk factors closely related to the occurrence of PGF. Furthermore, diabetes and massive intraoperative hemorrhage were proved to be associated with AF, while massive intraoperative hemorrhage and advanced tumor were independent risk factors of DSF. This study identified the risk factors of PGF, AF, and DSF for radical distal gastrectomy, which could be further applied in clinical practice.
Footnotes
Acknowledgment
The authors thank all patients whose data were used for the study.
Authors' Contributions
Conception and design: N.L., Z.Y., and P.L.; Administrative support: N.L. and P.L.; Provision of study materials or patients: Z.Y., Y.G., and X.Z.; Collection and assembly of data: Y.G. and J.Y.; Data analysis and interpretation: Y.S., X.Z., J.Y., and N.L.; Article writing and editing: Z.Y., Y.S., P.L., and N.L.; Final approval of article: All authors.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The retrospective study was reviewed and approved by the Medical Ethics Committee of the First Medical Center of the Chinese People's Liberation Army (PLA) General Hospital. Because this study does not involve patient intervention, information disclosure, and long-term follow-up, informed consent was not required.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.