
Abstract
Objective:
To determine the importance of a critical view of safety (CVS) techniques and Rouviere's sulcus (RS) in laparoscopic cholecystectomy (LC) and its relation to biliary duct injuries (BDIs) and to determine the frequency and the type of RS.
Design, Setting, and Participants:
A descriptive study was carried out among 76 patients presenting to the surgery department of a tertiary care center in Nepal. The study population included all patients in the age group 16–80 years undergoing LC.
Outcome Measures:
The main outcome of interest was to calculate the percentage of BDIs along with the frequency and the type of RS.
Results:
A total of 76 patients were enrolled in the study, out of which 57(75%) were female patients with a male-to-female ratio of 1:3 and a mean age of 45.87 ± 15.33 years. Seventy-one (93.4%) patients were diagnosed with symptomatic gallstone disease. The CVS was achieved in 75 (98.7%) of the cases, whereas in 1 case, the CVS could not be achieved, and in the same patient routine LC was converted into open cholecystectomy owing to the difficult laparoscopic procedure. In 56 (73.7%) cases, RS was first visible to the operating surgeons after port installation, alignment, and adequate traction of the gallbladder; in 20 (26.3%) cases, RS was not originally apparent.
Conclusion:
According to the findings of this study and the literature's critical assessment of safety, this method will soon become a gold standard for dissecting gall bladder components. The technique needs to be extended further, especially for training purposes. Major difficulties can be avoided by identifying RS before cutting the cystic artery or duct during LC.
Introduction
Cholecystectomy is one of the most common abdominal surgical procedures performed today, of which >80% is performed laparoscopically.1,2 Prof. Dr. Erich Mühe of Germany performed the first laparoscopic cholecystectomy (LC) in 1985. 3 Currently LC is the gold standard for the management of gallstones. 4
Since LC was introduced, it has gained favor due to its advantages over open cholecystectomy (OC), such as less postoperative discomfort and a shorter hospital stay. However, the incidence of biliary duct injury (BDI), a potentially fatal consequence, increased along with this. Compared with an average of 0.2% in OC,5,6 the incidence of BDI encountered a drastic increase after the introduction of LC, with reported rates of up to 1.5%.7–13
Three main risk factors have been identified, which increase the risk of biliary tree trauma, and these include a surgeon's experience, an inflammatory process, and biliary anatomical variations.14,15
Most surgeons initially acquired their knowledge of LC through 1–3 years of postgraduate study and frequently implemented it into their practices without supervision. Consequently, many surgeons became anatomically confused during the first several procedures, unwittingly transecting the bile duct early in the dissection. 16
Since the incorporation of training of LC in the residency program, outcomes in terms of BDI have been excellent, 17 though longer operating times for LC were often reported when residents performed the operation.18,19 Recent reports show that residents are now performing LC with equivalent safety and in equal time as their attending, and often in patients who are less healthy than were previously operated on laparoscopically.20,21
Other studies that attributed the outcome to surgeons' learning curve later concluded that patient number and operator experience did not significantly decrease the incidence of BDI.12,22 Since then, considerable effort has been made to improve safety in LC with a variety of methods described in the literature, reducing the incidence of BDI to ∼0.23% and 0.30%.23,24
The vast majority of reported BDIs result from the misidentification of the common bile duct (CBD) as the cystic duct (CD).25,26 As a result, several different methods have been described regarding CD dissection. 6 These techniques include the infundibular approach, “fundus down” method, hepatic hilum exposure, intraoperative cholangiography, identification of Rouviere's Sulcus (RS), and “critical view of safety” technique.
The “critical view” technique, which recognizes the cystic and CBD junction intraoperatively, the “infundibular” technique, which recognizes the CD and gallbladder junction, and the routine use of intraoperative cholangiography are the techniques that, at least theoretically, aim to reduce the risk of such injuries. The aim of all these techniques is to establish an undisputable surgical method that could clearly distinguish the anatomical structures of that area in an objective way, unbiased by subjective delusions. 6
Strasberg was the first to coin the term “critical view of safety” in 1995, and this approach to the identification of cystic structures has been accepted as the gold standard technique to reduce biliary tract injury. 27
RS is an important extra biliary landmark for safe dissection of Calot's triangle during LC. RS is a 2–5 cm sulcus extending to the right of the liver hilum anterior to the caudate lobe. The sulcus ascertains the plane of the CBD exactly. It can be recognized in 80% of cases. 28
BDIs during LC remain an important cause of morbidity, mortality, increased hospital stay, and litigation.15,25 Since the introduction of laparoscopic surgery in early 1990, their reported rate, which ranges from 0.3% to 0.5%, has not altered significantly. 26 By conducting this study, we can find out the role of critical view of safety (CVS) and RS, and BDIs in LC. The crucial elements of using this helpful landmark in safe laparoscopic surgery are covered in this article, along with potential hazards wherein the landmark may not be present or may be misinterpreted. The sulcus is made more visible by the helpful acronym “RANGERS”—Rouviere's at Neck of Gallbladder Eases Recognition of Structures—which enables safer LC.
All laparoscopic cholecystectomies should ideally be performed with strict use of the “critical view” approach, which makes it easier to identify the anatomic components that should be divided.
The objective of this study is to determine the importance of CVS techniques and RS in LC and its relation to BDIs and to determine the frequency and the type of RS.
Materials and Methods
Study setting
This was a descriptive study carried out in a tertiary care center in Nepal (Department of General Surgery, B.P. Koirala Institute of Health Sciences, Dharan).
Study population
The study population included all patients in the age group 16–80 years undergoing LC in B.P. Koirala Institute of Health Sciences, Dharan. Patients, <16 years of age and those willing to undergo OC were not included. Patients who were diagnosed with complicated gallstone disease preoperatively were excluded.
Calculation of the sample size and sampling technique
The study considered a 95% confidence interval. For this purpose, the study considered the prevalence of BDI as 0.5%. Now we can use the following formula to estimate the sample size.
where N = estimated sample size to be calculated,
zb = 0.842 at 80%power,
za/2 = 1.96 at 95% CI,
p = p1+p2/2,
q = 1-p,
p1 = 0.8,
p2 = 0.95, and
P = .875.
Using the formula, N is nearly equal to 76.
The first 76 cases who met the inclusion criteria of the study and consented to be part of the study were enrolled.
Outcome measures
The main outcome of interest was to calculate the percentage of BDIs along with the frequency and the type of RS.
Enrollment of the patients
All patients undergoing LC in BPKIHS, Dharan, were enrolled in the study. Informed and written consent was taken from all the patients willing to participate in the study. Demographic data were recorded in the proforma sheet.
Operative technique
After general anesthesia, port placement, positioning, and proper gall bladder traction, Calot's triangle was dissected anteriorly and posteriorly to achieve a CVS in both anterior and posterior aspects (Douplet View), that is, two structures seen entering the gall bladder and lower one-third of gall bladder separated from the liver to expose the cystic plate. RS was spotted, whether or not it was originally evident to the operating surgeon. If RS was not originally apparent, the likely cause (such as omental/bowel adhesion, lack of RS, or liver cirrhosis) was recorded, and in the case of an adhesion, whether RS became evident before splitting the cystic artery/duct or not was documented on the release of the adhesion.
The operating surgeon made a note of the RS features (in terms of its type: open sulcus/closed sulcus/slit/scar; orientation: oblique/horizontal) in the RS visible group (either initially or postadhesion release). By comparing the breadth and depth of the RS with the typical distance between the tips of two dissecting forceps' jaws, the dimensions of the RS were assessed intracorporeally. A sulcus was referred to be a deep sulcus if it was sufficiently wide and deep (centimetrically). The deep sulcus' openness or closure was also noted, depending on whether its medial end was open toward the porta hepatis, allowing the portal structures to be seen, or closed toward the porta hepatis.
The term “slit sulcus” refers to a sulcus that is only detectable along its length because it lacks sufficient depth and width (subcentimetric). The likely cause (such as the lack of RS, liver cirrhosis) was recognized in the case of invisible RS even on the release of adhesion.
Statistical analysis
Data were entered into Microsoft Excel and converted into Statistical Package for Social Science (SPSS) for statistical analysis by using SPSS V.11.5. Descriptive statistics were calculated as percentage, mean, standard deviation, median, and interquartile range.
Ethical consideration
The ethical clearance was taken from the institutional review committee of B.P. Koirala Institute of Health Sciences, Dharan, Nepal. The patients were explained the purpose of the study and were also assured that the study was anonymous and the participation was voluntary, then the informed verbal consent was taken.
Patient and public involvement
There was no patient and public involvement in the design, conduct, reporting, or dissemination plans of our research.
Results
A total of 76 patients were enrolled in the study.
Age distribution
The age of the patients enrolled in the study ranged from 19 to 74 years with a mean age of 45.87 ± 15.33 years. The majority were in the range of 31–40 years of age (Fig. 1).
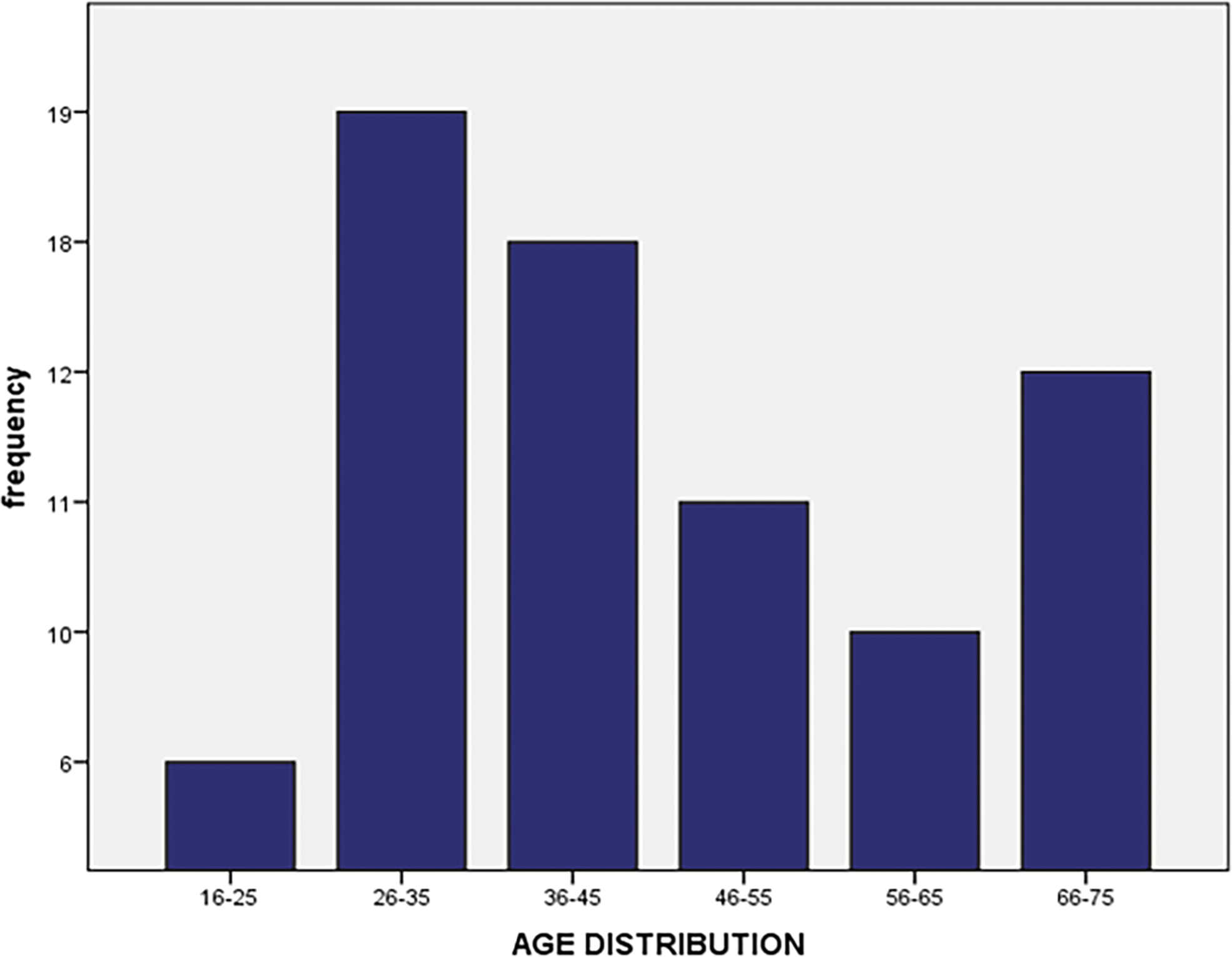
Distribution of patients in different age groups.
Gender
In our study, 19(25%) were male patients and 57(75%) were female patients. The ratio of male to female was M:F = 1:3 (Fig. 2).
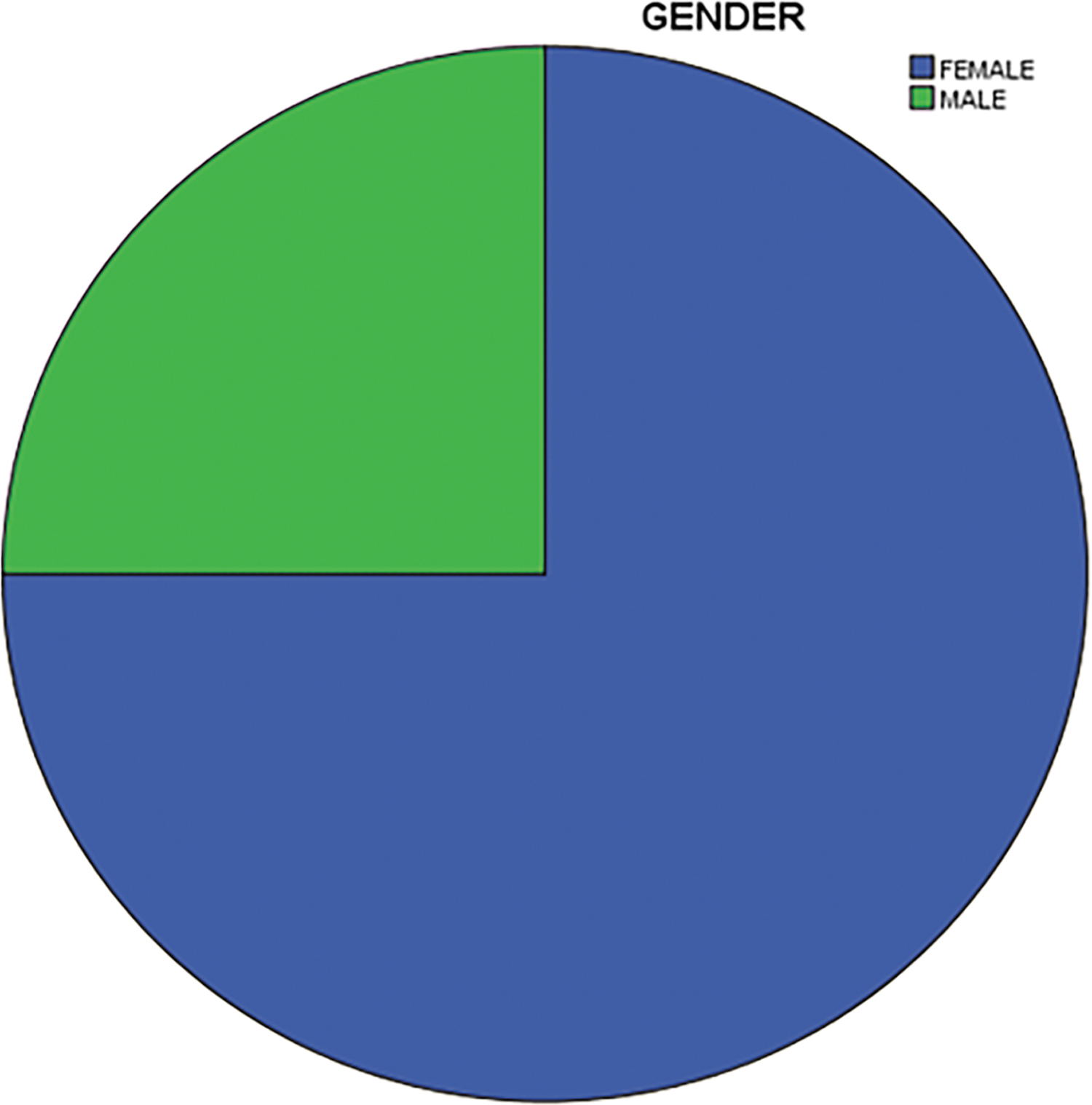
Sex-wise distribution of patients.
Distribution of patients based on districts
The majority of patients were from the Sunsari district (48.7%) followed by Morang (11.8%; Fig. 3).
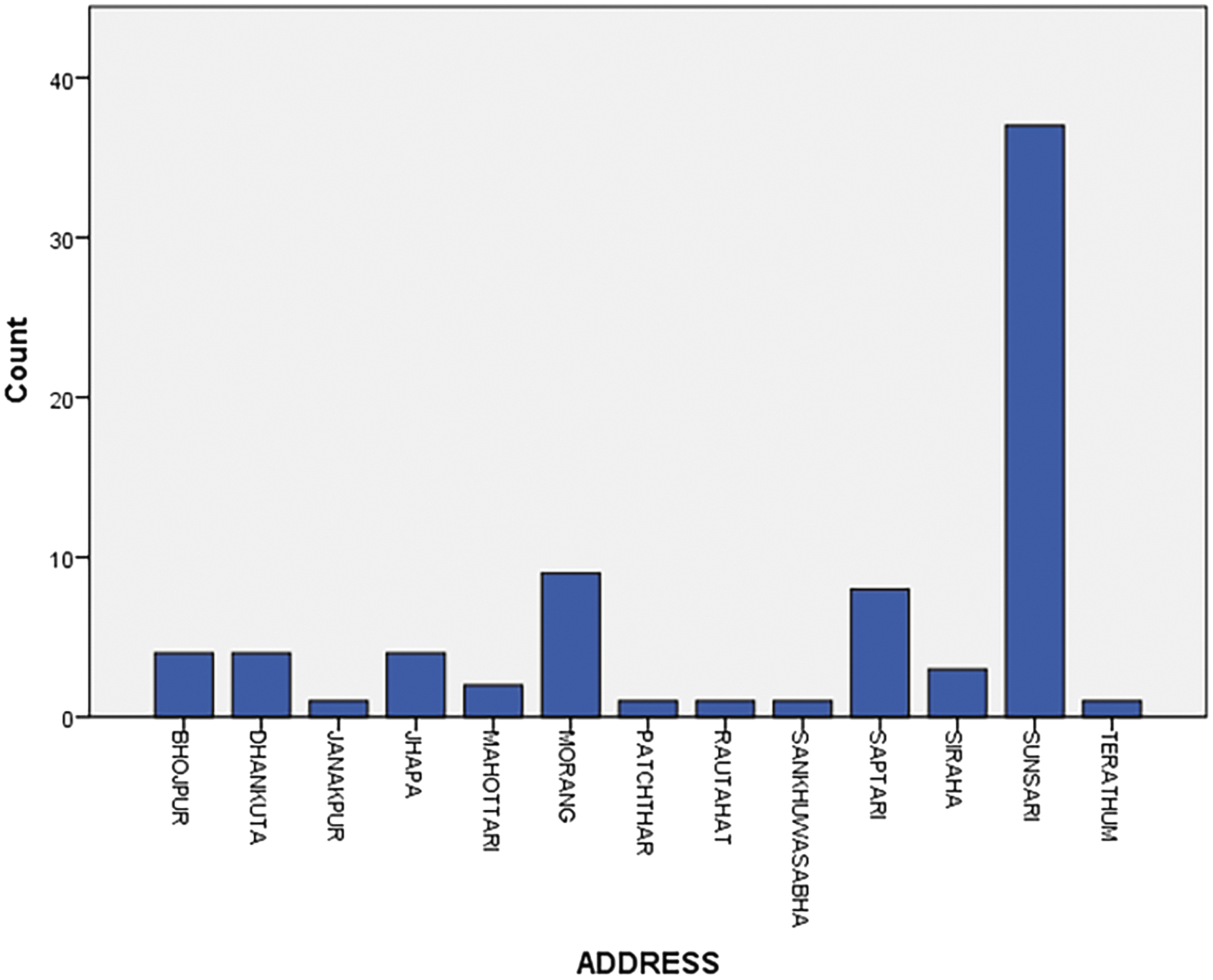
Distribution of patients based on districts.
Diagnosis
Of the total enrolled cases (n = 76), 71 (93.4%) were diagnosed with symptomatic gallstone disease, 3 (3.9%) were diagnosed with gall bladder polyp, and 1 (1.3%) was diagnosed with chronic calculus cholecystitis and empyema gall bladder (Fig. 4).
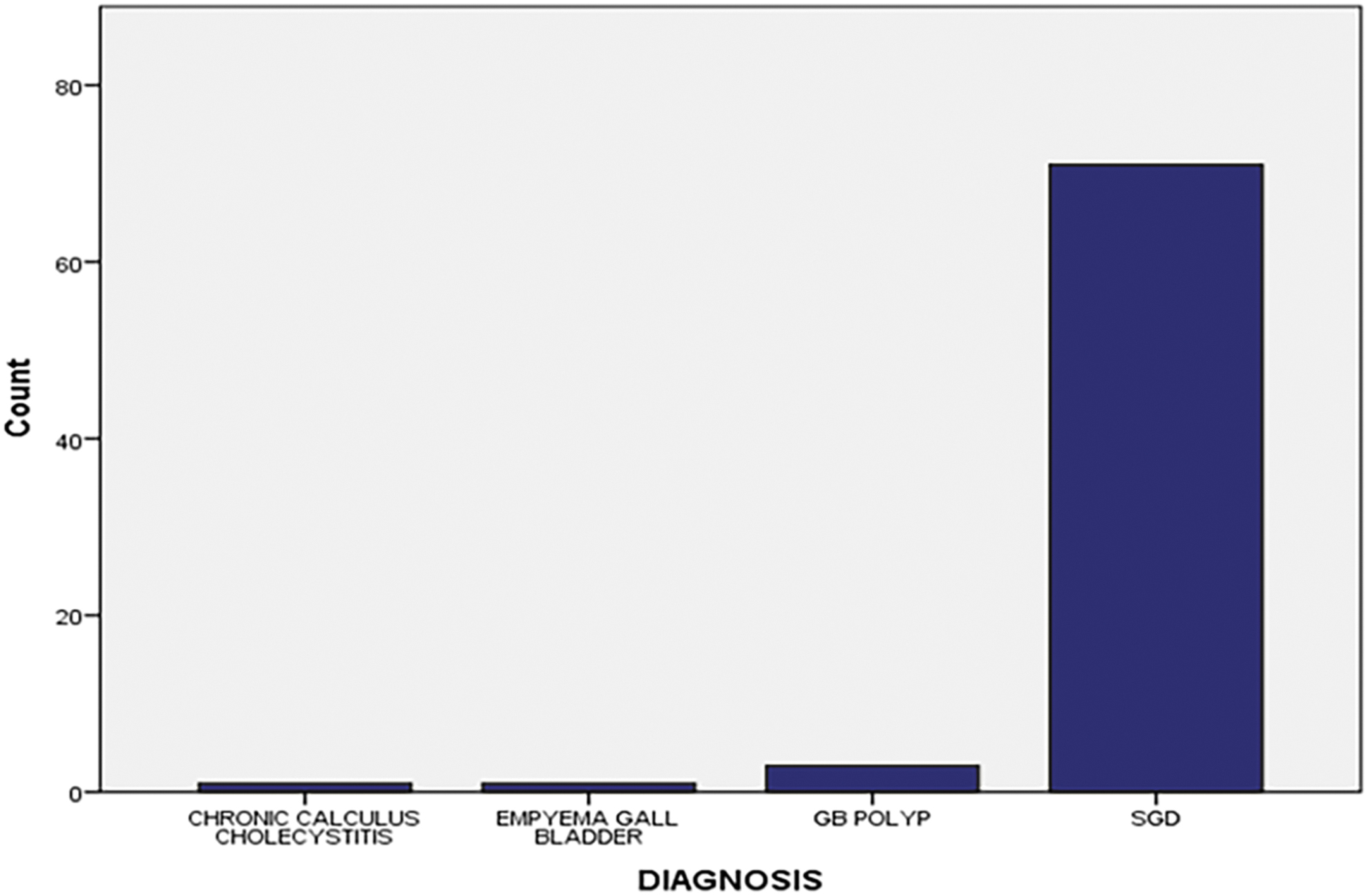
Diagnosis of patients.
The CVS achievement
During the dissection, a CVS was achieved in 75 (98.7%) of the cases, whereas in 1 case, CVS could not be achieved (Fig. 5).
Achievement of critical view of safety.
Visibility of RS after correct port placement, positioning, and traction of the gallbladder
After proper port installation, positioning, and traction of the gallbladder, RS was initially visible to the operating surgeons in 56 (73.7%) instances, whereas it was not visible in 20 (26.3%) cases (Fig. 6).

Visibility of Rouviere's sulcus after port placement, positioning, and proper traction of gallbladder.
Types of RS
RS was present in 56 (73.7%) cases, of which open sulcus type, closed sulcus type, slit type, and scar type RS were identified in 31 (40.8%), 7 (9.2%), 6 (7.9%), and 12 (15.8%) cases, respectively (Fig. 7).

Type of Rouviere's sulcus.
Intraoperative findings
Intraoperatively, 38 (50%) patients were found to have multiple calculi, 32 (42.2%) were found to have single calculus, and 3 (3.9%) of each gall bladder were found to have multiple and single polyps (Fig. 8).
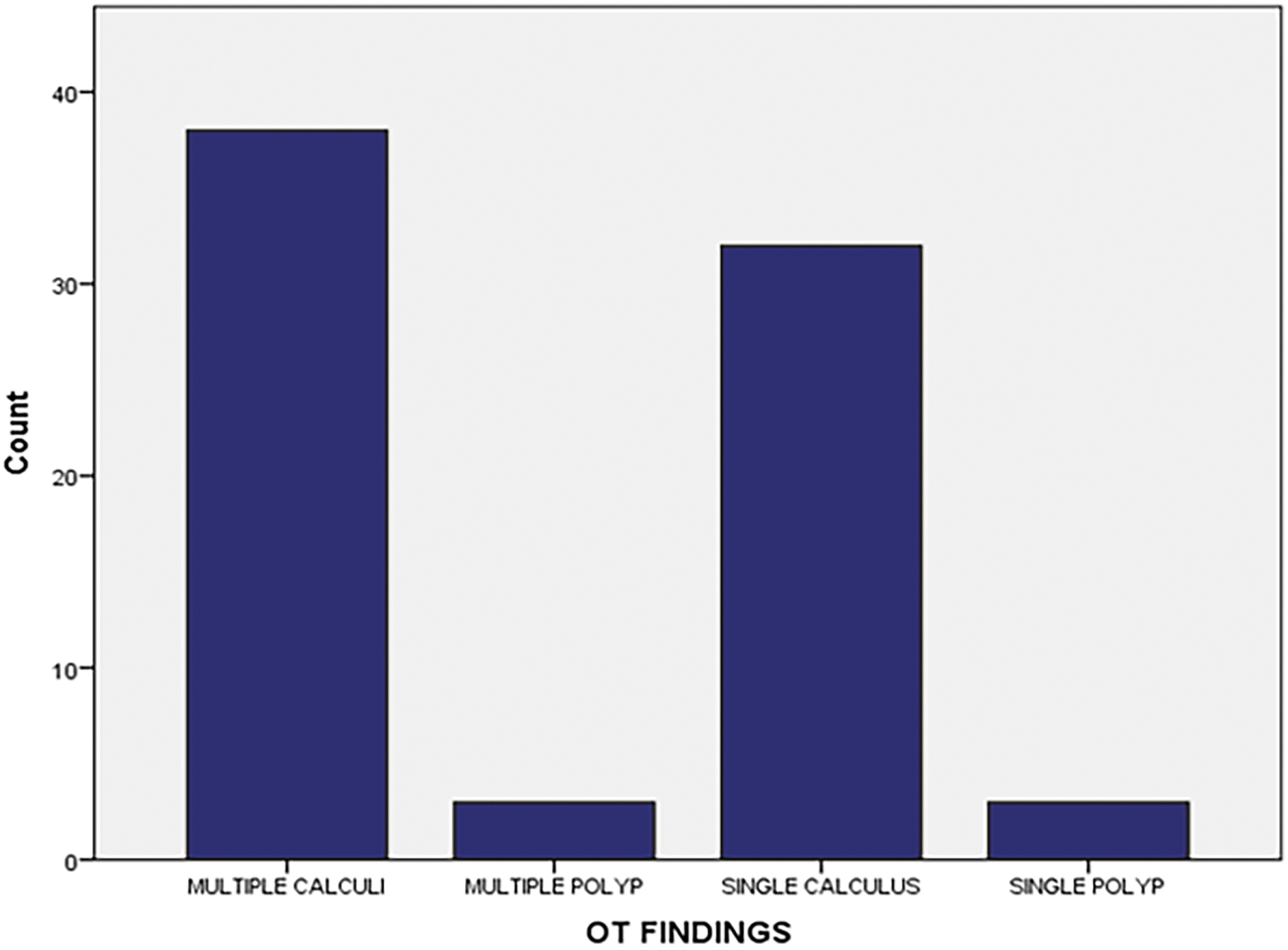
Intraoperative findings.
Biliary duct injury
No patient was found to have intraoperative or postoperative BDI.
Conversion to OC
Among 76 patients enrolled in our study, 75 patients underwent routine LC, whereas 1 patient underwent OC due to difficulty during the laparoscopic procedure.
The CVS versus conversion to OC
Of the total patients operated on, in only 1 patient CVS was not achieved and in the same patient routine LC was converted into OC owing to the difficult laparoscopic procedure (Table 1).
Critical View of Safety Versus Conversion to Open Cholecystectomy
RS versus conversion to OC
Of the total patients operated on, in 20 patients RS was absent and in 1 among the same group of patients, routine LC was converted into OC (Table 2).
Rouviere's Sulcus Versus Conversion to Open Cholecystectomy
Discussion
CVS is one the most accepted technique owing to its protective value during safe dissection in Calot's triangle. CVS clarifies the relations of the anatomic structures that should be divided, and, therefore, it should be ideally and routinely applied in all LCs because of its highly protective role against BDIs. CVS is a method of target identification, the targets being the CD and the cystic artery. 27
Owing to the pressure of carbon dioxide insufflation opening up the sulcus broadly, as well as the improved lighting and picture clarity of the laparoscopic camera, RS is visible quite clearly during LC.
When identification of Calot's triangle becomes difficult during the course of operation, RS can be used as a landmark of great significance as cystic artery and duct lie anterosuperior to this sulcus. Hence, it should be used as a reference point to begin dissection to avoid BDIs. 29
Age distribution
The average age of the patients in our research was 45.87 ± 15.33 years, indicating that simple gallstones are more common in people in their middle years. According to the study of Sachdeva et al., where the mean age was 41.5 ± 15.4 years. 30
The majority in our study were in the range of 26–35 years of age. This suggests a shift in the trend of gall stone disease from middle to young age, and this is in accordance with the study by Gupta et al. 31
Gender distribution
In our study, we found that the female-to-male ratio was 3:1, with females having a little larger prevalence of gallstones. According to a research by Sachdeva et al., the ratio of ladies to men with gallstones was 1.56:1. 30
Females are thought to be more at risk because of sex hormones. Estrogen causes bile to become oversaturated by increasing biliary cholesterol production.
Critical view of safety
CVS was achieved in 98.7% of patients in our study. A study performed by Avgerinos et al. achieved CVS visualization in 95.4% of 1046 LC. 14 Similarly, Nijssen et al. mentioned it to have been achieved in 80% of cases. 32 Similarly, Sanford and Strasberg achieved visualization of CVS in 78% of cases. 33
Pucher et al. provided an extensive literature review of 151 studies accounting for a total of 505,292 patients undergoing LC, and pooled data analyses (based on 70% of the included studies corresponding to 60% of patients) showed an overall BDI rate ranging from 0.32% to 0.52%. 34 Tornqvist et al. analyzed 51,041 cholecystectomies and reported an overall BDI rate of 1.5%. 35 In line with the very low incidence of BDI, our study further consolidated the fact without even a single BDI.
RS characteristics
Approximately 73.7% of the patients had RS, with the open sulcus type being the most prevalent. Other types of RS included scar, closed sulcus, and slit. Dahmane et al. reported that RS was present in 82% of normal livers, and open RS was the commonest. 36 Hugh et al. and Singh et al. noted RS in 78% and 84.5% of livers, respectively.37,38
Conversion of laparoscopic to OC
One patient with nonvisualization of CVS and Operational Theater finding of dense adhesion in gall bladder with frozen Calot's triangle was converted to OC as a bail-out procedure. In a study by Nassar et al., 0.49% of patients underwent conversion to OC with the most common causes of conversions being dense adhesions (32%) and impacted bile duct stones (25%). 39 Our study and study of Nassar et al. 39 further underlined the fact that despite the low incidence of conversion with recent technological advancement, chances of conversion with OT finding of dense adhesion and impacted bile duct stones are still relatively high.
Conclusion
Furthering the introduction of the technique is crucial, especially for training reasons, since the findings of CVS in the literature and this study indicate that the method will become the gold standard for the dissection of gall bladder components in the future. If the hepatocystic angle is impacted by advanced inflammation or developing fibrosis as a result of prior episodes of inflammation, CVS may not always be an option.
The open sulcus variety of RS is the most prevalent, and it affects the majority of people in our region of the world. Major difficulties can be avoided by identifying RS before cutting the cystic artery or duct during LC.
Limitation
Owing to the low predicted rate of events, multicenter studies are needed to analyze the result of the “BDI rate” with the power of our study insufficient.
Small sample size, limited research time, observational bias, and being a single-center-based study were some of the study's limitations.
Footnotes
Authors' Contributions
S.S.S., D.N., and N.L. contributed to conception, design of the study, and acquisition of data. S.S.S. was involved in analysis and interpretation of data. N.L. drafted the article. D.N. revised the article. All authors contributed to the final approval of the version to be submitted.
Data Availability Statement
Data used to support the findings of this study are included within the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.