
Abstract
Background:
Several methods to repair pediatric inguinal hernias utilizing a minimally invasive technique have been developed over the decades. These methods often involve passage of suture through the peritoneum at the level of the inguinal ring. We previously described the Godoy Burnia, a laparoscopic, sutureless, cautery-only inguinal hernia repair (IHR), and this follow-up study provides longer term data for this emerging surgical technique.
Methods:
After institutional review board approval, a single-centered retrospective review was performed of female pediatric patients with Godoy Burnia repair from 2014 to 2021. Demographics, operative details, and outcomes were reviewed.
Technique:
Through a single umbilical incision, a 3 mm port and camera and 3 mm Maryland dissector are placed into the abdomen. The Maryland dissector grasps the hernia sac, everts it, and brings it into the abdomen. Electrocautery is applied to allow scarring and closure of the inguinal ring.
Results:
Sixty-nine hernia repairs were performed on 44 patients with ages 5 days to 16 years (average 3.9 years) and weighing 2–70 kg (average 16 kg). Average follow-up was 52.8 months, and average operative times were 14/16 minutes for unilateral/bilateral repair, respectively. Twenty-two percent of hernias were found at time of another surgery and repaired. One recurrence (1.45%) in a 16-year-old patient, and 2 patients with other short-term complications.
Conclusions:
Godoy Burnia, a single-incision, sutureless, laparoscopic IHR in girls, is an acceptable alternative surgical technique with a low complication and recurrence rate. The longer follow-up in this study demonstrates the durability of the repair in most age groups, and decreased operative times suggest a favorable learning curve.
Introduction
The indirect inguinal hernia repair (IHR) is one of the most common operations performed by pediatric surgeons worldwide. This has historically been performed via an open surgery with high ligation of the hernia sac. However, increasing adoption of laparoscopy has led to the development of several novel techniques in the literature. The majority of these techniques describe suture ligation of the peritoneum at the internal inguinal ring in an attempt to shutter close the indirect defect.1–6 Over time, laparoscopic IHR has been shown to maintain similar recurrence rates, cost, and complications as open IHR. 7 However, critiques of laparoscopic suture ligation of the peritoneum include allowing the remnant herniated peritoneum to remain in situ within the inguinal canal, suture granuloma, and the usage of multiple laparoscopic ports with its associated pain, scarring, and hernia risk.
Minor peritoneal trauma at the internal inguinal ring induces scarring and more durable closure of an indirect defect than suture alone. 8 The Godoy Burnia technique was first published in 2017 by Novotny et al. 9 In this report, we previously described inversion and cauterization of the distal hernia sac as an effective, single-incision, sutureless IHR. Three subsequent publications have demonstrated functionality of the Godoy Burnia repair or variation but all with short-term follow-up of roughly 1.5–2.5 years.10–12
We hypothesize that the Godoy Burnia repair is a safe and durable repair. The aim of this study was to report our institutional outcomes paying close attention to longer follow-up, hernia recurrence, need for revision surgery, and operative time.
Methodology
This study was approved by the institutional review board (IRB) at Beaumont Hospital. Our studied patient population included females who were 18 years of age or younger and had unilateral or bilateral inguinal hernias. A female study population was specifically chosen so as to allow sufficient cautery without concern for thermal spread to the underlying vas deferens and gonadal vessels within the inguinal canal. The study was performed from 2014 to 2021, exclusively evaluating hernia repairs performed at Beaumont Hospital on the Royal Oak campus. The hernias repaired were either the primary operation or they were found incidentally during another case and repaired during the same operation. Our population was collected from hernia repairs performed by 1 pediatric surgeon at our institution during this time frame.
Patients were identified by a query of the electronic medical record evaluating the dates cross-referenced with the surgeon performing this procedure. Every patient listed in the study had a Godoy Burnia procedure completed for their herniorrhaphy. Once patients were identified by surgical intervention, data including patient age and weight at the time of surgery, unilateral or bilateral hernia repair, operative length, recurrence, and complications, among others were collected. Data collection was performed using a secured website collection sanctioned by the IRB. Data were compiled in a similar manner, de-identified, and then evaluated to determine the importance given our primary and secondary questions. Data were analyzed using GraphPad Prism 9.5.1 (www.graphpad.com). A simple linear regression was performed to establish a line of best fit when analyzing operative time through the years of the study.
Burnia technique
Our patient population had the Godoy Burnia technique performed for IHR (Fig. 1). The Godoy Burnia is a single-incision, sutureless, laparoscopic IHR typically performed via a single umbilical incision. As previously described, an incision is made in the umbilicus, a 3 mm port is inserted, the abdomen is insufflated, and a 3 mm laparoscope is inserted. Next, through the same skin incision, but via a separate small fascial defect, a 3 mm Maryland dissector is inserted into the abdomen (Fig. 2). After abdominal inspection and identification of either unilateral or bilateral inguinal hernias, the Maryland dissector is used to grasp the base of the hernia sac as distally as possible from within the internal inguinal ring (Fig. 3).

QR code, which links to Dr. Godoy's original YouTube video demonstrating his surgical technique.
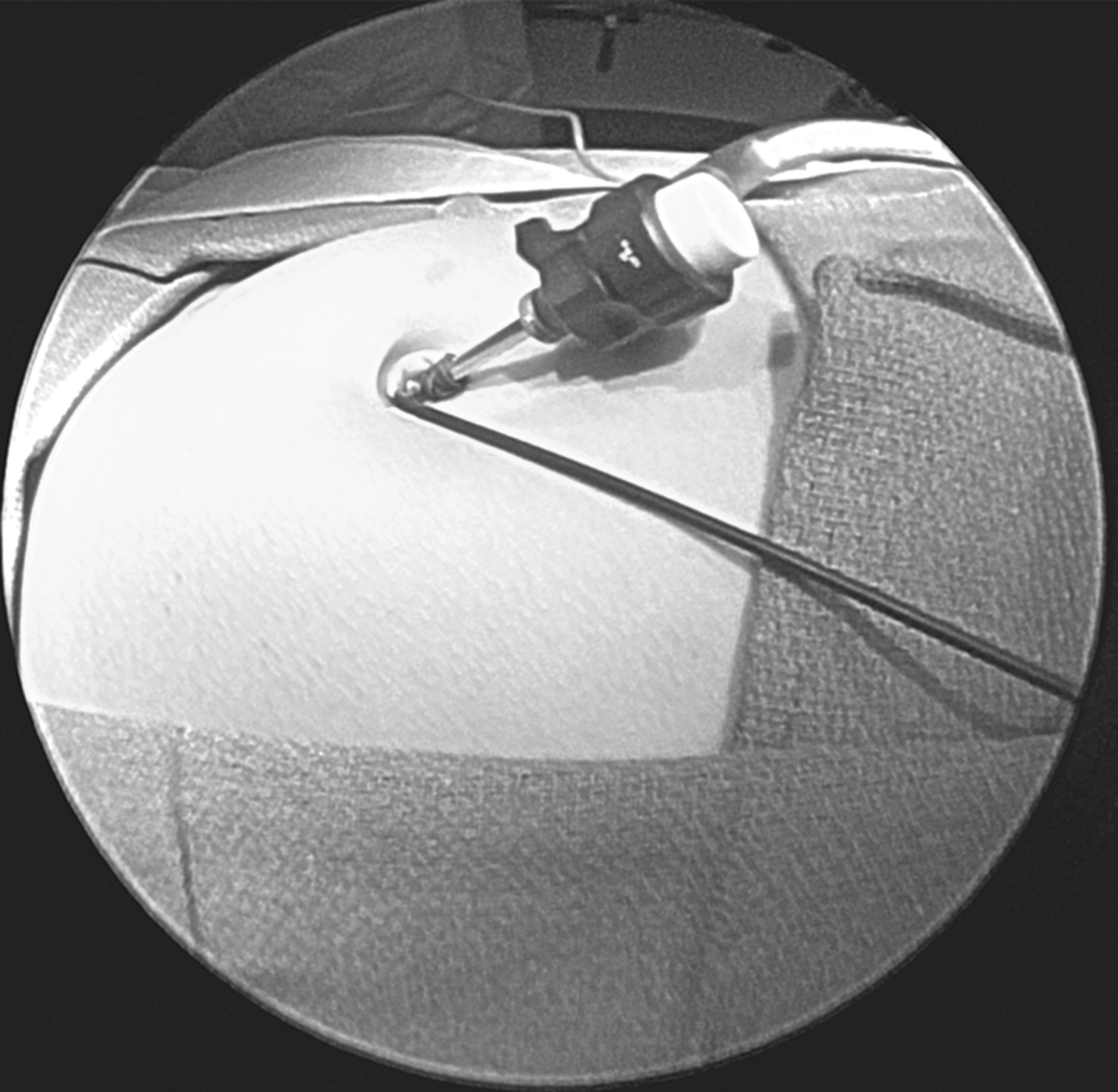
Umbilical incision with 3 mm port; Maryland dissector adjacent.
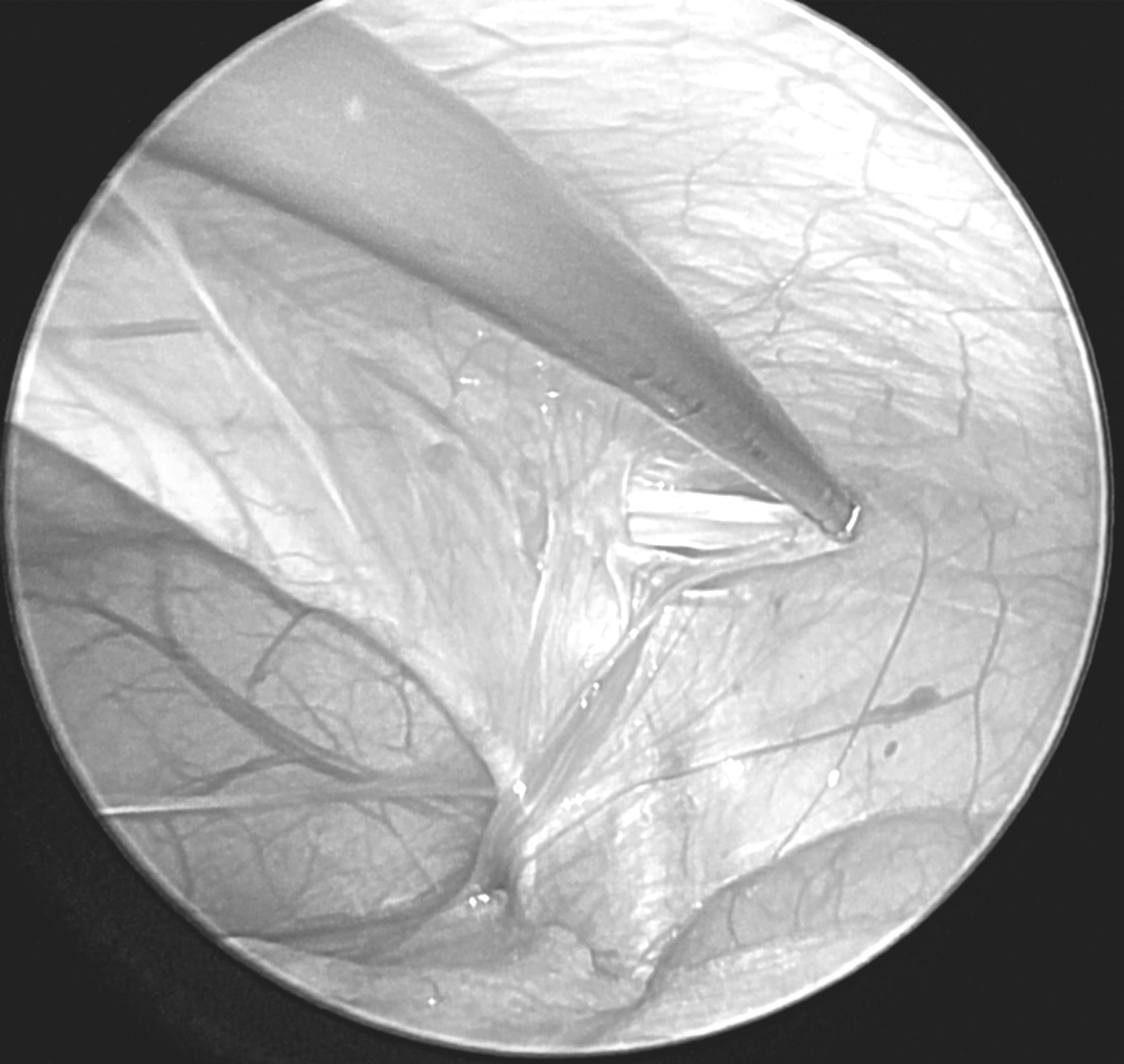
Indirect inguinal hernia.
The sac is then everted by pulling it back into the abdomen, while taking care to avoid the adjacent ovary or fallopian tube. Electrocautery is then applied through the Maryland dissector to the hernia sac to allow sufficient scarring and closure of the inguinal ring (Fig. 4). Specifically, the cauterized sac/patent processus vaginalis is no longer able to stent open the inguinal canal. The remaining fulgurated tissue closes the prior aperture in the abdominal wall and allows for additional scarring of the prior hernia site.
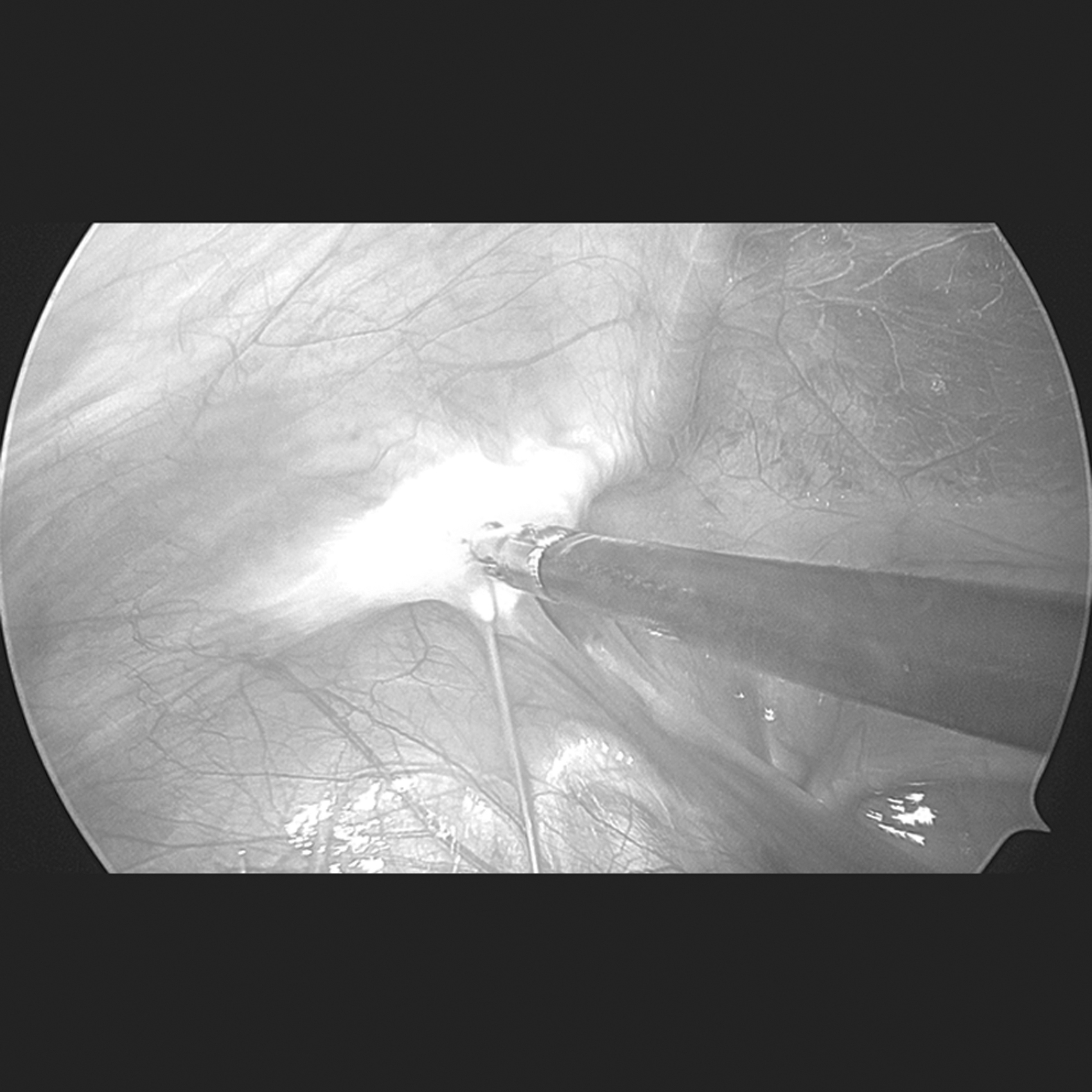
Inverted hernia sac fulgurated.
Results
There were 69 Godoy Burnia repairs performed on 44 patients between 2014 and 2021 at our institution. All repairs were completed laparoscopically without need to convert to an open surgery. Every surgery completed after February 2015 was completed via a single-incision technique. Every patient who underwent an elective Godoy Burnia repair was discharged the same day upon recovery in the post-anesthesia care unit. The average follow-up time was 52.8 months, with a range of 7.2–102 months.
The patient population had relatively few comorbidities with prematurity the most common (8/44, 18%). The average age of the study population was 3.9 years, with the youngest a premature 5-day-old infant and the oldest a 16-year-old (Fig. 5A). The majority of patients were infants and toddlers with 65.9% (29/44) aged 3 years and younger. Only 9.1% (4/44) of patients were teenagers. The average weight of our patients was 16 kg, with a range of 2–70 kg (Fig. 5B).
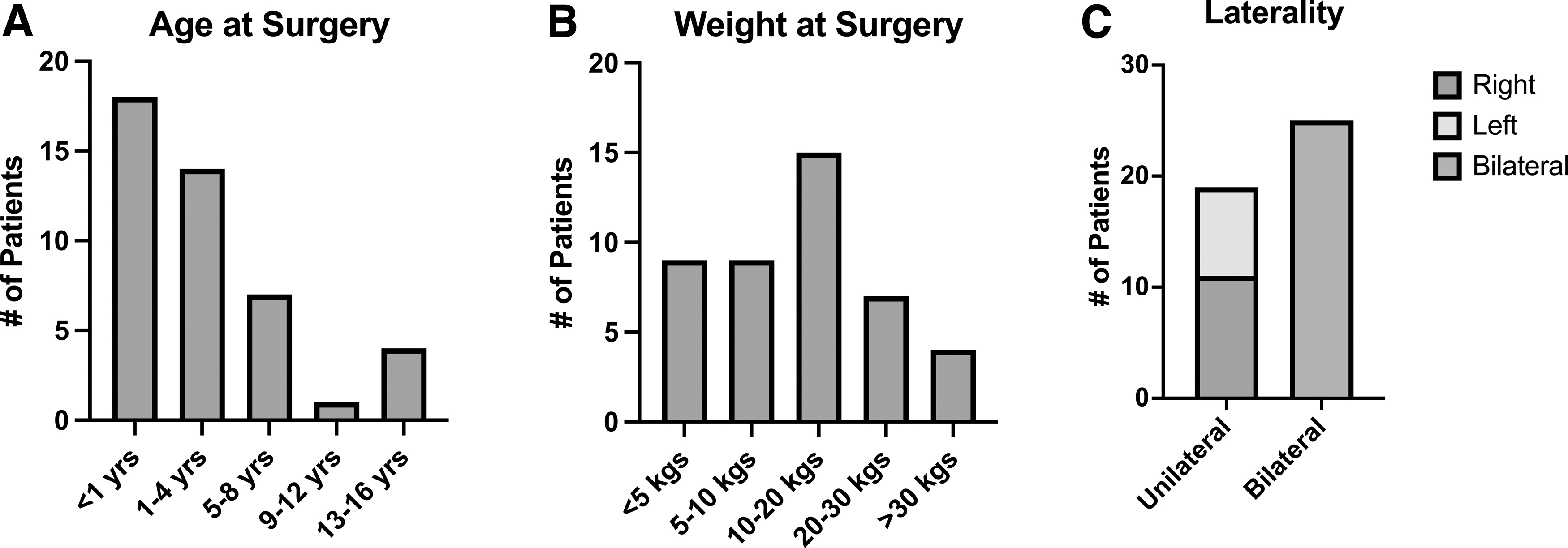
Overall, 15 of 69 hernias (22%) were found incidentally and performed at the time of another surgery. Nineteen patients underwent a unilateral Burnia repair (11 right, 8 left), and 25 patients had a bilateral hernia repair performed (Fig. 5C). Average operative times for unilateral and bilateral hernia repairs were 14 minutes (8–22 minutes) and 19 minutes (8–43 minutes), respectively. Of note, the three longest bilateral repair times were performed in 2014 and did not utilize a single-incision technique. The average operative time for a single-incision bilateral hernia repair was 14 minutes (8–25 minutes) (Fig. 6). In addition, in 2014, the first year of the study, the average repair took 24 minutes from start to finish, and in 2021, the final year of the study, the average repair lasted 12 minutes (Fig. 7). A simple linear regression found a slope of −1.366 minutes per year, indicating progressively shorter operations over time with an r2 value of 0.5877.

Operative time of elective Burnia repairs.
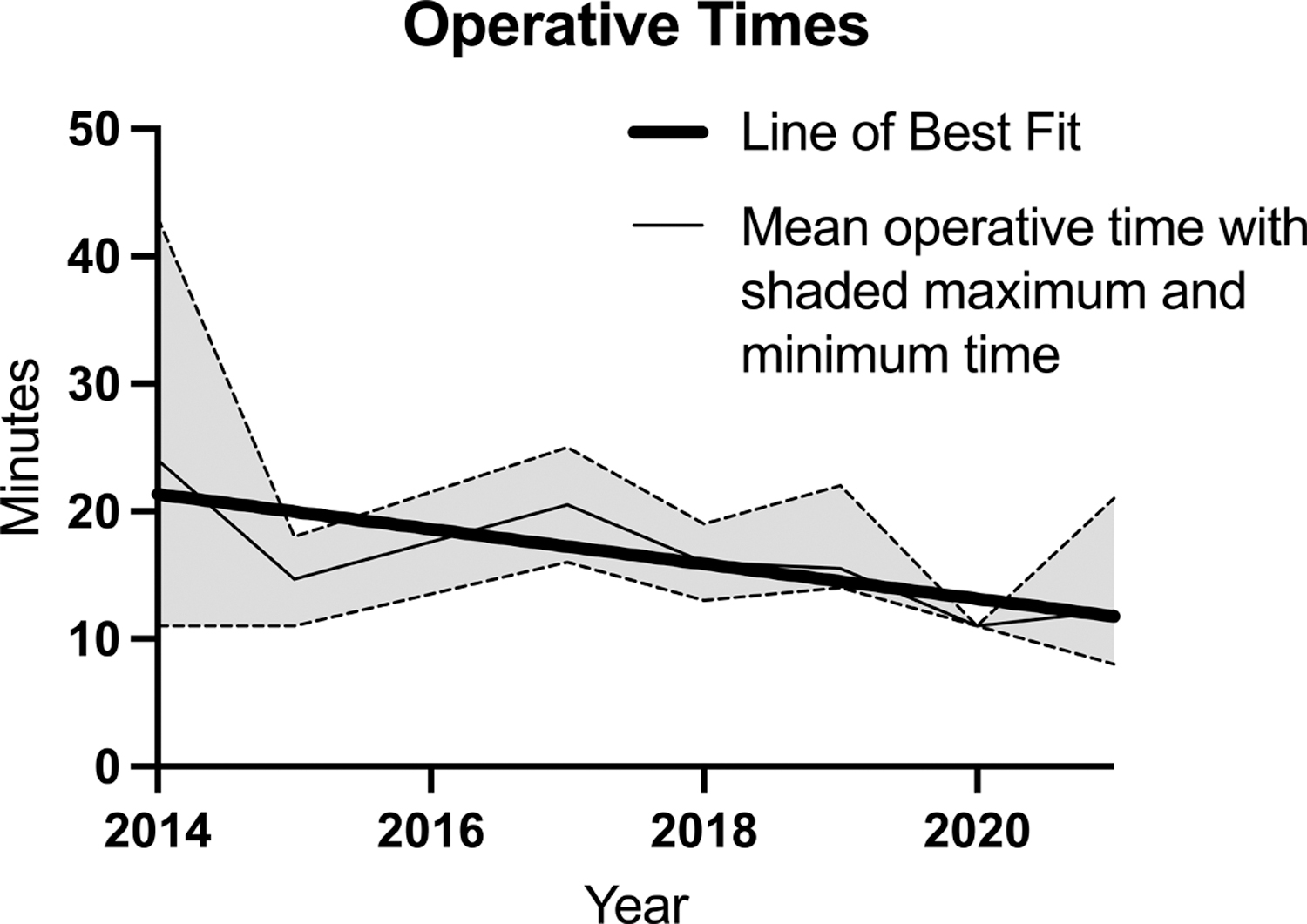
Operative time of elective Burnia repairs during the study period.
There were three complications (4.3%). A single recurrence (1.45%) in a 16-year-old patient was found 28 months following repair and underwent an open operation and is doing well in follow-up. The second complication was an incisional hernia from a secondary port site (repaired 1 month after the index surgery) on a 2 kg, 2-month-old, former 24-week postmenstrual age patient. The third complication was in a 3-year-old patient who developed an umbilical surgical site infection, requiring a short course of antibiotics.
Discussion
Historically, the Marcy repair, an open surgical procedure with an incision over the inguinal canal and suture ligation of the hernia sac, has been the predominant pediatric IHR. 7 With the increasing use of laparoscopy in the 21st century, there has been a rise in the number of pediatric patients who have undergone laparoscopic IHR, particularly within tertiary centers.7,13 There are a large number of operative techniques developed for laparoscopic herniorrhaphy, and the current literature demonstrates recurrence rates similar to traditional open repairs, with the added benefit of bilateral groin evaluation and less incisional morbidity. 14 The Godoy Burnia, a single-incision, sutureless, laparoscopic IHR in girls, has already been shown to be a viable option from our previous publication in 2017. 9 Other studies have evaluated the Godoy Burnia since Novotny et al., the most notable were two studies both published in 2019 and 2021.
In 2019, Marte et al. performed a prospective study describing their early implication of sutureless hernia repair. 11 There was no comparison group, and they did use preset inclusion criteria before obtaining consent from the patient's parents to perform herniorrhaphy. They had excellent results with both male and females, and latter of which they used the Godoy Burnia technique. In 2021, Duh et al. performed a double-armed study in which the Godoy Burnia procedure was compared with an open hernia repair. 10 There were ∼150 hernia repairs in each study arm. Their overall results showed no hernia recurrences for either repair at the time of follow-up.
We completed this retrospective follow-up study as a single-institution cohort study that has longer follow-up than our previous publication. Like our first publication, our results still demonstrate both low complication and hernia recurrence rates, in line with other methods of pediatric herniorrhaphy. We drew three main conclusions from our new set of collected data. First, compared with our initial results, the average operative time has decreased by nearly half in this study. Each year of the study, there has been a consistent decrease in the operative length of procedure (Fig. 7). This likely is a result of familiarity with the procedure from staff and resident education in this technique. This suggests that, while there is a learning curve, the repair can be performed very expeditiously. This may bear out to a future cost–benefit when compared with open repair.
Second, longer term follow-up in our patient population still shows low rates of reoccurrence, with <2% reoccurrence rates over an average of 52.8 months follow-up. Third, we recommend caution in adolescent or teenage children given our hernia recurrence that occurred 28 months following repair. We had only 4 adolescents in our study population, but this late recurrence raises the question of the durability of the repair technique in this age group. While our average follow-up for adolescents was 60.25 months, arguing that the other three repairs were successful and durable, we would caution use in older, larger children. We believe that the application of this technique in this age group should fall under the jurisdiction of an IRB-approved study.
While our study is an important follow-up to our original publication, there are several limitations to discuss. An obvious limitation is that our study is confined to a single institution and surgeon. Our surgeon has been performing the Godoy Burnia technique for 9 years and has become very proficient at both performing and teaching the technique, which is demonstrated in continually decreasing operative times. While the number of herniorrhaphies performed is relatively small (<100), there does seem to be a dramatic increase in proficiency with this technique as evidenced by the decrease in operative time. Next, this is a retrospective case series that is without comparison to the gold standard open approach.
We were hesitant to compare with open approaches during the same time period because the senior author did not perform any and the variation in operative time with other institutional surgeons would add a variable that would be difficult to account for. There were no set guidelines on which patient is well fitted for a Godoy Burnia repair aside from the patient being female and pediatric with an inguinal hernia. The size of the hernia, laterality, or how the hernia was identified was not part of our methodology. Finally, our sample size is limited to fewer than 100 hernias repaired. This is, in part, due to the single surgeon, single-center report, but also the population is limited given the relative rarity of female inguinal hernias when compared with males.
To further prove the Godoy Burnia as a reproducible reliable technique in female pediatric patients with inguinal hernia, these limitations must be addressed. Multicenter prospective studies with larger patient numbers must be performed to match existing hernia research and data in pediatric herniorrhaphy. Factors to be considered are cosmesis, operative time which ultimately translates to overall cost, and postoperative pain. The reproducibility shown by our study and the other current authors demonstrating Godoy Burnia as a valid technique is encouraging.9–11 We believe that this repair is an excellent option for indirect inguinal hernia in females and should be able to be performed by most pediatric surgeons, using these articles and Dr. Godoy's YouTube video as a guide. With increased use and a larger population, we will discover the ideal population in which to use the repair and recognize the best indication and shortcomings.
Conclusions
The Godoy Burnia, a single-incision, sutureless, laparoscopic IHR in girls, is an acceptable alternative surgical technique with a low complication and recurrence rate. The longer follow-up in this study demonstrates the durability of the repair in the majority of age groups, and decreased operative times suggest a favorable learning curve. Further adoption and study of this novel technique will better identify which populations are best served by this approach.
Footnotes
Authors' Contributions
D.F.: Data curation (equal), formal analysis (equal), investigation (lead), project administration (lead), resources (equal), validation (equal), visualization (supporting), writing—original draft (equal), writing—review and editing (lead). S.W.: Data curation (equal), formal analysis (equal), investigation (supporting), project administration (supporting), resources (equal), validation (equal), visualization (lead), writing—original draft (equal), writing—review and editing (supporting). J.G.L.: Data curation (supporting), formal analysis (supporting), investigation (supporting), project administration (supporting), resources (supporting), validation (supporting), visualization (supporting), writing—original draft (supporting), writing—review and editing (supporting), supervision (supporting). N.N.: Data curation (supporting), formal analysis (supporting), investigation (supporting), project administration (supporting), resources (equal), validation (equal), visualization (supporting), writing—original draft (supporting), writing—review and editing (supporting), supervision (lead).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.