
Abstract
Background:
Transumbilical laparoscopy-assisted appendectomy (TULAA) is the technique of choice for all types of appendicitis. However, the technique is challenging for trainees to learn in comparison with performing conventional three-port laparoscopic appendectomy (CTPLA) in children. We aimed to compare the surgical outcomes of children with appendicitis treated by TULAA versus CTPLA performed by pediatric surgeons in training (PSITs).
Materials and Methods:
This retrospective study analyzed pediatric patients with acute appendicitis treated with CTPLA or TULAA between April 2016 and December 2022. Operative time (OT: minutes), pneumoperitoneum time (PT: minutes), blood loss (milliliter), length of hospital stay (days), and surgical site infection rate were compared between the two groups. Operative outcomes were also analyzed according to type of appendicitis such as uncomplicated and complicated cases.
Results:
Two hundred twenty-five laparoscopic appendectomies were performed by CTPLA (n = 94) or TULAA (n = 131). All cases were performed by PSITs and there was no open conversion cases. TULAA had a shorter OT (67.0 ± 28.4 versus 78.3 ± 21.7; P < .01) and PT (26.1 ± 17.4 versus 52.5 ± 22.1 min; P < .01). The surgical site infection rate was slightly higher in the TULAA group, but the difference was not statistically significant. In uncomplicated appendicitis (n = 164), significant differences between the CTPLA and TULAA groups were observed in OT (CTPLA versus TULAA: 70.7 ± 14.9 versus 59.1 ± 21.6, P < .01) and PT (CTPLA versus TULAA: 43.6 ± 13.1 versus 20.4 ± 13.6, P < .01). With regard to postoperative complications, only surgical site infection was significantly different between the CTPLA and TULAA groups (CTPLA: 0.0% versus TULAA: 8.2%, P < .05). In complicated cases (n = 61), there were significant differences between the groups in PT (CTPLA versus TULAA: 73.4 ± 24.9 versus 42.3 ± 17.2, P < .01) and length of hospital stay (CTPLA versus TULAA: 7.0 ± 1.3 versus 8.9 ± 4.7, P < .05).
Conclusions:
TULAA had a shorter OT and PT than CTPLA. TULAA for PSITs shows similar safety and feasibility to CTPLA for not only uncomplicated cases but also complicated cases.
Introduction
In 1983
Although various techniques have been developed for the treatment of acute appendicitis, there are few reports on appropriate techniques that combine surgical training and minimally invasive techniques.
In this study, we compared surgical outcomes between pediatric patients who underwent TULAA or CTPLA for uncomplicated or complicated appendicitis. We also aimed to evaluate the feasibility of TULAA for complicated appendicitis when performed by pediatric surgeons in training (PSITs).
Materials and Methods
We conducted a retrospective study of laparoscopic appendectomies for pediatric acute appendicitis performed between April 2016 and December 2022. The patients underwent interval appendectomy, and those whose pathological findings included “catarrhalis” were excluded. All operations were performed by PSITs and the surgical technique was selected according to the preference of the supervising surgeon. CTPLA was performed between April 2016 and March 2019. TULAA was introduced on April 2019 and performed between April 2019 and December 2022
Surgical procedures
The CTPLA procedure
A 12-mm or 5-mm trocar is placed at the umbilicus using the open access procedure and the abdominal cavity is identified using a 5-mm 30° telescope. The abdomen is insufflated to 8 mmHg with carbon dioxide. A 5-mm trocar is placed at the left lower abdominal quadrant, and another 5-mm port is placed at the suprapubic region as working ports (Fig. 1a). The appendix is identified and then grasped by a laparoscopic grasper. The mesoappendix is dissected using an ultrasonically activated device (Harmonic ACE plus®; Ethicon Endo-Surgery, Cincinnati, OH, USA). Ligation is performed at the base of the appendix with an ENDOLOOP® (Ethicon Endo-Surgery) and another ligation is performed 1 cm distal from the previous ligation and the appendix is dissected using the ultrasonically activated device.
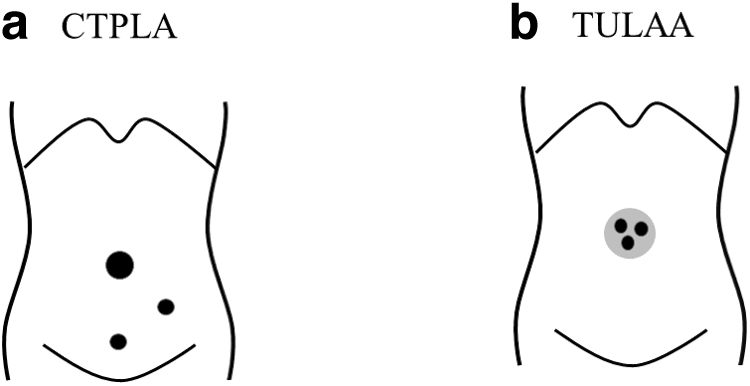
Port layout for CPTLA and TULAA. CTPLA, conventional three-port laparoscopic appendectomy; TULAA, transumbilical laparoscopically assisted appendectomy.
The TULAA procedure
A 15-mm skin incision is made at the umbilicus, so as not to exceed the umbilical ring, and laparotomy is performed. A single-port device composed of a wound protector and a cap with trocars (Arunote Lap Single®) is applied to the incision site. The abdominal cavity is identified using a 5-mm 30° telescope (Fig. 1b). The abdomen is insufflated to 8 mmHg with an ultrasonically activated device (Harmonic ACE plus; Ethicon Endo-Surgery) for dissection. After exploration of the peritoneal cavity, the peritoneal attachments to the appendix and cecum are dissected to allow the appendix to reach the umbilicus (Fig. 1b).
The cap of the single port device is opened, and the wound protector in the single-port device is left at the transumbilical incision site. The appendix is extracted through the transumbilical incision by pulling out the grasper holding the appendix. The appendix is then resected outside the abdominal cavity.
Statistical analyses
Statistical analyses for nominal variable were performed using the chi-squared test for parametric data and Fisher's exact test for nonparametric data. Statistical analyses for continuous variables were performed using the t-test for parametric data and Mann–Whitney U test for nonparametric data. P < .05 were considered to indicate statistical significance. Data are expressed as the mean ± standard deviation. All statistical analyses were performed with the EZR software program (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add the statistical functions frequently used in biostatistics.
Ethical concerns
This study was performed in accordance with the ethical guidelines for medical and health research involving human subjects by the Ministry of Health, Labor, and Welfare of Japan in 2014. The study complied with the 1964 Declaration of Helsinki (revised in 2013) and was approved by the local ethics committee of Kagoshima University Hospital (Registration No.: 27–119). All of the participants or their parents provided their informed consent for inclusion in this study.
Results
During the study period, 8 PSITs were responsible for the surgery.
Patient background characteristics
Two hundred twenty-five pediatric laparoscopic appendectomies were performed in this study (CTPLA, n = 94; TULAA, n = 131). Table 1 gives the background characteristics of the patients in the CTPLA and TULAA groups. The background characteristics of the two groups did not differ to a statistically significant extent.
Patient Background and Characteristics in the Overall Population
CTPLA, conventional three-port laparoscopic appendectomy; n.s., no significant; TULAA, transumbilical laparoscopically assisted appendectomy.
The operative results and clinical outcomes in all patients
The operative results and clinical outcomes are given in Table 2. The operative time (OT) and pneumoperitoneum time (PT) in the TULAA group were both shorter than those of in the CTPLA group (OT, TULAA versus CTPLA: 67.0 ± 28.4 versus 78.3 ± 21.7, P < .01; PT, TULAA versus CTPLA: 26.1 ± 17.4 versus 52.5 ± 22.1, P < .01). There were no significant differences in the other results (Table 2). In the TULAA group, intraperitoneal resection was performed in 5 cases (3.5%) because it could not be pulled out of the umbilicus.
Operative Results and Outcomes in the Overall Population
CTPLA, conventional three-port laparoscopic appendectomy; n.s., no significant; TULAA: transumbilical laparoscopically assisted appendectomy.
Patient background characteristics according to the type of appendicitis
We defined the type of appendicitis based on the intraoperative findings. Cases without intraoperative findings of obvious perforation were defined as uncomplicated (n = 164). Cases with obvious perforation were defined as complicated (n = 61). Patient background characteristics according to the type of appendicitis were shown in Table 3. With the exception of sex and WBC count, There were significant differences (P ≤ .01) in the patient characteristics of the two groups (uncomplicated versus complicated: age [years old]; 10.4 ± 2.4 versus 9.2 ± 3.1, body weight [kg]; 36.3 ± 12.9 versus 30.2 ± 11.9, body temperature [°C]; 37.3 ± 0.7 versus 38.1 ± 0.8, illness period [days]; 1.3 ± .1.1 versus 2.1 ± 1.5, WBC [/μL]; 13,637 ± 3984 versus 15,694 ± 4957, CRP [mg/dL]; 3.1 ± 4.3 versus 10.2 ± 7.4, size of appendix [mm)] 9.5 ± 3.0 versus 10.4 ± 3.0).
Preoperative Data and Outcomes in Patients with Uncomplicated Appendicitis
CTPLA, conventional three-port laparoscopic appendectomy; n.s.: not significant; TULAA, transumbilical laparoscopically assisted appendectomy.
CTPLA versus TULAA in uncomplicated appendicitis
The preoperative data and outcomes of CTPLA and TULAA in patients with uncomplicated appendicitis are given in Table 3. Among patients with uncomplicated appendicitis, CTPLA and TULAA were performed for 66 and 98 patients, respectively. Regarding the preoperative data, significant differences between the CTPLA and TULAA groups were observed in body temperature alone. Regarding the operative data, significant differences between the CTPLA and TULAA groups were observed in OT (CTPLA versus TULAA: 70.7 ± 14.9 versus 59.1 ± 21.6, P < .01) and PT (CTPLA versus TULAA: 43.6 ± 13.1 versus 20.4 ± 13.6, P < .01).
Length of hospital stay was not significantly different (CTPLA: 4.1 ± 0.4 versus TULAA: 4.0 ± 0.5, P > .05). No patients underwent appendectomy internally in the TULAA group. With regard to postoperative complications, only surgical site infection was significantly different between the CTPLA and the TULAA groups (CTPLA: 0.0% versus TULAA: 8.2%, P < .05). However, all of the surgical site infection (SSI) were mild infections that improved with only wound washing at home.
CTPLA versus TULAA in complicated appendicitis
The preoperative data and outcomes of CTPLA and TULAA in patients with complicated appendicitis are given in Table 4. Among patients with complicated appendicitis, CTPLA and TULAA were performed for 28 and 33 patients, respectively. There were no significant differences in patient background characteristics or preoperative data between the CTPLA and TULAA groups. There were significant differences between the groups in PT (CTPLA versus TULAA: 73.4 ± 24.9 versus 42.3 ± 17.2, P < .01) and length of hospital stay (CTPLA versus TULAA: 7.0 ± 1.3 versus 8.9 ± 4.7, P < .05); however, the OT of the two groups did not differ to a statistically significant extent (CTPLA versus TULAA: 96.3 ± 24.9 versus 90.2 ± 33.6, P > .05).
Preoperative Data and Outcomes in Patients with Complicated Appendicitis
CTPLA, conventional three-port laparoscopic appendectomy; n.s.: not significant; TULAA, transumbilical laparoscopically assisted appendectomy.
There was no significant differences between the two groups in postoperative complications including surgical site infection. In the TULAA group, intraperitoneal resection was performed in 5 cases (15.1%) because it could not be pulled out of the umbilicus.
Discussion
This study focused on the outcomes and retrospectively reviewed the treatment of pediatric appendicitis patients who were treated at our institution. The major findings of this study were as follows. (1) In all patients, TULAA had a shorter OT, and PT. Blood loss and length of hospital stay of the 2 groups were not significantly different. (2) The surgical site infection rate was slightly higher in the TULAA group. (3) In uncomplicated appendicitis, OT and PT in the TULAA groups were significant shorter than those in the CTPLA group. Surgical site infection in the TULAA group was significantly higher than that in the CTPLA group. (4) In complicated cases, PT in the TULAA group was significantly shorter than that in the CTPLA group. Length of hospital stay in the CTPLA group was significantly shorter than that in the TULAA group.
Single-site (incision) laparoscopic appendectomy (SLA) is an effective alternative to conventional three-port laparoscopic appendectomy (CTPLA) and is one of the techniques that is spreading to various centers because it requires only a small incision within the umbilical ring, which is barely noticeable after surgery. However, previous studies comparing SLA and CTPLA in adults have shown that SLA is associated with significantly longer operative times, and technical difficulties may be the reason for the longer operative time during internal resection of the appendix in SLA. 3
Especially in pediatric surgery, though the number is still not large, an increasing number of studies are being conducted on the removal of the appendix through a single umbilical incision and extracorporeal excision. 4 In contrast, TULAA combines the advantages of good intra-abdominal visibility of laparoscopy with the safety and rapidity of conventional external open appendectomy. Several recent reports using TULAA in children have shown significantly shorter operative times than CTPLA. 5 However, in general, there is concern that single-site (incision) surgery is more technically challenging than CTPLA, especially for surgeons in training, due to the limitations of intraperitoneal forceps manipulation and forceps–endoscope interference outside the body.
In the case of TULAA, many studies have reported a completion rate of ∼80% in adults and children without conversion to laparotomy or additional port. 6 In our cases, the percentage of cases in whom the appendix was resected internally because it could not be pulled out of the umbilicus was only 4.6%. No cases were treated with an additional port and no cases were converted to laparotomy. The OT for these patients was 67.0 ± 28.4 minutes for TULAA and 78.3 ± 21.7 minutes for CTPLA. This difference was statistically significant, which suggests that TULAA is a shorter and better tolerated technique.
This may be because the distance between the umbilicus and the ileocecal area is shorter, especially in children, and the ileocecal area is loosely fixed, facilitating withdrawal to the umbilicus. As for wound infections, all did not require antibiotics and those improved with home cleaning alone. Although CTPLA and TULLA showed no difference in postoperative wound infection rates, the present results show that surgical time is comparable and PSIT is as acceptable for performing TULLA as it is for CTPLA
Especially in the cases of uncomplicated appendicitis, there were no significant differences in patient background, and the OT, PT, and the length of hospital stay in the TULAA group were significantly shorter than in the CTPLA group. The reason for the shorter OT in the TULAA group may be related to the fact that the resection of the appendix and the mesoappendix is easier than in CTPLA because appendectomy is performed by pulling the appendix out of the wound, and the PSITs are working with the supervising surgeon, making the procedure similar to open surgery. Unfortunately, wound infections were somewhat more common in uncomplicated appendicitis.
The fact that there was no overall difference and only minor infections suggests that measures such as additional intraoperative wound cleansing and covering should be considered. These results were in line with the relevant literature, and TULAA is considered feasible, especially for uncomplicated appendicitis.
In several studies of complicated appendicitis, SLA including TULAA was reported to be associated with a longer OT in comparison with CTPLA,4,7,8 and many other operative outcomes were reported to be comparable between the two groups. 9 However, the results of this study differed from some previous reports: the OT remained the same and there were no significant differences in surgical outcomes, such as the complication rate. This difference may be due to two factors: the surgeons who performed the surgeries were PSITs (either near to or after the end of their surgical training) and they may have been more familiar with laparoscopic appendectomy than expected. In fact, some of the trainees had never performed open appendectomy.
They performed laparoscopic dissection of adhesion and, in some cases, dissected the ileocecal site and pulled the appendix out of the wound, even in cases in whom the appendix could not be easily pulled out from the wound due to difficulty in detaching adhesions due to abscess formation, physiological adhesions, and other reasons. Although potentially more invasive, the technique of detaching adhesion from the retroperitoneum can be applied to other procedures, such as ileal resection, with no difference in blood loss or complications and would be a very good method for surgeons in their later training and for surgeons with a high degree of specialization. 10
Also, unlike in the past, the training environment for laparoscopic surgery has improved considerably, and one factor may be that trainees can use a dry box to familiarize themselves with the operation of equipment used in SLA and other procedures. In fact, TULAA was associated with a very high completion rate (96.5%), and the rate of achievement was higher than that described in the relevant literature.
Basically, the complications of TULAA are the same as those of CTPLA. However, studies have reported that TULAA is associated with a higher incidence of wound infection in comparison with conventional CTPLA. 6 This is presumably because the appendix is pulled directly into the wound, making it easier for the appendix to come into contact with the wound and cause infection. In our institution, the rate of surgical site infection was high in simple appendicitis. It is thought that devices such as the wrap protector used in our institution, which prevents contamination of the wound, can improve the incidence of wound infection. According to the results of this study for simple appendicitis, this issue should be further investigated with the accumulation of more cases in the future.
Many studies have reported that TULAA is superior to CTPLA from a cosmetic standpoint. Although objective evaluation is difficult, in many cases who were managed in our institution, the scars were not noticeable and the surgery was well received by the patients' families. In addition, similarly to other reports, TULAA was considered a useful technique from the medical economic viewpoint, as it reduced the number of supplies used in comparison with CTPLA.
Limitations
This study was associated with some limitations including the fact that it was conducted retrospectively, and that the study population was relatively small. In addition, there is no difference in surgical technique, instruments used, or antibiotics used, but the duration is somewhat longer than 7 years. We were not able to evaluate the PSITs with respect to their years of experience and their respective proficiency levels, and it is possible that the supervising physicians are judging the choice of surgical techniques based on the status of PSITs, which is also a limitation. Accordingly, a randomized control study should be conducted in the future.
Conclusion
We compared the TULAA and CTPLA techniques, which combine the advantages of SLA and open surgery, when performed by a pediatric surgeon in training. TULAA had a shorter OT and PT than CTPLA. TULAA for PSITs shows similar safety and feasibility to CTPLA. The results showed that TULAA was considered an acceptable technique even for complicated appendicitis, even performed by trainee surgeons. According to our results, TULAA can be performed for appendicitis with adhesions and abscesses and can be flexibly modified to a multi-port approach in difficult cases, while CPTLA can be performed for appendicitis with adhesions and abscesses. TULAA can be used for appendicitis and the results were comparable with the conventional principle. TULAA can also be cosmetically and economically superior to CPTLA. Further improvement of surgical techniques and instruments is needed to improve the infection rate in TULAA.
Footnotes
Acknowledgment
The authors thank Brian Quinn for his comments and help with the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.