
Abstract
Background:
Laparoscopic liver resection (LLR) has become a widely used standardized operation for patients with hepatocellular carcinoma (HCC) in the field of hepatic surgery. However, the risk factors and long-term implications associated with unplanned conversion to an open procedure during the LLR have not been adequately studied.
Methods:
The study incorporated 96 patients with HCC. Risk factors of conversion and their prognosis were analyzed by comparing patients who successfully underwent LLR with those who required unplanned conversion.
Results:
In this study, the unplanned conversion rate for laparoscopic hepatectomy was 42.7%. Patients who underwent conversion had longer length of stay (8 versus 7 days, P < .001), longer operation time (297.73 versus 194.03 minutes, P = .000), a higher transfusion rate (29.3% versus 5.5%, P < .001), and more postoperative complications compared with patients who successfully underwent LLR. The two surgical maneuvers did not show substantial disparities in terms of total survival and disease-free survival rates. Risk factors of unplanned conversion contained tumor location (odds ratio [OR], 3.129; 95% confidence interval [CI]: 1.214–8.066; P = 0.018) and tumor size (OR, 2.652; 95% CI: 1.039–6.767; P = 0.041).
Conclusions:
The unplanned conversion during LLR for HCC was linked to unfavorable short-term prognosis, yet it did not influence long-term oncologic outcomes. Moreover, preoperative evaluation of tumor size and location may effectively reduce the probability of unplanned conversion during LLR.
Introduction
Ever since the initial instance of laparoscopic liver resection (LLR) was reported in 1991, LLR has becoming the preferred maneuver for patients with hepatocellular carcinoma (HCC).1–4 In contrast to open liver resection (OLR), LLR has the advantages of less intraoperative blood loss, less postoperative pain, a shorter hospital stay, and a lower complication rate, as well as no significant difference in tumor R0 resection rate, operative mortality, and postoperative survival rate.2,4,5 In addition, because of the high difficulty and risk, the rich experience of operator is required to complete LLR. 6 However, unplanned conversion to OLR during LLR is unavoidable due to the difficulty to control bleeding or approach deeper regions in the liver.
The previous studies showed that patients who unexpectedly had to switch to an open procedure during LLR experienced inferior short-term outcomes compared with those who had a successful LLR.7,8 The unplanned conversion is becoming the main concern of LLR.9–11 Meanwhile, some preliminary studies have discussed factors linked to unexpected conversion to OLR during LLR and presented associated risk scores, including the background liver disease, resection scope, tumor location, tumor size, and other factors,12–14 yet the risk factors of unplanned conversion are still controversial.15,16 Moreover, there is limited research examining the impact of unplanned conversion on long-term implications in patients with HCC. Thus, it is urgent to research risk factors and long-term effects of unplanned conversion during LLR for HCC.
This study retrospectively analyzed the clinical data to identify related factors regarding unplanned conversion to an open approach on patients with HCC who underwent LLR, to investigate the intraoperative and postoperative conditions and long-term implications, so as to improve the safety of LLR.
Methods
Patient selection
We retrospectively analyzed data from 96 patients who underwent LLR from January 2017 to November 2022 at the Department of General Surgery in the Second Affiliated Hospital of Guangxi Medical University in Nanning, China. This study was approved by the Second Affiliated Hospital Ethics Committee of Guangxi Medical University (No. 2022-KY-0161). The patients provided their informed consent beforehand.
The inclusion criteria were as follows: (1) LLR for HCC; (2) all patients without portal vein cancer thrombus and active hepatitis; (3) every patient underwent volumetric computed tomography or magnetic resonance imaging before surgery; (4) all patients had Child-Pugh grade A or B liver function 17 ; and (5) patients were in good performance status with an Eastern Cooperative Oncology Group performance score less than 2 points.
The exclusion criteria were as follows: (1) open hepatectomy contraindications; (2) inability to establish CO2 pneumoperitoneum during the operation or failure to insert laparoscopic surgical instruments; and (3) patients requiring hepatic vascular and biliary reconstruction during operation or underwent nonhepatic surgery (except cholecystectomy).
According to whether conversion to laparotomy during the operation, there were two groups: laparoscopic group (Lap) and unplanned conversion group (Conversion). Multiple tumors were regarded as 2–3 tumors. Liver segments II, III, IVb, V, and VI according to Couinaud's classification were considered anterolateral segment (AL), and segments I, IVa, VII, and VIII were identified as posterosuperior segment (PS). All surgeries were performed by the same team of doctors. The Clavien–Dindo Complication Classification system 18 was used to evaluate postoperative complications.
The assessed indicators of risk factors related to unplanned conversion to open surgery are as follows: age, body mass index (BMI), sex, Child-Pugh stage, history of alcohol consumption, surgical history, history of smoking, HBV infection, hypertension disease, diabetes mellitus, liver cirrhosis, alanine aminotransferase (ALT), platelet (PLT), total bilirubin (TBIL), albumin (ALB), alpha fetoprotein (AFP), tumor location, tumor size, tumor number, whether adjacent to vital blood vessels or not, liver resection scope, and intraoperative blood loss. PLT, ALT, TBIL, ALB, and AFP were measured at the last time before surgery. The indicators of factors related to unplanned conversion to OLR during LLR can be found in Tables 1 and 2.
Reasons for Conversion to Laparotomy
Analysis of Related Risk Factors of Unplanned Conversion
Lap group, the patients who underwent laparoscopic liver resection; Conversion group, the patients who underwent unplanned conversion. Surgical history contained upper abdominal surgery, microwave ablation for liver tumor, or alcohol injection for liver tumor. AL, liver segments II, III, IVb, V, and VI; PS, liver segments I, IVa, VII, and VIII.
Indicates using Fisher exact test.
Indicates P < .05.
AFP, alpha fetoprotein; AL, anterolateral segment; ALB, albumin; ALT, alanine aminotransferase; BMI, body mass index; PS, posterosuperior segment; TBIL, total bilirubin.
The intraoperative and postoperative assessed indicators are as follows: operative time, allogeneic transfusion, intraoperative blood loss, postoperative complications (pleural effusion, pneumonia, bile leakage, hepatic failure, postoperative death during hospitalization), and postoperative hospital stay (POS). These indicators were selected as observed indices for clinical analysis. Disease-free survival (DFS) and overall survival (OS) were used as long-term prognostic indicators. Follow-up was conducted by outpatient service or telephone. The start time of follow-up was from the day of surgery, and the end date of follow-up was April 1, 2023.
Operative technique
The patient was placed in a supine position. Five ports were then placed: one above the umbilicus for the laparoscopy and epigastric, upper quadrant, and lateral abdominal working ports. CO2 pressure for the pneumoperitoneum was maintained about 12–14 mmHg during the operation. Intraoperative ultrasonography was performed to assess the characteristics of lesion, including size, location, resection margins, and relationship with the vascular or biliary structures. Pringle maneuver was used routinely. The selective occlusion of hepatic blood inflow was necessarily performed by the extra-Glissonian or intra-Glissonian approach. Hepatic parenchymal transection was performed using ultrasonic dissector and bipolar forceps. The larger structures were controlled with clips. The conversion to OLR was carried out as uncontrolled bleeding or other conditions, including difficulty to operate in the laparoscopy. The management of perioperative period was followed by Chinese Expert Consensus on Enhanced Recovery After Hepatectomy. 19
Statistical analysis
IBM SPSS 23.0 software package (SPSS Statistics, Inc., Chicago, IL) was used to analyze the data. Continuous variables following a normal distribution were expressed as mean ± standard deviation (x ± s), while those not conforming to a normal distribution were indicated by the median [M (IQR)]. In the univariate analysis, continuous data were compared using either the Student's t-test or Mann–Whitney U test. On the contrary, the chi-square test or Fisher's exact test was used to evaluate categorical variables. Logistic multiregression equations were applied to identify independent risk factors, and an unplanned conversion risk assessment equation was established. The equation fitting evaluation used the Hosmer–Lemeshow goodness-of-fit test, while the efficiency of the risk assessment model's prediction was assessed using the receiver operating characteristic (ROC) curve analysis. The discriminatory power was assessed by the area under the curve (AUC).
Values ranging from 0.5 to 0.7 showed a lower diagnostic accuracy, 0.7 to 0.9 represented a moderate diagnostic accuracy, and AUC >0.9 indicated a high diagnostic accuracy. The Kaplan–Meier method analyzed OS and DFS rates, with the log-rank test comparing differences between the two groups. P < .05 was considered statistically significant.
Results
This study encompassed a total of 96 patients undergoing LLR due to HCC. Out of these, 55 patients successfully completed LLR, while 41 patients required an unplanned conversion, yielding a conversion rate of 42.7%. The main reasons for unplanned conversion to laparotomy included uncontrollable bleeding during surgery (24.4%), difficult exposure (31.8%), and adjacent to vital vessels (19.4%) (Tables 1 and 2). In addition, the patients were mainly male patients with age of <65 years (80.2%), most of whom had viral hepatitis B and cirrhosis. The proportion of AL segment tumors with a diameter <5 cm was higher in the Lap group. The Conversion group had a higher proportion of tumors in the PS segment with a diameter of ≥5 cm.
Risk factors linked to unplanned conversion
The characteristics of patients in each group are described in Table 2. There were no significant differences in the two groups, including age, BMI, sex, surgical history, HBV infection, history of smoking, history of alcohol consumption, hypertension disease, diabetes mellitus, liver cirrhosis, Child-Pugh stage, PLT value, ALT value, TBIL value, ALB value, tumor number, and resection scope. These mentioned indicators were not the risk factors for unplanned conversion to laparotomy. Patients experiencing unplanned conversion had larger tumors (P = .001) and more bleeding (P = .000) compared with those who underwent successful LLR. Meanwhile, the tumor location (P = .000), adjacent to vital vessels (P = .021), and AFP (P = .011) may also positively correlate with unplanned conversion.
Subsequently, four preoperative related factors that showed significant correlation in the univariate analysis were examined through multivariate logistic regression analysis, with the results depicted in Table 3. Tumor location (OR, 3.129; 95% CI: 1.214–8.066; P = .018) and tumor size (OR, 2.652; 95% CI: 1.039–6.767; P = .041) were independently associated with conversion. AFP and adjacent to vital vessels were not a risk factor for conversion.
Logistic Regression Analysis of Risk Factors Related to Conversion to Laparotomy
Indicates P < .05.
AFP, alpha fetoprotein; CI, confidence interval; coefficient, regression coefficient; OR, odds ratio; SE, standard error.
Predict logistic regression equation efficacy
Tumor location and tumor size were used as independent variables, and then, the logistic regression equation was established: ln (P/1-P) = −1.706 + 1.141 × tumor location +0.975 × tumor size. The result of the Hosmer–Lemeshow goodness-of-fit test used to evaluate the fitting efficiency of equation was P = .535, indicating that the model was effective.
The predicted value of logistic regression equation was 0.5 as the segmentation point (P ≥ .5 was positive, and P < .5 was negative). The classification table of observed and predicted values assessed by the regression equation is shown in Supplementary Table S1. The ROC curve for evaluating the efficiency of risk assessment model showed that the AUC was 0.772 (95% CI: 0.676–0.869, P = .000), sensitivity was 63.4%, and specificity was 76.4% (Fig. 1), respectively. It demonstrated that prediction efficiency of the risk assessment model was acceptable.
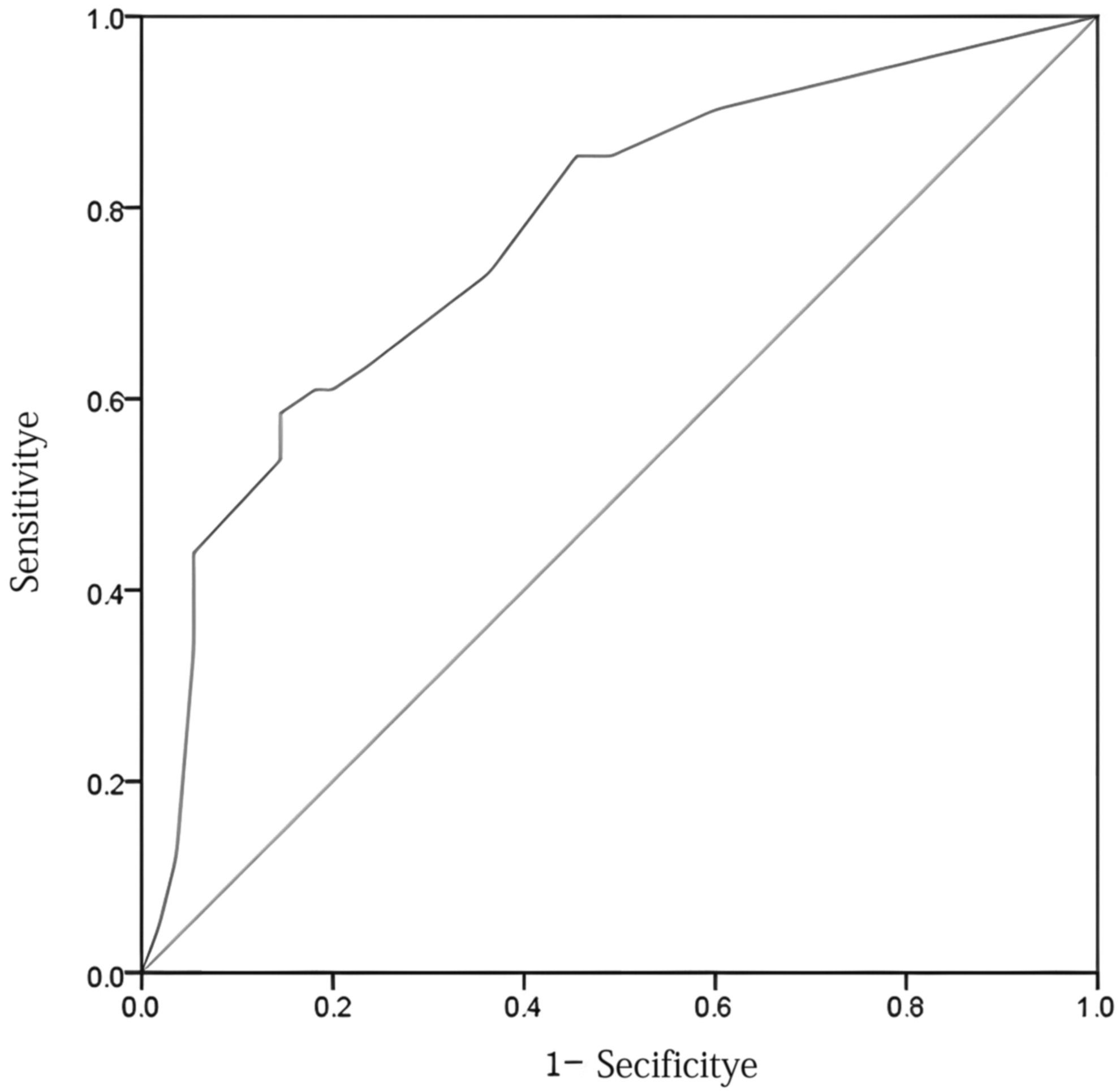
ROC curve of logistic regression equation predicting conversion to laparotomy (area under the curve: 0.772, 95% confidence interval: 0.676–0.869, P = .000; sensitivity: 63.4%; specificity: 76.4%; Youden index: 0.398; cutoff point: 0.44). ROC, receiver operating characteristic curve.
Comparison of perioperative outcomes
The comparison of perioperative outcomes between two groups is shown in Table 4. In patients who experienced an unplanned conversion, the average duration of operation was increased (297.73 ± 98.82 minutes versus 194.03 ± 78.47 minutes, P = .000) and POS was longer (median 8 versus 7 days, P = .003) compared with the Lap group. In addition, the unplanned Conversion group had significantly more blood loss (median 500 versus 100 mL, P = .000) and a higher percentage of blood transfusion (29.3% versus 5.5%, P = .001). The incidence of postoperative pneumonia and postoperative pleural effusion was notably higher in the group that underwent unplanned conversion.
Comparison of Perioperative Outcomes
Lap group, the patients who underwent laparoscopic liver resection; Conversion group, the patients who underwent unplanned conversion.
Values are presented as mean ± standard deviation or number of patients (%).
Indicates using Fisher exact test.
POS, postoperative hospital stay.
Furthermore, the postoperative complications were assessed with the Clavien–Dindo Complication Classification system, shown in Table 4. The incidence of adverse events in the Conversion group was significantly higher than that in the Lap group (85.4% versus 10.9%), and mainly located in Grade II–IIIa.
Comparison of long-term oncologic outcomes
Most of the China liver cancer stage (CNLC) in the Lap group was Ia (36 cases, 65.5%), and most of the CNLC stage in the Conversion group was Ib (25 cases, 61.0%). The postoperative pathology of both groups was mainly moderately differentiated carcinoma. A high proportion of transcatheter arterial chemoembolization (TACE) was carried out in the Conversion group after surgery, shown in Table 5.
Tumor Characteristics and Postoperative Treatment Comparison Between Conversion and Laparoscopic Liver Resection
Lap group, the patients who underwent laparoscopic liver resection; Conversion group, the patients who underwent unplanned conversion.
Indicates using Fisher exact test.
Indicates P < .05.
CNLC, China liver cancer stage; High, highly differentiated carcinoma; Moderate, moderately differentiated carcinoma; Poor, poorly differentiated carcinoma; TACE, transcatheter arterial chemoembolization.
The follow-up period ranged from 0.6 to 62.0 months with a median of 31.0 months in Lap group and from 0.4 to 62.0 months with a median of 29.0 months in Conversion group. The Kaplan–Meier analyses revealed that mean DFS in the Lap group was 30.976 months (95% CI: 23.980–37.971), and the median DFS was 28 months (95% CI: 14.018–41.982). The mean DFS in the Conversion group was 34.436 months (95% CI: 25.94–42.923), and the median DFS was 36 months (95% CI: 14.598–57.402) (Table 6). The log-rank test showed no significant difference (X 2 = 0.201, P = .654) in DFS between the two groups (Fig. 2).

DFS rate of patients who underwent laparoscopic liver resection (Lap) and unplanned conversion (Conversion). DFS, disease-free survival.
Comparison of Disease-Free Survival
Lap group, the patients who underwent laparoscopic liver resection; Conversion group, the patients who underwent unplanned conversion.
CI, confidence interval; SE, standard error.
In addition, the mean OS in the Lap group was 46.283 months (95% CI: 40.007–52.559). The mean OS in the Conversion group was 45.745 months (95% CI: 37.704–53.786) (Table 7). The log-rank test revealed that the OS was not significantly affected by an unplanned conversion during LLR (X 2 = 0.000, P = .986) (Fig. 3).
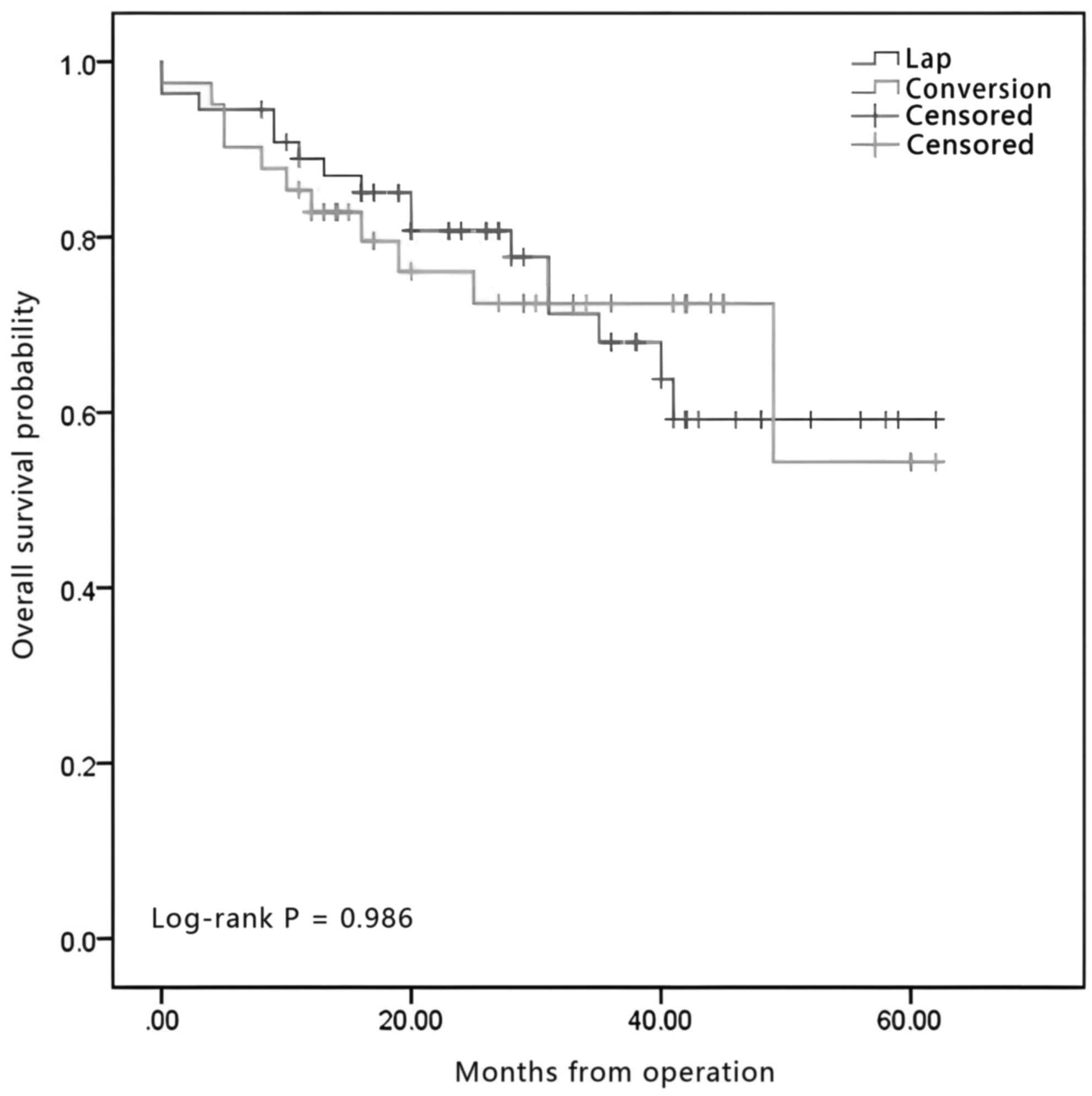
OS rate of patients who underwent laparoscopic liver resection (Lap) and unplanned conversion (Conversion). OS, overall survival.
Comparison of Overall Survival
Lap group, the patients who underwent laparoscopic liver resection; Conversion group, the patients who underwent unplanned conversion.
CI, confidence interval; SE, standard error.
Discussion
According to our study, tumor location and tumor size were independent predictors of conversion. Among them, the highest converted probability was identified in the PS segment, where the diameter of lesion was greater than 5 cm. In addition, the short-term prognosis of converted patients was worse, including longer hospital stays, higher chance of transfusion, and more postoperative complications compared with successful LLR. However, our study did not observe any notable difference in DFS and OS between the two groups.
HCC is one of the most common tumors in the world.20–22 Surgical treatment is still the most effective and important treatment for liver cancer, and minimally invasive hepatectomy assisted by laparoscopy or Da Vinci robotic surgical system has become one of the preferred methods in liver surgery.23,24 However, since laparoscopic maneuver is limited, conversion to laparotomy to ensure the safety of operation is still necessary. Thus, to analyze the related risk factors of conversion to laparotomy so as to reduce the unplanned conversion to laparotomy is an important measure to guarantee the safety of LLR.
Previous studies showed that the intraoperative factor regarding conversion from LLR to laparotomy is usually due to uncontrollable bleeding.11,25,26 In this study, we found that difficult exposure (31.8%) and adjacent to vital vessels (19.4%) were also important reasons for the surgeon to decide to convert to laparotomy during the operation. The previous three indicators are direct risk factors involved in intraoperative conversion; however, these indicators can be only evaluated during the operation. In the event of uncontrollable bleeding, difficult exposure, or adjacent to vital vessels, the difficulty of operation will increase and lead to conversion to laparotomy.
In fact, indirect risk factors are more valuable and practical for surgeons, including patient factors and tumor characteristics. It can be evaluated preoperatively and reduce the chance of unplanned conversion. So far, several studies have evaluated the risk factors for unplanned conversion. Silva et al. believed that hypertension and right hepatectomy were associated with a higher risk of conversion. 9 Cauchy et al. found that elevated BMI, large tumor diameter, and biliary reconstruction were risk factors. 25 Other recent studies found that tumor size, tumor location, prolonged surgical time, and history of upper abdominal surgery were risk factors for unplanned conversion.15,16,27,28
Our study showed that tumor location (OR, 3.129; 95% CI: 1.214–8.066; P = .018) and tumor size (OR, 2.652; 95% CI: 1.039–6.767; P = .041) were independent risk factors. Both the Hosmer–Lemeshow goodness-of-fit test and the ROC curve analysis validated the effectiveness of the risk prediction model. As we know, when the tumor is larger, a broad resection plane will be required, which leads to a higher risk of bleeding. Meanwhile, when the tumor location is difficult to expose, operative difficulty will increase. These factors elevate the risk of conversion.
In addition, the learning curve of surgeon may be an important factor related to the higher conversion rate (42.7%) reported in this study. Previous researches confirmed that the learning curve of surgeons had a significant effect on the conversion rate in LLR.29–31 Furthermore, since laparoscopic hepatectomy was a difficult and complicated operation, the surgeons' experience had a direct relationship with the higher conversion rate.
At present, there are still some controversies about the long-term prognosis of unplanned conversion. Stiles et al. reported that the group with unplanned conversion exhibited lower OS, and this difference was particularly noticeable among patients who underwent open conversion during laparoscopic major hepatectomy. 7 Shin et al. also showed poor perioperative and long-term outcomes after unplanned conversion. 32 In contrast, Lee et al. found that unplanned conversion during LLR did not affect long-term oncologic outcomes. 16
In our study, the DFS and OS between the two groups had no significant difference. This result may be related to postoperative treatment. Liang et al. found that tumor factors and postoperative treatment could affect the long-term prognosis of patients after hepatectomy. 33 In addition, Li et al. showed that postoperative adjuvant TACE could achieve higher OS than surgical resection alone. 34 It can be noted that patients in the Lap group were mainly in Ia stage, while patients in the Conversion group were mainly in the Ib stage. Furthermore, more patients in the Conversion group experienced postoperative TACE. Thus, the postoperative treatment might account for the difference in long-term outcomes between the Conversion group and Lap group in our study.
As for short-term prognosis, the Conversion group was significantly worse than the Lap group. These results were consistent with the previous findings.9,35–37 In particular, complication rates were 15 times higher in the unplanned Conversion group than in the Lap group (36.6% versus 1.8%). Therefore, to reduce unplanned conversion will contribute to improve the short-term outcome of patients.
The limitations in this study are a single-center retrospective analysis and the restricted cases. A large sample and multicenter studies will be still needed in the future.
In conclusion, successful LLR had faster postoperative recovery and more satisfactory short-term outcomes. Unplanned open conversion during LLR for HCC was related to the tumor location and size, but it did not influence the long-term outcomes.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics Statement
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Guangxi Medical University (No. 2022-KY-0161). The patients provided their written informed consent to participate in this study.
Footnotes
Acknowledgment
The authors confirm that this research was carried out without any commercial or financial affiliations that could be perceived as a potential conflict of interest.
Authors' Contribution
Y.Y. and Y.O. designed the project. Y.O., T.L., T.H., Z.X., M.Y., and J.L. collected the data. Y.O., T.L., and Y.Y. wrote the article. Y.H. and X.C. played significant roles in project consultations and in interpreting the results. All the authors participated in crafting the article and approved the submitted version.
Publisher's Note
All views conveyed in this article are exclusively those of the authors and do not necessarily reflect the positions of their associated institutions, or those of the publisher, the editors, and the reviewers. Any product evaluated in this article, or any claim made by its manufacturer, is neither guaranteed nor endorsed by the publisher.
Disclosure Statement
The authors confirm that this research was carried out without any commercial or financial affiliations that could be perceived as a potential conflict of interest.
Funding Information
This work was supported by the Guangxi Natural Science Foundation (2023GXNSFDA026011, Y.Y.), the Scientific Research Project of Guangxi Health Commission (S2021114, Y.Y.), and the Guangxi Medical and health key cultivation discipline construction project (X.C.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.