
Abstract
Background:
Because of lack of an appropriate surgical approach, laparoscopic surgery in patients with left/right Glisson pedicle involvement is still rarely conducted. This study aimed to discusses the methods of intrahepatic Glisson intrathecal dissection via a hepatic parenchymal transection-first approach for laparoscopic hemihepatectomy in patients with left/right Glisson pedicle involvement.
Materials and Methods:
We retrospectively analyzed the clinical data of 21 patients who underwent laparoscopic hepatectomy in the Second Affiliated Hospital, Third Military Medical University (Army Medical University) from March 2021 to May 2022.
Results:
The mean age of the patients was 53.1 ± 11.6 years; mean operation time, 191.9 ± 22.3 minutes; median intraoperative blood loss, 205 mL (160–300 mL); and median length of hospital stay, 8 days (7–9 days). None of the patients underwent conversion to open procedure. Thirteen patients had pathologically confirmed hepatocellular carcinoma (HCC) with portal tumor thrombi (PVTT), and 8 was confirmed hepatolithiasis. Intraoperative frozen pathology and final pathology showed tumor free surgical margins in HCC with PVTT patients. After conservative treatment, all the complications such as postoperative liver section effusion, pleural effusion, pneumonia, intra-abdomen bleeding, and bile leak were cured. During outpatient follow-up examination, no other abnormality was detected. All HCC with PVTT patients were treated with a tyrosine kinase inhibitor after the operation and survived tumor-free.
Conclusions:
Proposed here is a more safe and feasible method of laparoscopic hemihepatectomy in patients with left/right Glisson pedicle involvement, but many problems still needs further exploration.
Introduction
Laparoscopic liver surgery, a widely considered safe and feasible surgical practice without compromising oncological outcome, has expanded from initial local hepatectomy to anatomical hepatectomy. 1 Nowadays, due to the development of surgical techniques and laparoscopic instruments, growing reports have confirmed the feasibility and safety of laparoscopic anatomical hemihepatectomy (LAH) in selected patients.2,3 In LAH, the approach choice for the treatment of left/right Glisson pedicle represents the critical steps. To date, the approaches for the treatment of left/right Glisson pedicle in LAH include Glisson pedicle approach (which can be classified into three types: the extrahepatic, intrahepatic, and transfissural approaches), 4 extrahepatic Glisson intrathecal dissection approach (EHGI). 5
Compared with EHGI, the use of Glisson pedicle approach can reduce operation time, intraoperative hemorrhage, and morbidity. However, for patients with left/right Glisson pedicle involvement, such as portal tumor thrombi (PVTT) 6 and hepatolithiasis, 7 Glisson intrathecal dissection is usually required for portal vein, hepaticartery, and biliary duct isolation, and the Glisson pedicle approach is not appropriate for direct transection of Glisson pedicle. In comparison, it would be more reasonable to apply Glisson intrathecal dissection for treatment. However, EHGI has certain drawbacks. Through constant practice and exploration, we have carried out laparoscopic anatomical liver resection via a hepatic parenchymal transection-first (HPTF) approach8,9 and applied it to intrahepatic Glisson intrathecal dissection (IHGI) in patients with left/right Glisson pedicle involvement. IHGI via HPTF may be a better alternative in selected patients. This study aimed to introduce this strategy for LAH in Patients with left/right Glisson pedicle involvement.
Materials and Methods
Patients
The data of patients who underwent laparoscopic liver resection in our hospital between March 2021 and May 2022 were retrospectively collected. The inclusion criteria in this study were as follows: (1) male or female patients aged between 18 and 75 years old, (2) liver function is graded as Child–Pugh class A or B; (3) left/right Glisson pedicle involvement and histologically confirmed hepatocellular carcinoma (HCC) with PVTT or hepatolithiasis; (4) patients underwent IHGI via HPTF for LAH. The following exclusion criteria were applied: (1) the presence of severe organs dysfunction; (2) patients underwent IHGI via HPTF for LAH combined with other organs resection except for cholecystectomy. Hepatitis B virus patients received standardized antiviral treatment. Prophylactic antibiotic therapy was administered to all patients 30 minutes before surgery and maintained until the second postoperative day.
All patients were treated with a full course of postoperative hepatic function protection, hematischesis, analgesia, rehydration, and other symptomatic and supportive care. Our study protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Third Military Medical University (Army Medical University). This study was performed according to the Declaration of Helsinki, and written informed consent was obtained from individual participant included in the study.
Surgical techniques
All procedures were performed under general anesthesia. Patients were placed in supine in the reverse Trendelenburg position with head up 30° and leg splitting. The monitor was located on the left front of the patient, while the main surgeon stood on the right side of the patient, the camera assistant stood between the spread legs, and the assistant stood on the left side of the patient. Pneumoperitoneum was established and maintained with carbon dioxide at 12–14 mmHg. Low central venous pressure (CVP; <5 cmH2O) is maintained by anesthesia to control blood loss. Five trocars are typically inserted similar to the fan shape around the operation area. A tourniquet for extracorporeal Pringle's maneuver was set using a self-designed occlusion device through a 3 mm incision between left two ports.
Operation began with division of liver ligaments and liver mobilization. Intraoperative ultrasound was performed on the liver surface to determine the courses of middle hepatic vein (MHV). Parenchymal dissection proceeded from the caudal to cranial side along MHV, exposing the MHV on the cutting plane of the liver remnant. Short hepatic veins were clipped. After sufficient opening of the hepatic parenchyma around the ventral and dorsal side of the left/right Glisson pedicle, the left/right Glisson sheath was dissected layer by layer to expose the portal vein and biliary duct completely. According to the condition of the patients, appropriate treatment could be performed, such as accurate portal vein transection after tumor thrombi positioning via ultrasonography (Fig. 1 and Supplementary Video S1); portal vein thrombectomy under direct vision (Fig. 2 and Supplementary Video S2); bile duct transection after full exposure, the opening of bile duct stump, exploration via bile duct stump by choledochoscope, and suture of bile duct stump or placement of T tube drainage (Fig. 3 and Supplementary Video S3).

Accurate portal vein transection after tumor thrombi positioning via ultrasonography.
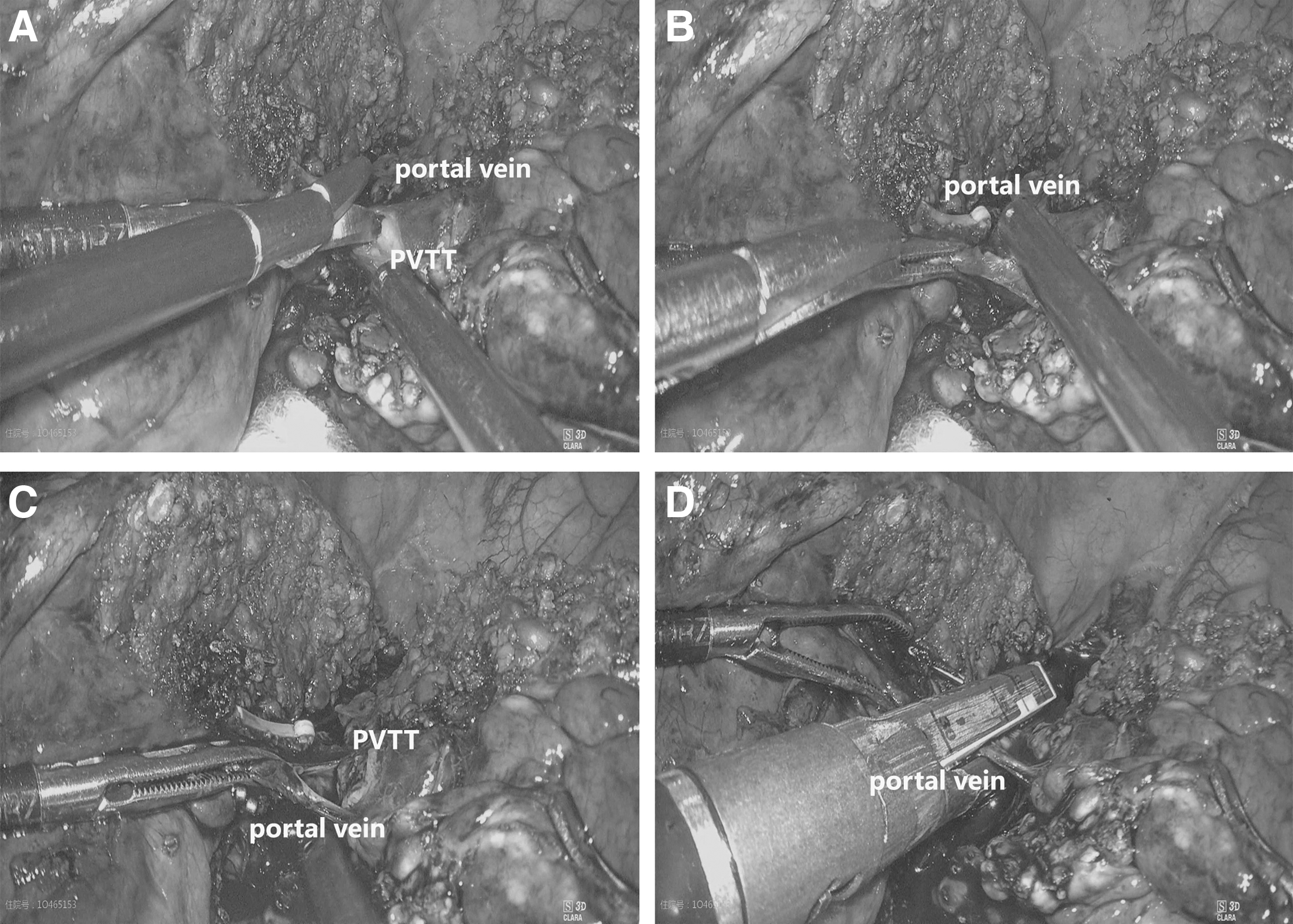
Portal vein thrombectomy under direct vision.
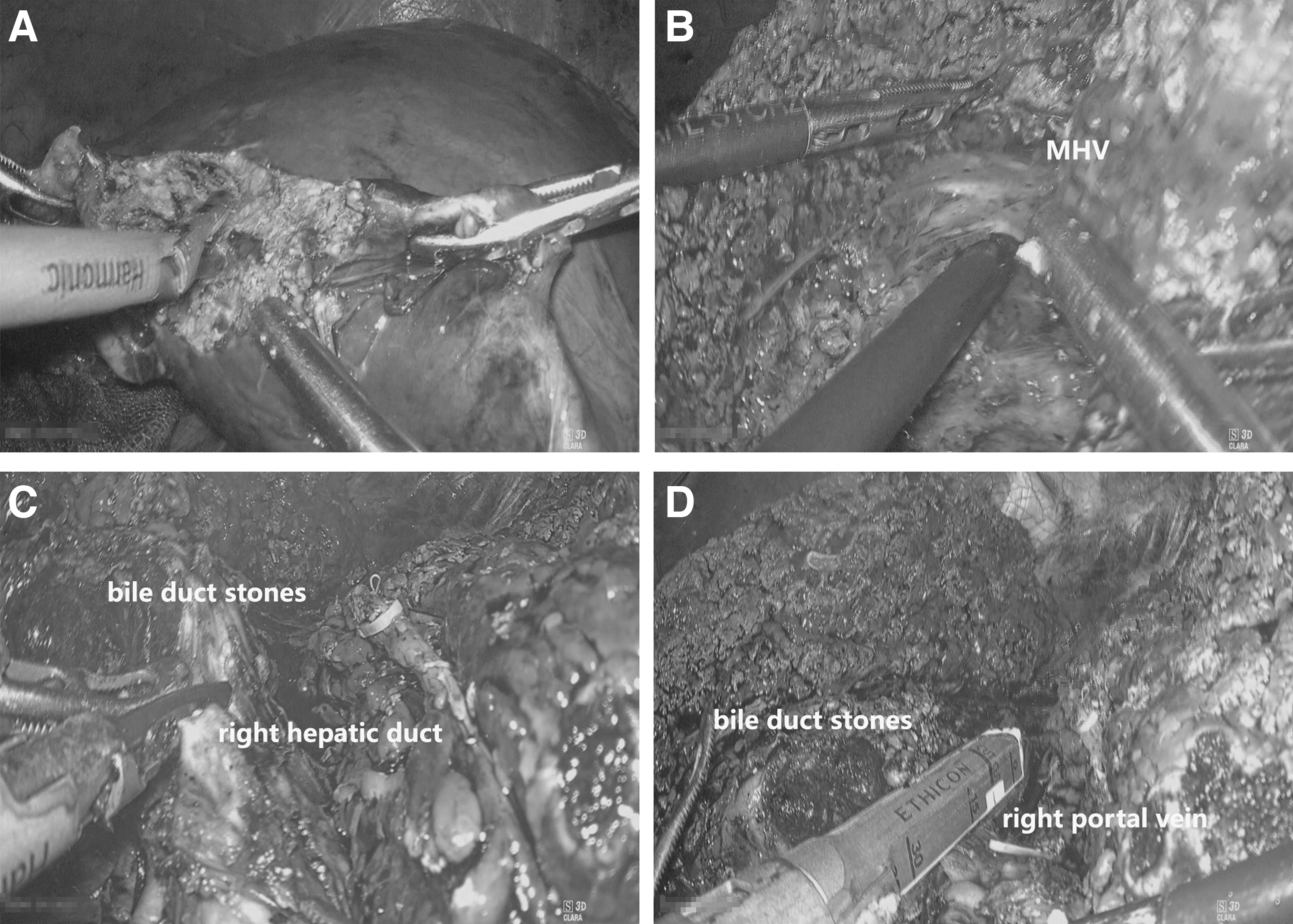
Bile duct transection after full exposure.
Statistical analysis
Data analysis was conducted using SPSS version 22.0 (IBM SPSS, Inc., Chicago, IL, USA). Descriptive statistics was used for analyzing variants. Age, operation time, tumor-free margin, and follow-up time were expressed as mean ± standard deviation and blood loss and postoperative hospital stay were presented as median and interquartile range.
Results
Patients in this study (mean age 53.1 ± 11.6 years) underwent preoperative evaluation, such as blood biochemistry and tumor markers analyses, indocyanine green (ICG) clearance test, imageological examination, and three-dimensional reconstruction. Five patients underwent IHGI thrombectomy for PVTT via HPTF for laparoscopic right hemihepatectomy (LRH); 2 patients underwent IHGI accurate portal vein transection after tumor thrombi positioning via ultrasonography for PVTT via HPTF for LRH; 6 patients underwent IHGI thrombectomy for PVTT via HPTF for laparoscopic left hemihepatectomy (LLH); 3 patients underwent IHGI bile duct open operation for hepatolithiasis via HPTF for LRH; 5 patients underwent IHGI bile duct open operation for hepatolithiasis via HPTF for LLH.
Postoperative pathological analysis revealed that 13 patients were diagnosed with HCC with PVTT. Among the HCC patients, 5 were classified as moderately differentiated, 6 as moderately to poorly differentiated, and 2 as well differentiated. Pathological diagnosis of intraoperative frozen section showed that the portal vein resection margins of the PVTT patients were negative, and the postoperative pathology showed liver and portal vein resection margins were negative. Eight patients had pathologically confirmed hepatolithiasis. No patient is converted to open surgery.
The mean operation time was 191.9 ± 22.3 minutes, median estimated blood loss was 205 mL (160–300 mL), and no blood transfusion cases. The median postoperative hospital stay was 8 days (7–9 days). There was no mortality. According to Clavien Dindo classification, postoperative complications included Grade I complications (pleural effusion, n = 5; liver section effusion, n = 3) and Grade II complications (pneumonia, n = 1; intra-abdominal collection secondary to bile leak, n = 1). No Grade III and above complications occurred. In all cases, the complications were cured by conservative treatment.
All 21 patients were followed, with a mean follow-up time of 15.3 ± 3.8 months. During the follow-up period, none of the 21 patients developed complications such as hemorrhage, bile leakage, and others. During the follow-up, there was no reoperation or perioperative mortality. All HCC with PVTT patients were treated with a tyrosine kinase inhibitor after the operation and survived tumor-free. No recurrence of bile duct stones was reported in hepatolithiasis patients during follow-up.
Discussion
LAH remains a challenging procedure because of technical factors, including the choice of appropriate surgical approach. The choice of laparoscopic surgical approach for anatomical resection of LAH is not simply a “road of entry” but a series of strategic decisions on how to accomplish the surgical goals while ensuring the safety and effectiveness of the surgery. 10
The main approaches for LAH are Glisson approach and EHGI. The Glisson approach, an important technique in LAH, is based on hepatectomy with Glisson pedicle transection proposed by Takasaki. It can be divided into the extrahepatic, intrahepatic, and transfissural approaches.11,12 It has several advantages over standard liver resection including shorter operative time, lower intraoperative hemorrhage, and morbidity. The Laennec capsule can be used as a marker and approach for anatomical hepatectomy. The surgeon can achieve anatomical separation and management of the right/left Glisson pedicle without anatomical damage to the liver parenchyma. The Laennec capsule approach for hepatectomy with Glisson's pedicle transection is essentially an extrahepatic, extrathecal approach that can overcome some of the shortcomings of the conventional extrahepatic, extrathecal approach and is safe and effective. 13
However, for patients with left/right Glisson pedicle involvement, such as PVTT and hepatolithiasis, the use of the Glisson approach was unable to process the intrathecal ducts separately and determine the involved area of the lesion. There might be tumor thrombi dissemination or residue in PVTT patients, 14 and a risk of laparoscopic linear cutting stapler failure for patients with stones, 15 suggesting the requirement of Glisson intrathecal dissection for treatment in the two groups of patients. Glisson intrathecal dissection can realize accurate isolation and processing of the intrathecal duct under direct vision, ensuring the accuracy and safety of processing, which has been applied generally for extrahepatic Glisson pedicle isolation. 5
In general, patients with PVTT and hepatolithiasis show changes in the structure of the hepatic hilum, such as narrow hepatic hilar region, short portal vessels, vascular proliferation, and dense fibrosis in the Glissonian sheath. Moreover, hepatolithiasis patients may have atrophy in the affected hepatic segment and lobe, resulting in torsion and displacement of the hepatic hilum, resulting in greater difficulty in technical operation. Therefore, in clinical practice, for the treatment of the first hepatic hilum intraoperatively, the use of the traditional EHGI for patients with left/right Glisson pedicle involvement was prone to bleeding that was difficult to control.16,17
In view of the difficulty in EHGI due to left/right Glisson pedicle involvement, the key to addressing this problem may be searching for an appropriate method to create sufficient processing space for the Glisson pedicle. We have also carried out relevant research and explored feasible and safe approach. During LAH, we used HPTF guided by the MHV, intrahepatic left/right Glisson pedicle can be treated after fully exposing in the parenchyma and achieved good outcomes.8,9 Therefore, we wondered whether HPTF can be extended for patients with left/right Glisson pedicle involvement. After clinical practice, we proposed IHGI via HPTF for LAH in patients with left/right Glisson pedicle involvement and also standardized the procedure after continuous exploration and improvement.
The key technical points of IHGI via HPTF for LAH in patients with left/right Glisson pedicle involvement can be summarized as follows:
(1) Adequate imageological examination can be used to fully understand the anatomical structure and variation of the intrahepatic intrathecal duct, so as to avoid unnecessary traumatic bleeding owing to isolation blindly.
(2) Intraoperative ultrasound is an important step. As a recommended diagnostic method for PVTT and hepatolithiasis, intraoperative ultrasound has been applied widely in clinical practice. However clinically, there may be inaccurate detection and even unsafe events due to the difference between ultrasonic detection and the actual situation during the operation, as well as the subjective judgment of the operator. Therefore, there is also a need for emphasizing the safe application of intraoperative ultrasonography.
(3) In the first longitudinal liver transection plane, the left/right Glisson pedicle can be temporarily clipped to form the ischemic line, and the preresection line can be determined. In patients with PVTT, there may be a natural demarcation line separating ischemic from nonischemic liver parenchyma due to portal vein embolism; and in patients with hepatolithiasis, there may be a clear boundary between the atrophic liver and the adjacent normal liver, both of which facilitate the identification of the preresection line.
(4) During hepatectomy for hepatolithiasis, ICG-enhanced fluorescence imaging can also be used to successfully locate the intrahepatic affected area and determine the preresection line according to the fluorescence staining boundary for liver parenchyma transection.
(5) Active exposure of the MHV avoids the massive hemorrhage caused by accidental injury of the hepatic vein during the operation; the anatomical level of the Laennec capsule can be fully utilized for blunt separation while separating and protecting the vein. 18
(6) The procedure should be performed under CVP (3–5 cmH2O) and intermittent blockage of the first hepatic portal to reduce the blood oozing from the wound during separation. 19
(7) Full dissection was performed to expose the Glisson pedicle so that creating sufficient processing space for the IHGI.
(8) During IHGI, it is important to apply gentle operation, careful separation, as well as more practical and reliable processing for the treatment of blood vessels in particular. Moreover, for vessels with larger diameters, attention should be paid to prevent the endoclip from falling off and causing massive bleeding, which may increase the difficulty to stop bleeding under the endoscope. If necessary, a linear stapler can be used for processing.
The application value of the IHGI via HPTF in LAH is mainly reflected in the following aspects: (1) It follows the “easy first” strategy and simplifying the surgical procedure somewhat, shortening the operation time, and improving the safety of the operation. (2) Enough space for operation can be created to realize precise intrahepatic operation for left/right Glisson pedicle involvement. (3) Contact and compression to the tumor can be reduced during operation, associated with in situ hepatectomy, which is more in line with the principle of the nontouch isolation technique. The ineffective liver tissue without inflow and outflow tract can be completely removed; the possibility of postoperative tumor recurrence and postoperative complications can be reduced, so as to improve the survival rate of patients.
Several limitations for the current study may, such as retrospective analysis, be a single-center experience with small sample size, and short follow-up period, may introduce potential selection bias. Additionally, the learning curve in the laparoscopic approach may limit the reproducibility of these results. Laparoscopic surgery for PVTT under pneumoperitonium has the potential advantage of being minimally invasive, providing better visualization and avoiding tumor residuals, but it is technically more difficult to perform, especially in case of extended thrombosis. Therefore, it should be performed by surgeons with expertise in hepatic surgery and minimally invasive technique in and in selected patients. Compression and crushing of PVTT during laparoscopic thrombectomy under pneumoperitonium could be avoided and new intrahepatic metastases caused by tumor thrombus to the remnant liver minimized. Although these patients cannot be cured by surgery alone, early adjuvant therapy followed by laparoscopic surgery might contribute to a good outcome.
Clinical studies with a high level of evidence are still necessary to gain further experience and make up the insufficiency in current research.
Conclusions
Laparoscopic treatment of the patients with left/right Glisson pedicle involvement is still a great challenge that necessitates the development of a reasonable and safe surgical procedure with a definite curative effect. Data from currently research suggest that IHGI via HPTF for LAH in patients with left/right Glisson pedicle involvement is a safe and feasible procedure; however, high-quality research is still needed.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the general program of Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau; Grant No. 2023MSXM004).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.