
Abstract
Introduction:
Reported results and techniques of laparoscopic sleeve gastrectomy (LSG) are variable. Our objective was to assess results of weight loss, complications, and reflux in a large consecutive series of LSG, describing technical detail which contributed to outcomes.
Methods:
Retrospective review of prospectively collected data of 500 consecutive patients undergoing LSG. Patient demographics, weight loss, complications, and functional outcomes were analyzed and operative technique described.
Results:
Five hundred patients underwent LSG over 3 years (2 revisional). Mean (range) preoperative body mass index was 40 kg/m2 (32–75 kg/m2). Mean follow-up and length of hospital stay were 12 months (1–36) and 7.2 days (5–12), respectively. All-cause 30-day readmission rate was 0.3%. Mean excess weight loss was 22.3% (1 month), 42.2% (3 month), 57.2% (6 month), and 73.1% (1 year). There was no mortality and intraoperative complications occurred in our 500 cases. Early surgical complications in 2 (0.2%) patients (postoperative bleeds). Gastro-oesophageal reflux symptoms decreased about 10%.
Conclusion:
With attention to detail, LSG can lead to good excess weight loss with minimal complications. Tenants to success include repair of hiatal laxity, generous width at angula incisura, and complete resection of posterior fundus.
Introduction
Obesity has become a major public health issue in China. 1 The clinical management and treatment of obesity face enormous challenges and opportunities. 2 Laparoscopic sleeve gastrectomy (LSG) has become a standard surgical procedure for the treatment of obesity, and it can also significantly improve obesity-related diseases, such as type 2 diabetes, hypertension, and high cholesterol. 3 However, as a functional surgery, any complications associated with LSG, such as gastric leak and bleeding, can have significant negative impacts on patients. These complications can lead to prolonged hospital stays, additional surgeries, and in some cases, even death.
This article aims to illustrate the community practice experience of a surgeon who performed 500 consecutive LSG procedures. We believe that discussing technical considerations that can help reduce the risks of gastric leakage and bleeding is important.
Methods
A retrospective analysis was conducted on 500 LSG procedures performed by a single surgeon at Shanxi Bethune Hospital from January 2010 to May 2023. All patients signed an informed consent form before surgery. Inclusion and exclusion criteria were based on Chinese guidelines for surgical treatment of obesity and type 2 diabetes 4 :
Inclusion criteria
Clear diagnosis of obesity with a body mass index (BMI) >32.5 kg/m2.
BMI ≥27.5 kg/m2 with poorly controlled traditional treatment, presence of at least two features of metabolic syndrome, or complications.
25 ≤ BMI <27.5, waist circumference for men ≥90 cm, and for women ≥85 cm, and reference imaging examination suggests central obesity.
Exclusion criteria
Obesity caused by physical factors or medications, including Cushing's disease, hypothyroidism, or drug-induced obesity
Presence of clear contraindications for surgery
Pregnancy or lactation
Surgical technique
After successful anesthesia, sterilize the operation area and lay down a sterile drape. Make a 1 cm incision just above the navel and puncture the abdominal wall with a 10 mm trocar to establish CO2 insufflation, then introduce a laparoscope into the abdominal cavity. Place a 12 mm trocar 10 cm to the right of the navel and a 5 mm trocar 10 cm to the left of the navel along the midline just below the xiphoid process. Insert atraumatic forceps below the xiphoid process to shield the left lobe of the liver. Using an ultrasound scalpel, closely follow the greater curvature of the stomach, separating it from the omental tissue. The dissection should extend from approximately 1.5 cm to the left of the His angle, at the esophagogastric junction, down to about 4 cm from the pylorus. Introduce a 36 F gastric tube orally. At a point approximately 5 cm from the pylorus, use a laparoscopic linear stapler to remove the greater curvature of the stomach, encompassing the gastric tissue surrounding the 36 F gastric tube, effectively transforming the residual gastric cavity into a tube-like structure of approximately 100 ml in volume. Suture the serosal and muscular layers of the stomach's incised edge with absorbable sutures in a continuous manner. Remove the excised stomach tissue through the 12 mm trocar on the left side. Verify the absence of active bleeding, deflate the CO2 insufflation, remove all trocars, and suture the incisions.
Results
A retrospective evaluation was conducted on a chart of 500 consecutive patients who underwent LSG in our center from January 2013 to May 2023. The summary of patients' weight, BMI, age, and gender is presented in Table 1. Among the 500 patients, 42 (8.4%) were classified as super-obese (BMI ≥55).
Demographics of the 500 Sleeve Gastrectomy Patients
Values represent mean ± standard deviation.
The overall complication rate of the 500 patients was 3.2%, with a readmission rate within 30 days after surgery of 1.7%. There were no reported deaths among the 500 patients. One patient experienced bilateral lower limb weakness and numbness 1 month after surgery, which was later diagnosed as Guillain–Barré syndrome. There were no leaks observed among the 500 cases of consecutive sleeve gastrectomy. The most common complications were acid reflux and vomiting (6 cases) and numbness in the Vastus lateralis muscle (5 cases), while other complications were less prevalent (Table 2). Data on weight loss were collected through self-reported weight combined with telephone, text message, and WeChat communication. Complete follow-up data within the first year were available for 131 patients (Fig. 1).
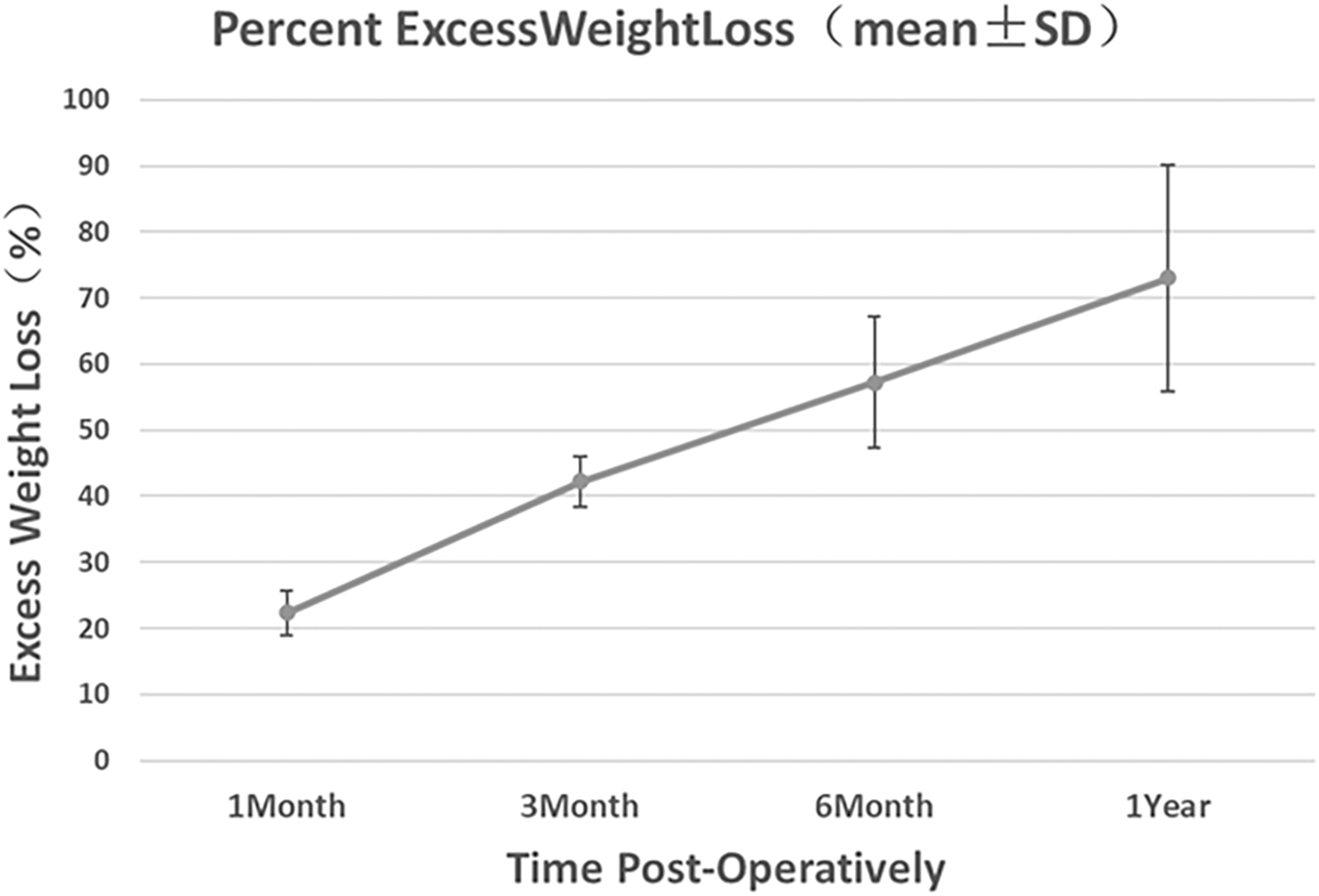
Percent excess weight loss: Mean excess weight loss of 131 cases out of 500 patients was 22.3% (1 month), 42.2% (3 month), 57.2% (6 month) and 73.1% (1 year). SD, standard deviation.
Complications in 500 Sleeve Gastrectomy Patients
Discussion
With the rapid development of China's economy and the improvement of living standards, the number of obese patients is increasing year by year, leading to an increasing demand for weight loss surgery in China. 5 LSG is a minimally invasive weight loss surgery technique that involves removing most of the stomach using laparoscopic technology to create a narrow gastric sleeve. This surgery can significantly reduce the capacity of the stomach, limit food intake, and achieve weight loss. 6 LSG is suitable for patients with severe obesity, especially those with accompanying diseases such as diabetes and hypertension. 7
Currently, LSG has become one of the routine surgical methods for treating obesity in China. 8 According to statistics, as of 2021, the number of LSG surgeries in China has reached the second highest globally, second only to the United States. 9 More and more hospitals and doctors are receiving training and practicing LSG surgery, and achieving good surgical results. In addition, due to the advantages of LSG such as minimal surgical trauma and fast recovery, it is becoming increasingly popular among patients.
However, LSG still faces certain challenges and problems in its development in China. Due to the surgical operation's complexity, complications such as gastric leakage and bleeding may occur.10,11 Our center has reported 500 cases of LSG, all performed by a single surgeon, and none experienced gastric leakage. We would like to share some of our surgical techniques, which may provide reference for other centers to perform this type of surgery.
The location and number of trocars used in LSG can vary depending on the surgeon and their surgical habits. Jiang et al. analyzed 20,180 patients who underwent LSG and found that the number of trocars used varied in different studies, with four or five trocars being the most commonly used. The trocars were typically placed in an inverted trapezoid or left-predominant pattern. Single-incision LSG does not increase the risk of complications, but it can prolong the operation time. 12 In our series of 500 LSG cases, 412 were performed using four trocars and 88 were performed using three trocars, with a 5 mm trocar placed below the xiphoid process. The site of trocar insertion and surgical positioning can be found in Figure 1. For patients with a BMI ≥32.5, four trocars may be preferred to reduce the difficulty of the operation. It is routine for us to administer subcutaneous injections of ropivacaine at the trocar site postoperatively to prevent patients from experiencing pain.
In a study of 422 patients undergoing LSG conducted by Velotti et al., 13 there were no statistically significant differences in operative time or intraoperative and postoperative complications when comparing the use of LigaSure and Harmonic electrosurgical devices. In our practice, we have performed 500 LSG procedures using the Harmonic device, with our surgical approach being largely similar to that proposed by Chung et al. 14 We begin the dissection at the middle of the stomach, and when cutting the greater omentum, we use distal electrocoagulation and proximal electrosection, employing “a two-knife technique” to successively divide the stomach and omentum. When dissecting the short gastric vessels and posterior gastric artery, we utilize Hemo-lock clips for secure occlusion. Preserving pyloric function is crucial, as it is key to preventing postoperative gastric leakage. Therefore, we choose to retain ∼5 cm of the omentum near the pylorus to ensure its blood supply. Similarly, we maintain a distance of about 3 cm from the cardia.
There is currently a debate on whether to use sutures for reinforcement after completing the gastrectomy closure. A prospective study 15 compared the use of sutures for reinforcement during LSG surgery and concluded that reinforced sutures can reduce the bleeding rate, but do not affect the gastric leak rate. We use 4-0 inverted needles for reinforcement during surgery, with a 1 cm needle spacing. Compared to the reported probability of postoperative gastric leakage in the literature, 16 none of the 500 laparoscopic sleeve gastrectomies we performed had any gastric leaks.
Conclusion
LSG has shown promise as both a primary bariatric procedure and a staged procedure for high-risk patients. Our data indicates that LSG can be successfully performed in a community practice, with a low complication rate and satisfactory medium-term weight loss. However, it is crucial for surgeons performing LSG to minimize the risk of creating strictures at the incisura angularis and stapling near the esophagus at the angle of His. And for beginners in this field, it is important to carefully select patients with lower BMI as a means to overcome the initial learning curve as quickly as possible. It is worth mentioning that our study has major weaknesses, including limited follow-up rates, reliance on self-reported weight data, and a lack of primary pressure-volume measurements.
Footnotes
Acknowledgment
We thank Q.Y.X., for collection of data.
Authors' Contributions
M.K.: Conceptualization, Methodology, Writing—Original draft. Q.Y.X.: Data curation. Z.X.Z.: Visualization, Investigation. H.J.L.:Writing—Reviewing and Editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Shanxi Province “136 Revitalization Medical Project Construction Funds”.