
Abstract
Background:
We previously described sleeve gastrectomy with jejunoileal bypass (SGJIB) as promising novel technique for the surgical treatment of obesity
Methods:
A retrospective analysis of a prospective database in a Private Practice of Alimentary Tract Surgery in São Paulo, Brazil. We analyzed 176 patients with 60 months of follow-up, 74 of whom underwent Vertical Sleeve Gastrectomy with Jejunoileal Bypass (VSG-JIB) (50 women and 24 men) with a mean age of 38 years and a mean body mass index (BMI) of 40 kg/m2, and 102 patients underwent Roux-en-Y gastric bypass (RYGB) (90 women and 12 men) with a mean age of 36.5 years and a mean BMI of 39.73 kg/m2.
Results:
There was no statistically significant difference in long-term weight loss between the two groups. The rate of postoperative complications immediately after surgery was similar, but there was a tendency toward less severe complications in the SGJIB cohort.
Conclusion:
Sleeve gastrectomy with jejunoileal bypass is a novel surgical procedure for weight loss with comparable efficacy and safety compared with laparoscopic RYGB.
Introduction
Obesity is a complex condition that leads to changes in body structure and is associated with several comorbidities, such as type 2 diabetes mellitus (T2DM), hypertension, sleep apnea, asthma, coronary heart disease, and cancer.1–5 In the United States, to treat morbid obesity, laparoscopic sleeve gastrectomy is the most employed operation followed by Roux-en-Y gastric bypass (RYGB). 2 Randomized clinical trials have demonstrated long and sustained weight loss after both techniques. 6 RYGB has been associated with greater weight loss and lower incidence of de novo gastroesophageal reflux, 7 with the disadvantage of higher complication rates and reoperation. 8
Depending on the country of origin and other socioeconomic factors, weight regain of around 10% to 29.5% in 5 years has been observed in sleeve gastrectomy. 9 Currently, 5% to 10% of patients require revisional surgeries due to weight regain with sleeve gastrectomy. 10 To reduce this weight regain, we 11 proposed to associate jejunoileal diversion with the restrictive method, turning the operation into a mixed technique, vertical gastrectomy with jejunoileal bypass. To analyze long-term weight loss and complications of this novel intervention, as it compares to laparoscopic RYGB, we designed a cohort study comparing both interventions.
Methods
Institutional Review Board
This study was reviewed by the University of São Paulo Medical School Institutional Review Board and received approval on September 2012, and is registered in the Brazilian registry Plataforma Brasil (protocol 03066112410010065). All patients provided informed consent before the surgical intervention and study inclusion.
Study design
This was retrospective analysis of a prospective database. Patients were selected to either conventional gastric bypass or the novel surgical procedure. Patients were followed by a period of 60 months, to account for weight loss, short-term and long-term surgical complications. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cohort studies was used as a methodological reference for writing this research report.
Cohort abstraction
The following data were abstracted: sex, age, comorbidities, height, weight, and immediate postoperative complications such as bleeding, anastomotic leak, intestinal obstruction, reoperation, and deaths that occurred within the 30 days after the surgical procedure. In addition, late complications were evaluated, which were defined as weight regain, malnutrition, incidence of cholecystolithiasis, gastroesophageal reflux, reoperation, and deaths within a period of 60 months.
Sample size and power calculation
We estimated that to detect a mean difference of 2 points in body mass index (BMI), with a standard deviation (SD) of 2, an Alpha of 0.05 and 80% power, we would need a minimum sample size of 34 patients (17 in each group).
Inclusion criteria
Age greater than 18 years and less than 65 years.
Diagnosis of Grade III obesity without comorbidities or Grade II obesity with comorbidities, according to World Health Organization (WHO) definitions. 12
Underwent SG with jejunoileal bypass or RYGB as primary surgery by video laparoscopy.
Exclusion criteria
Revisional surgery.
Age less than 18 years or greater than 65 years.
Novel procedure description—sleeve gastrectomy with jejunoileal bypass
Five trocars were placed, the first one being a 10 mm trocar for the 30° optics, 10 cm above and 7 cm to the left of the umbilicus; the second one being a 12 mm trocar for the surgeon's right working hand and the introduction of staplers, 3 cm below the left costal margin, in the left midclavicular line; the third one being a 12 mm trocar for the surgeon's left working hand and the introduction of staplers, 6 cm below the right costal margin, in the right midclavicular line; the fourth one being a 5 mm trocar at the level of the xiphoid appendix for the placement of the liver retractor; and the fifth one being a 5 mm trocar for the introduction of auxiliary forceps, parallel to the optic trocar, in the left flank, in the anterior axillary line. The surgeon begins with either jejunoileal bypass or vertical sleeve gastrectomy. Vertical sleeve gastrectomy is conducted, significantly constricting the stomach. Gastric devascularization starts at the antrum, about 3 to 4 cm from the pylorus, liberating the greater curvature until the fundus, with a meticulous dissection of the esophagogastric angle, short gastric vessels, and the posterior aspect of the fundus.
After this release, a 12 mm Fouchet probe is introduced, transduodenally, to mold the gastric curvature and also delimit the remaining stomach's caliber. The stomach resection starts from the antrum, using a green cartridge. It is important that the staple line be molded by the intragastric probe, seeking to create a gastric tube of about 20 mm in diameter. The section continues under direct vision to the esophagogastric angle, performed on continuous seromuscular sutures using a Polydioxanone (PDS) thread. For the jejunoileal bypass, the inframesocolic duodenojejunal angle—Treitz ligament—is initially identified. The jejunum is measured along its antimesenteric border over an extent of 80 cm. At this level, a suture is applied to repair and anchor the jejunal loop to the stomach, to identify it later. Six centimeters below, another suture is applied to define the distal level of the jejunal loop and facilitate the subsequent position of the ileal loop. After this step, the ileocecal valve is identified, and 120 cm of the distal ileum is measured, also along the antimesenteric border, in a cranial direction. The distal point of this ileal loop is sutured to the proximal point of the jejunal loop.
The already repaired distal point of the jejunal loop is sutured to the proximal point of the ileal loop. This way, a presentation for the lateral–lateral jejunoileal anastomosis is created. Then, using a 45 mm white-loaded stapler, the jejunoileal anastomosis is performed. The repair sutures are cut and removed. This way, an intestinal bipartition is created, with the entire intestinal transit located to the left in the abdominal cavity. The mesenteric gap is closed using nonabsorbable thread to avoid internal hernias.
Standard procedure description—RYGB
Our comparator was a standardized laparoscopic RYGB. 13 The patient receives general anesthesia, in a horizontal supine position with semilithotomy tilt, and the surgeon positioned between the patient's legs. Five trocars are placed: a 10 mm trocar for the optical scope, 5 cm above and to the left of the umbilicus; another 12 mm trocar in the left midclavicular line, 2 cm below the left ribcage margin; another 12 mm trocar in the right midclavicular line, 5 cm below the right ribcage margin; 1 parallel 5 mm trocar to the optical port, located 10 cm away from it on the left flank; and finally, the fifth trocar at the level of the xiphoid appendix for liver retractor placement.
The first step involves dissecting the esophagogastric—Hiss—angle, exposing the left arm of the left diaphragmatic pillar. A Fouchet catheter is inserted orally to shape the gastric pouch and gastrojejunostomy. A hole is made on the lesser curvature, near the perigastric area, about 5 to 7 cm from the esophagogastric junction. The stomach is horizontally divided using a laparoscopic linear stapler in a section of about 4 cm. A vertical incision is made in the stomach, parallel to the lesser curvature, toward the molded angle of His under a 32Fr Fouchet catheter.
Moving to the inframesocolic area, the Treitz angle is identified, and the biliary limb is isolated with an extension of about 80 cm. The transition between the alimentary limb and the biliary limb is marked at this level. The unit is lifted to the supramesocolic area, and a gastrojejunostomy is performed by inserting a laparoscopic linear stapler at the distal point of the gastric pouch and the jejunal loop. The stapler gap is closed with extramucosal sutures using 3-0 PDS thread. Next, a 120 cm alimentary segment is measured, and it is anastomosed to the bile loop using a laparoscopic linear stapler. The stapler gap is closed with extramucosal sutures using 3-0 PDS thread.
The integrity of the anastomoses is tested using Methylene Blue solution. The mesenteric gap is closed with continuous sutures of Ethibond® 3-0. The bile loop is separated from the alimentary loop using a laparoscopic linear stapler. The abdominal cavity is drained.
Primary objective
The primary objective of this study was weight loss and maintenance in patients undergoing SG with Jejunoileal Bypass versus RYGB.
Secondary objectives
Evaluate the immediate and long-term complications of Sleeve Gastrectomy with Jejunoileal Bypass (SGJIB) and RYGB.
Evaluate the safety of the two operations.
Evaluate the Clavien–Dindo 14 complication score of the two operations. This is a validated score to address the severity of postoperative complications, with scores 3 or higher requiring nonpharmacological interventions, denoting greater severity.
Statistical analysis
In the present research, data were tabulated in an Excel® spreadsheet (Microsoft 365®, 2019) and statistically analyzed using STATA software, version 17. For descriptive analysis, absolute quantities, measures of central tendency (mean and median), and distribution (minimum, maximum, and percentage) were used, and the Student's t-test was applied. Unadjusted relative risks were obtained for primary and secondary outcomes using the chi-square test. Adjusted relative risks (corrected for age, sex, hypertension, diabetes mellitus, liver disease, presence of neoplasm, heart failure, smoking, peripheral vascular disease) were obtained using Poisson Regression. We also conducted propensity-score match analysis pairing by the same variables to estimate treatment effects. Statistical significance was set at P value <.05.
Results
A total of 176 patients, 74 patients underwent SGJIB and 102 patients underwent RYGB. In the SGJIB group, there were 50 (65.79%) women and 24 (34.21%) men. Of this total, 26 patients had systemic arterial hypertension (SAH) (35.14%), and 10 patients had T2DM (13.51%). The median age observed in this group was 38.24 years (SD = 12.11). The median BMI was 40 kg/m2 (SD = 4.10). In the RYGB group, 90 (81.82%) were women and 12 (18.18%) were men. Forty-three (38.74%) had SAH, and 27 (24.55%) had T2DM. The median age was 36.57 years (SD = 10.42), and the median BMI was 39.63 kg/m2 (SD = 5.25). Demographic characteristics are summarized in Table 1.
Demographic Characteristics of Two Cohorts
BMI, body mass index; RYGB, Roux-en-Y gastric bypass; SD, standard deviation.
Long-term weight loss
Weight loss after 60 months was assessed in the SGJIB and RYGB groups. The median BMI was 28.265 (SD = 7.144) in the SGJIB group and 28.04 (SD = 4.91) in the RYGB group. There was no statistically significant difference in long-term weight loss between the two groups, with a P value of .4629. Final weight loss is presented in Figures 1 and 2.
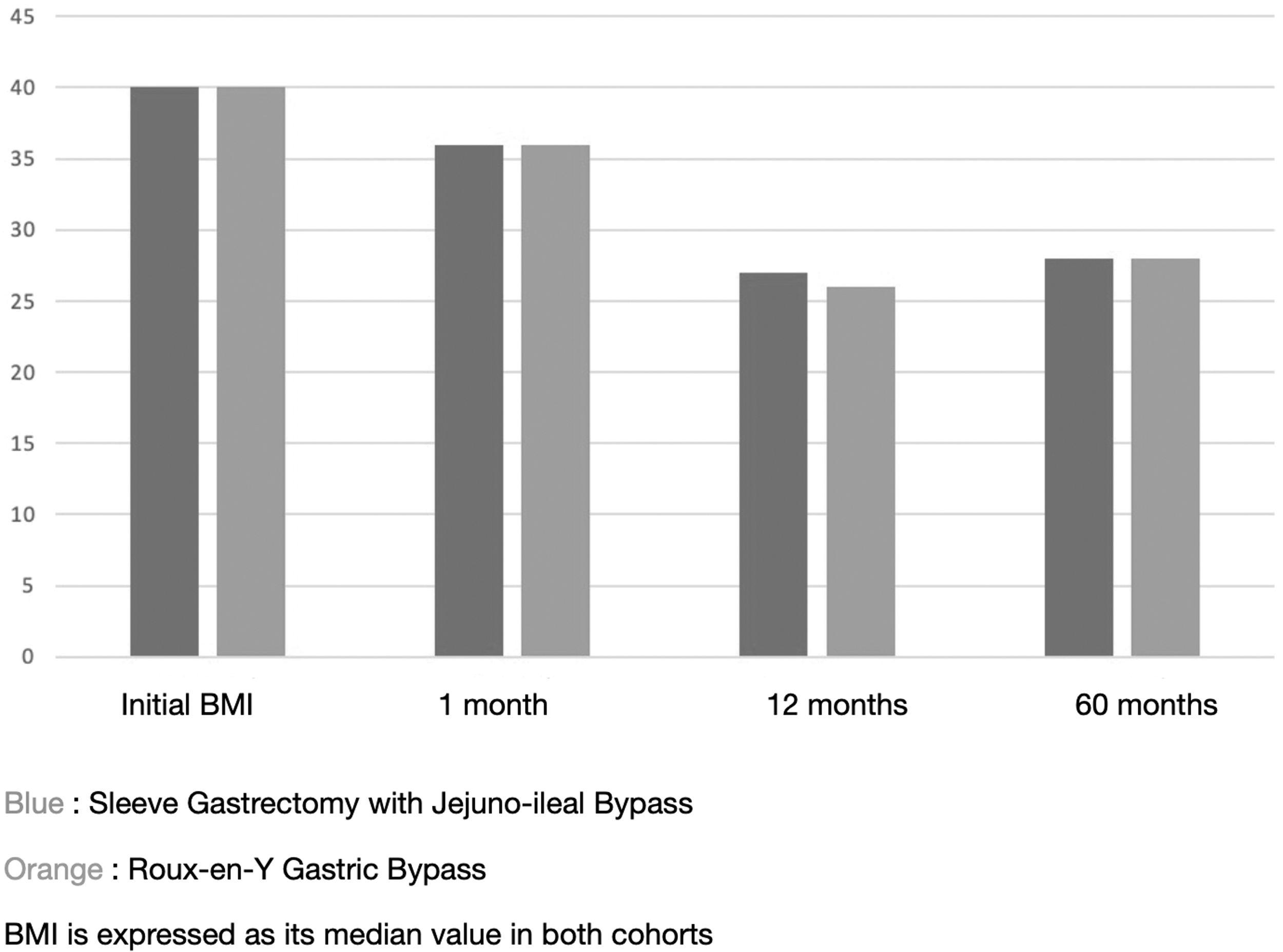
Time trends for weight loss. RYGB, Roux-en-Y gastric bypass.
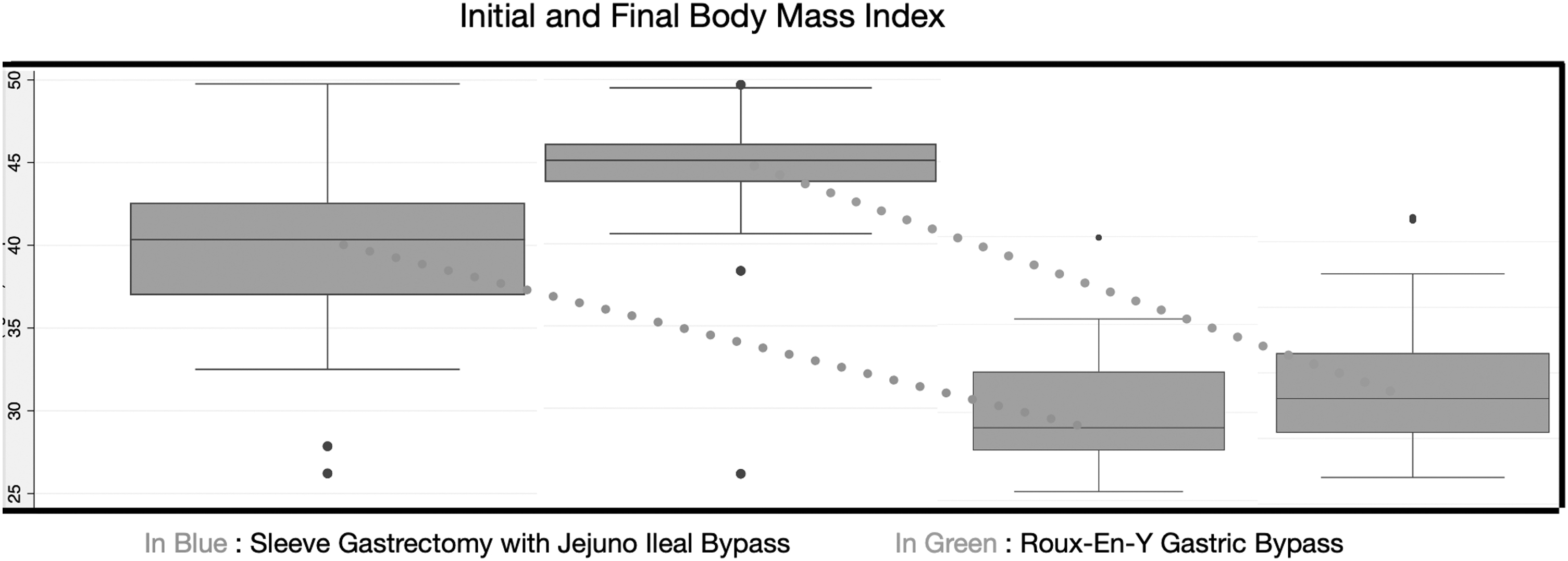
Initial and final BMIs for both cohorts. BMI, body mass index; RYGB, Roux-en-Y gastric bypass.
Immediate postoperative complications
Immediate postoperative complications in the SGJIB group were intra-abdominal hemorrhage in one case requiring reoperation and one case of small bowel bleeding treated endoscopically. In the BYGR group, one case of intra-abdominal bleeding requiring reoperation and one case of hemodynamic instability were observed. There was no statistically significant difference between the groups (relative risk [RR]: 1.63, 95% confidence interval [CI]: 0.21–12.58, P = .636) after multivariate adjustment for the incidence of complications in the immediate postoperative period.
Late postoperative complications
The overall incidence of late postoperative complications was 12.23%. In the SGJIB group, 12 (15.79%) patients had complications, and in the Roux-enY gastric Bypass (RYGB) group, 11 (9.91%) patients had complications. The complications in the SGJIB group were reoperation for internal hernia in four (4.32%) cases and malnutrition in three (3.24%) cases. In the RYGB group, the complications were reoperation to reverse jejunoileal diversion due to malnutrition in six (7.7%) cases and four (4.62%) cases of cholelithiasis. There was no statistically significant difference in the incidence of late postoperative complications between the groups (RR: 1.59, 95% CI: 0.74–3.42, P = .229).
Clavien–Dindo complication score
The Clavien–Dindo complication scores of immediate and late postoperative complications were analyzed according to the classification between the groups. The prevalence of a score equal to or greater than 2—indicating major postoperative complications—was observed in 4.9% of the SGJIB patients and 6.53% of the RYGB patients. SGJIB was associated with a significantly lower Clavien–Dindo score compared with RYGB, even after adjustment (RR: 0.56, 95% CI: 0.32–0.96, P = 0.036).
Gastroesophageal reflux
Gastroesophageal reflux incidence was defined as de novo clinical and/or endoscopic diagnosis of gastroesophageal reflux disease. Long-term incidence of gastroesophageal reflux with clinical or radiological repercussions was compared between the two groups. SGJIB was associated with an incidence of gastroesophageal reflux in five (6.58%) cases and RYGB had one (0.90%) case recorded (RR: 7.30, {95% CI: 0.87–61.27}, P = .0305). After multivariate adjustment, there was no difference between the groups (RR: 5.61, {95% CI: 0.54–57.92}, P = .147).
Propensity-score match
We included propensity-score match analysis with treatment effects and logit model in our study to adjust for clinical and demographical differences between the two groups for weight loss and long-term surgical complications. There was no significant difference for weight loss (Coef. = 3.54, P = .440) and for long-term complication incidence (Coef. = 0.017, P = .794).
Discussion
In this prospective cohort, including 176 patients, SGJIB showed safety and efficacy comparable to RYGB, an already well-established weight loss surgery in safety and efficacy. Analyzing the incidence of immediate postoperative complications, both groups had a low incidence of adverse events (less than 2%). In both interventions, the incidence of postoperative bleeding was the most frequent adverse event, but with low incidence in this cohort. It is known that at that time older stapling technology utilized in the beginning of this cohort could also contribute to higher incidence of digestive bleed. These findings corroborate the safety of RYGB, already demonstrated in decades of studies, and show our novel technique as an option with equivalent short-term safety and efficacy.
The incidence of late postoperative complications (cases of intestinal obstruction, reoperation, malnutrition, or cholecystolithiasis) did not differ significantly between the two groups. The severity of late postoperative complications was also analyzed using the Clavien–Dindo score. This score is a validated tool for analyzing the severity and need for intervention of postoperative complications. The VSG-JIB group presented a significantly lower score, indicating lower severity of complications, compared with the BGYR group. The difference remained significant even after multivariate adjustment, with a significant reduction in score equal to or greater than 2 in the GVDJ group. One possible reason is that our novel intervention requires only one anastomosis, and also is of lower risk than the gastrojejunal one in our comparator.
It is noteworthy that a significant portion of patients in the SGJIB group underwent reoperation to undo the jejunoileal diversion, usually associated with severe malnutrition cases. This finding may indicate that SGJIB has an important malabsorptive component that can lead to malnutrition as frequently as RYGB. The excluded segment measures around the total small bowel length minus 210 cm for the SGJIB cohort. However, the overall incidence of reoperation was still significantly lower than the one of RYGB, validating the safety of this novel procedure. Further studies can elucidate the long-term malnutrition effect of our novel intervention in larger samples.
A well-established and important limitation of conventional sleeve gastrectomy is the increase in gastroesophageal reflux previously diagnosed or the development of new symptoms of this pathology. On the other hand, RYGB has a proven effect of reducing gastroesophageal reflux. Therefore, the incidence of this symptom was compared between the two groups. The results indicated a higher relative risk for gastroesophageal reflux in the SGJIB group compared with the BGYR group. However, after multivariate analysis, this difference was not considered statistically significant. Future studies involving SGJIB should analyze this specific outcome. Of note, this result does not limit the indications for this novel procedure, because the already stablished and conventional intervention in which it builds on to—Sleeve Gastrectomy—is currently the leading weight loss intervention in the United States despite its association with gastroesophageal reflux disease.
The weight loss curve recorded was similar between the two groups. The nadir of weight loss in both groups occurred at 1 year postoperatively. The median BMI at 1 year was 26 in both groups, with an average loss of 14 BMI points. However, significant weight loss was already observed in both groups in just 1 month postoperatively. In the long term, both groups presented sustained significant weight loss, and there was no significant difference between the two groups. The final median BMI in both groups was 29.
In general, the average weight loss recorded in both groups after 60 months was 9 BMI points. This result is in line with other studies conducted in different parts of the world, which report predicted values of 6.8 and 8.2 BMI points for the groups submitted, respectively, to Sleeve Gastrectomy and BGYR and with a follow-up of 5 years or more. 15
Our data reveal considerable advantages for the novel weight loss technique of SGJIB as compared with the gold standard of RYGB. However, there are limitations that should be addressed. One, the study is of observational nature. Thus, the analysis is subject to multiple bias related to study design. In addition, subjects were not recruited to treatment arms in a randomized fashion. Thus, the analysis is subject to selection bias and systematic error. Randomized clinical trials are required to better understand the long-term safety and efficacy of this novel intervention.
Conclusion
SGJIB is a promising surgical intervention for weight loss, being associated with at least similar weight loss as RYGB, with less severe postoperative complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was self-funded.