
Abstract
Objective:
Compare the clinical efficacy of anterior and posterior Calot's triangle approach in laparoscopic cholecystectomy (LC) for chronic atrophic cholecystitis, to find out which approach is much safer and more reliable.
Patients and Methods:
From June 2020 to June 2022, 102 patients with chronic atrophic cholecystitis underwent LC in our hospital. They were divided into anterior Calot's triangle approach group and posterior Calot's triangle approach group. In addition, their clinical data, intraoperative conditions, surgical results, and postoperative recovery were analyzed.
Results:
LC was performed in 41 females and 28 males by the anterior Calot's triangle approach, and in 20 females and 13 males by the posterior Calot's triangle approach. There were no differences in age, gender, and body mass index between the two groups (P > .05). The probability of rupture of cystic artery between both groups was not significantly different (P = .549), and the intraoperative blood loss was more in the anterior group (P = .014). The operative time of the posterior approach appeared to be shorter (P = .013). Bile duct injury and conversion to open cholecystectomy revealed no significant difference (P > .05). The recovery time of gastrointestinal function, wound infection, white blood cell count, liver function, and postoperative hospital stay time were found to be not significantly different (P > .05).
Conclusion:
By the posterior Calot's triangle approach, LC is a convenient and feasible surgical procedure for chronic atrophic cholecystitis with less blood loss and can become easier without increasing the risk of surgery.
Background
Gallstones, as one of the most common biliary diseases, can cause significant morbidity with a prevalence of 20%–40% in European populations. 1 Postmortem studies have found gallstones in 12% of men and 24% of women of all ages. 2 Some patients are diagnosed with gallstones by accident and have no symptoms. Around 45.7% of the patients came to the clinic with chronic cholecystitis and 32.9% with acute cholecystitis. 3 More than 90% of chronic cholecystitis is associated with the presence of gallstones; due to extensive fibrosis, the gallbladder may appear shrunken.4,5 Some patients with chronic atrophic cholecystitis even have no obvious symptoms, and once the atrophy of gallbladder occurs, the gallbladder cancer rate will become higher. As we know, the most common surgical treatment of gallstones complicated with cholecystitis is laparoscopic cholecystectomy (LC). 6
The incidence of iatrogenic bile duct injury (BDI) is low, but with the widespread use of LC, the rate of iatrogenic BDI has not decreased. 7 The reported rate of occurrence of BDI in LC is ∼0.5% to 0.85%. 8 Once BDI occurs, it will bring a heavy blow to both the patient and the surgeon, and even affects the patient's quality of life seriously.9,10
Anatomic variations of Calot's triangle are found to be closely associated with BDI during LC. 11 There are some important ducts in Calot's triangle, such as cystic artery, hepatic artery, accessory hepatic duct, and anatomical variations often occur here. Injuries often arise from the incorrect identification of the common bile duct (CBD) or dissecting too close to the CBD or common hepatic duct (CHD). 12 Once injuries occur, both the risk of surgical complications and the probability of conversion to open cholecystectomy (OC) will increase. 13 Therefore, during LC, especially for the chronic atrophic cholecystitis, the dissection of Calot's triangle is the key to the success of LC.
To reduce the risk of surgical injury during LC for patients with chronic atrophic cholecystitis, this article studies the dissection of Calot's triangle by different approaches when performing LC in such patients. Finally, we try to find out which approach is more advantageous, safer, and easier for LC.
Patients and Methods
This study involved patients who suffered from atrophic gallbladder, which was diagnosed with chronic inflammation by ultrasound before the operation and verified during the surgery. Also, the clinical data were collected from the Hepatobiliary Surgical Department of the First Affiliated Hospital of Chongqing Medical University, Chongqing, China. All patients signed the informed consent form for surgery and underwent LC in our hospital. Complete clinical data were recorded. All methods were carried out in accordance with the 1964 Declaration of Helsinki and later amendments.
Patients
Because of the atrophy of gallbladder and gallstones, which were shown by abdominal ultrasound before admission, all patients were admitted to the hospital without obvious abdominal pain, abdominal distention, and other discomfort, although some patients had previous episodes of abdominal pain. According to the ultrasound, the gallbladder of any patient was either reduced in size (<6 cm in length and <3 cm in width) or was not visible in the gallbladder fossa area, with only the strong echo of gallstones. Moreover, atrophy of gallbladder was observed during laparoscopic surgery in all enrolled patients. Before the operation, the operative strategy for every patient was to perform LC. The gallbladder of every patient was clearly found to be atrophic during the operation.
The preoperative liver functions of these patients were normal, and no other serious diseases were found. Their surgical records were detailed, and those who were not detailed and had a history of abdominal surgery were excluded. In addition, pregnant and lactating women were not included.
Methods
Operation
All patients were scheduled for LC and CO2 was used to establish pneumoperitoneum during the operation. Three-port procedure was the preferred method, if necessary, the four-port procedure was used. The subcostal incisions, varying from 6 to 10 cm in length, were used in the patients who were converted to OC. According to different ways of dissecting the tissue in Calot's triangle during LC, all patients were divided into two groups: the anterior Calot's triangle approach group (anterior group) and the posterior Calot's triangle approach group (posterior group). The posterior group is to dissect the posterior portion of Calot's triangle preferentially, while the anterior group is to dissect the anterior portion Calot's triangle preferentially (Figs. 1 and 2).
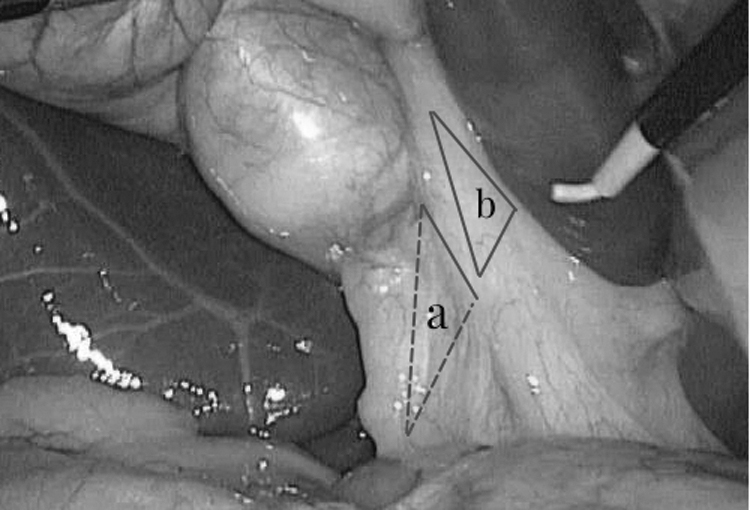
The anatomical position of the anterior and posterior Calot's triangle. Triangle a: the posterior portion of Calot's triangle, the posterior group preferentially dissected the posterior portion of Calot's triangle. Triangle b: the anterior portion of Calot's triangle, the anterior group preferentially dissected the anterior portion of Calot's triangle.
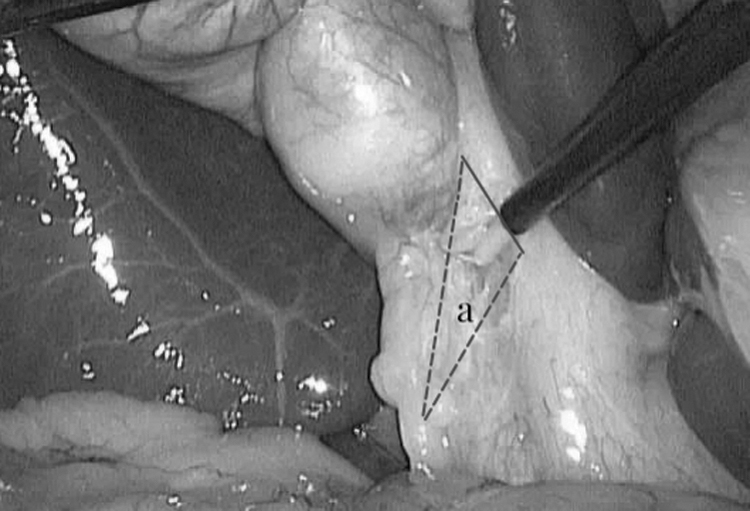
The anatomical position of the posterior Calot's triangle. Triangle a: the posterior portion of Calot's triangle, the posterior group preferentially dissected the posterior portion of Calot's triangle.
Because of the retrospective nature of the study, there was no use of preoperative randomization of patients into which approach. The basis for grouping was determined primarily by querying surgical records. According to the surgeon, their choices of approach were based on the adhesion and degree of clarity of the anatomical structure around Calot's triangle, and personal habits of surgery. Because it was a retrospective study, the results were inevitably influenced by confounding factors such as surgical skills, seniority, and personal habits of the surgeon. We decided to conduct further prospective, randomized, and controlled studies to determine which approach is better.
Analyses
Blood samples were collected on the day before and after operation. Serum was evaluated for white blood cell count (WBC), percentage of neutrophil (NEU%), and the liver function. The data from the operation were recorded and analyzed.
All analyses were performed using the software SPSS version 23.0 for Windows (IBM Corp., Armonk, NY.). The normality of the distribution of continuous variables was evaluated with the Kolmogorov–Smirnov test. All data in the descriptive statistics are given as mean with standard deviation for parametric data and in median with an interquartile range of 25%–75% for nonparametric data. For comparison, t-tests and the Mann–Whitney test were used for parametric and nonparametric data, respectively. Categorical variables are given as proportions and the Pearson chi-square and Fisher's exact tests were used for comparisons. P value < .05 was considered statistically significant.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by Ethics Committee of the First Affiliated Hospital of Chongqing Medical University in China on January 6, 2023, with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated deidentified data.
Results
Totally, 102 patients were enrolled in this study; the demographic and clinical characteristics are shown in Table 1. The ratio of female to male was 1.5. The age ranged from 20 to 79 years with a mean age of 49.4 ± 14.3 years. LC was carried out for 67.6% of patients by the anterior Calot's triangle approach and for 32.4% of patients by the posterior Calot's triangle approach. The body mass index of the patients was not significantly different. Liver function, WBC, and NEU% were normal before the surgery, and so, we did not analyze them.
Demographic and Clinical Characteristics of the Two Groups
BMI, body mass index; SD, standard deviation.
Some surgical information and complications occurring during the operation are shown in Table 2. In the anterior group, five cases (7.2%) were converted to OC. Among them, the reason of conversion was BDI in three patients. Two of these patients were minor biliary injuries, characterized by minor bile leakage in the gallbladder bed, which were successfully sutured during the operation. Based on Strasberg classification, 14 another patient was classified as type D. The type D case of whom the chief surgeon was a junior doctor who had worked for <5 years was diagnosed by the observation of a small amount of bile outflow near the CHD. Also, CBD repair was performed by another senior doctor for that patient during the operation.
Some Surgical Information and Complications During the Operation
BDI, bile duct injury; IQR, interquartile range; OC, open cholecystectomy; RCA, rupture of cystic artery.
The reason of conversion was rupture of cystic artery (RCA) in one patient with a variant of the cystic artery, which lay close to the cystic duct for a long distance and was ligated during OC. In addition, the causation of conversion was severe adhesion around Calot's triangle in other two cases. In addition, the other two patients with RCA were due to inadvertent injury of the cystic artery during dissection of Calot's triangle with the use of an electric hook, fortunately, the cystic artery was successfully ligated during LC. In the posterior group, one case (3.0%) was converted to OC because of severe adhesion and fibrosis in Calot's triangle.
Although there was no significant difference between the two groups in terms of RCA, BDI, and conversion to OC, operative time of the posterior group was significantly shorter than that of the posterior group (P = .013). LC performed from the posterior portion of Calot's triangle resulted in less blood loss than from the anterior portion of Calot's triangle (P = .014).
According to the Clavien–Dindo classification of postoperative complications, 15 no patient of this study had Grade IV and Grade V complications, and the classification of complications is shown in Table 3 in detail. Postoperative complications mainly included wound infection and postcholecystectomy bile leakage (PCBL), and were analyzed with some postoperative tests, shown in Table 4. Time to the first flatus (TFF), wound infection, PCBL, and length of hospital stays (LHS) were comparable in both groups. There was no significant difference between the TFF of the patients in the two groups (P = .172). In the anterior group, one patient who was converted to OC underwent wound infection after the surgery. There were two patients in the anterior group who suffered from PCBL, one was found by observing the color of abdominal drainage, and the other was diagnosed by ultrasonography because of persistent abdominal pain after operation.
The Postoperative Complications According to Clavien–Dindo Classification in the Two Groups
PCBL, postcholecystectomy bile leakage.
Some Postoperative Tests and Complications
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DB, direct bilirubin; γ-GT, gamma-glutamyl transpeptidase; NEU%, percentage of neutrophil; TB, total bilirubin; TFF, time to the first flatus; WBC, white blood cell count.
No wound infection and PCBL occurred in all patients in the posterior group. There was no significant difference in LHS, with a median of 2 days. On the first day after surgery, blood routine and liver function tests were performed in all patients. The laboratory tests used for analysis included WBC, NEU%, and the levels of total bilirubin (TB), direct bilirubin (DB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and gamma-glutamyl transpeptidase (γ-GT) in the serum (Table 4). WBC and NEU% were increased in all patients, but there was no significant difference between the two groups. The liver function of both groups was not significantly different, which indicated that the two approaches had similar effects on liver function (P > .05).
Discussion
LC is the gold standard operation for patients with gallstones and represents one of the most common routine interventions performed worldwide in both elective and emergency settings. 16 However, with the widespread of LC, the risk of BDI, a serious complication, is even higher than that of OC.17,18 One study found that 47% of surgeons had experienced BDI in their careers, and 17.1% had experienced BDI multiple times. 18 Because the morbidity and mortality associated with BDI are high, the quality of life and long-term survival of patients are decreased, and their forensic significance is also discussed. 19 We should not neglect the importance of surgical safety when performing LC. The factors related to the safety of LC include anatomy, pathology, wrong recognition of the ducts, and improper operation. 20
The most common site of injury is located near Calot's triangle, including the CHD, CBD, hepatic artery, cystic artery, accessory hepatic duct, and other important ducts. 21 A key critical view of safety (CVS) technology was proposed as early as 1995 as the safest way to ensure LC, emphasizing the anatomy of the surrounding tissues of gallbladder, particularly Calot's triangle, and is also a key step in reducing the risk of BDI during LC. 21 In 1891, Jean-François Calot thought the key to cholecystectomy was the anatomy of the extrahepatic duct system. He asserted that working in the region of the cystic duct is the more delicate part of the operation. 22 In patients with chronic cholecystitis and atrophic gallbladder, repeated inflammation of Calot's triangle can cause a series of pathological and physiological changes, which will lead to the critical area of scar formation and anatomical changes.23,24
At this point, bile ducts and arteries in Calot's triangle become difficult to dissect, and ultimately, the difficulty of LC and the risk of iatrogenic injury will increase.
With the wide application of LC, LC-related iatrogenic injury of Calot's triangle is not rare.25,26 Bleeding from the cystic artery is a very tricky complication in LC. Because of the cystic artery rupture, the entire critical vision of the operation and the exposure will be affected by the blood. In that case, the risk of conversion to OC and iatrogenic injury can increase. Agrusa et al. reported a 1.2% rate of conversion to OC due to arterial hemorrhage. 27 Kudurupaka reports that the incidence can be as high as 6.62%. 28 Cystic artery and right hepatic artery often occurred in Calot's triangle. Fateh et al. reported that 94.7% of cystic arteries were at a superomedial position to the cystic duct. 29
The region behind Calot's triangle is relatively more distant from cystic artery and right hepatic artery than the front. So, there is much more space to operate in the posterior portion, where the tissue is weaker than the anterior. If anatomical dissection starting from the posterior portion behind Calot's triangle is performed during LC, there will be a lower chance of injury to cystic artery and right hepatic artery than from the anterior. Of course, the risk of vascular injuries during LC would be lower if the variant of the cystic artery could be identified early, and according to Pesce et al., 30 there are currently four most common variants of cystic artery.
In this study, one patient from the anterior group had a type B variant of cystic artery which was a long artery originating from the junction of the cystic duct and CBD. During dissection of the cystic duct, the cystic artery was injured and stopping bleeding under laparoscopy was difficult. Due to the unclear vision of surgical field caused by hemorrhage, conversion to OC had to been carried out to ligate the ruptured cystic artery eventually. Other two patients in the anterior group suffered intraoperative bleeding from ruptured cystic arteries, due to the damage caused by electric hook during dissection of tissues with severe adhesion and fibrosis in Calot's triangle.
There was no significant difference between RCA in the two groups (P > .05). The amount of bleeding of the posterior group was significantly less than that of the anterior group (P < .05), which suggested that starting dissection from the posterior portion of Calot's triangle may reduce intraoperative bleeding in LC. Sapmaz and Karaca found that BDI, adhesion in Calot's triangle, and cystic duct injury accounted for 41.5% of the reasons for switching to open procedure. 31 Especially for chronic inflammation of the atrophic gallbladder, with the presence of changes of anatomical structure in Calot's triangle, iatrogenic injuries are more likely to occur. Kara and Kalayci reported that conversion to OC could be caused by fibrosis and adhesion of the tissue around Calot's triangle (27%), BDI (4.3%), and partial injury of the CHB (0.9%). 32
Nassar et al. analyzed 5738 cases of LC, of whom 0.49% (28/5738) underwent conversion to OC. Although the probability of transition is not very high, 32% (9/28) of patients converted to OC due to dense adhesion in Calot's triangle. 33 Therefore, careful dissecting of tissue around Calot's triangle can help to avoid conversion. In our study, the rate of conversion was comparable in both groups (7.2% versus 3.0%, P = .661). Variations in the cystic duct occur from time to time, and the doctors in the team occasionally encounter them during surgery. Fortunately, none of the cases in this study had a variant of the cystic duct. Also, there was no difference in BDI between the two groups. Performing LC via a posterior approach did not reduce the probability of conversion and BDI, neither did it increase the probability.
This also suggested that the posterior approach did not increase the risk of intraoperative complications compared with the anterior approach. The operative time in the posterior approach group was shorter than that in the anterior approach group, which indicated that the operation from the back of Calot's triangle might reduce the operative difficulty and shorten the operative time of LC. Therefore, the preferred approach for LC may be a safer and more convenient option.
Postcholecystectomy complications have always been the focus of LC. In a systematic review, Alexander et al. found that wound infection was reported in 118 studies (51%) and defined in 24 (10%), using 16 different definitions. 34 In our study, wound infection was defined as the presence of redness, exudation, and bacteria in the exudation of the wound after surgery. Also, wound infection was not significantly different with P > .05. Only one patient in the anterior group who converted to OC developed wound infection, probably due to the greater trauma of wound. Although LC has been the standard procedure for the treatment of gallbladder diseases, sometimes PCBL still occurs.
Nassar and Ng found that the incidence of PCBL can be as high as 0.4%, and they think that careful blunt dissection in the proper anatomical planes avoiding direct or thermal injury to subvesical and sectoral ducts and a policy of actively searching for hepatocystic ducts during gallbladder separation to identify and secure them can reduce bile leakage from such ducts. 35 The retro-triangular approach to the gallbladder is just a good option to avoid PCBL. In this study, PCBL occurred in two patients in the anterior group and none in the posterior group (P > .05). Both patients were diagnosed as bile leakage near the cystic duct by endoscopic retrograde cholangiopancreatography and were cured by biliary stent implantation.
After surgery, the body often has different degrees of inflammatory reaction to defend the host against invading pathogens and exogenous infections. A moderate inflammatory response helps the body fight off infection, while an excessive immune response can lead to organ damage. Surgical procedures can represent a potential trigger for systemic inflammation that causes the secretion of proinflammatory cytokines (interleukin-6, interleukin-8) and activation of neutrophils. 36 Therefore, we can detect the levels of the above inflammatory factors, WBC, or NEU% in serum to reflect the body's inflammatory response. There was no significant difference between WBC and NEU% (P > .05) in both anterior and posterior groups. This suggests that LC via the posterior approach does not elicit a stronger inflammatory response than the anterior approach.
Meanwhile, the levels of ALT, AST, TB, DB, ALP, and γ-GT of the two groups after LC were not significantly different, which indicated that the effects on liver function were equal. In other words, LC via posterior Calot's triangle approach does not increase the incidence of liver function damage.
The patient's postoperative recovery can reflect the impact of the operation in the end. We did not use postoperative pain as an outcome measure, since not all patients had chosen postoperative analgesia. At present, many methods can be used to reflect the recovery of gastrointestinal function after LC, such as the recovery time of bowel sounds, the first postoperative time of exhaust, and the first postoperative time of defecation. 37 We used the TFF after surgery to reflect the recovery of gastrointestinal function. The median time to anal exhaust was 23 hours in the anterior group and 22 hours in the posterior group (P > .05). This means that no matter which approach is used to perform LC, there is no difference in the effect of postoperative gastrointestinal function.
To sum up, there was no significant difference in postoperative recovery between the two groups, which also shows that carrying out LC by the posterior Calot's triangle approach is safe and feasible.
Limitations
As a retrospective study, this study has its limitations. Data of this study were obtained from a single institution and not a double-blind trial. Because of the retrospective nature of the analysis, the surgeon's criteria for choosing an approach are not well clearly, which may affect the results of the study. Moreover, the surgeons who perform these operations are not the same person, and so, it was difficult to rule out the influence of different doctors on the surgical results. For the short follow-up time, no comparison of follow-up was made. A small sample size also is a limitation of this study. Because of the limited number of cases and the nonrandomized control study, a propensity score-matched analysis was not done.
The surgical procedure in this research may not be representative of the average level of surgical practice. The clinical results of this study cannot be evaluated with the small sample size.
Conclusion
LC is a safe and an effective treatment for chronic atrophic cholecystitis. Dissection of Calot's triangle is particularly important, and it is safer and equally effective to perform LC through the posterior approach than through the anterior approach. Less operation time and less blood loss appear to be the major advantages of the posterior approach. However, some prospective studies with larger sample sizes are needed to substantiate these results.
Footnotes
Acknowledgment
The authors sincerely thank Dr. Yong Chen, Professor in the Department of Hepatobiliary Surgery, The First Affiliated Hospital of Chongqing Medical University, for his valuable suggestions in preparing the article.
Authors' Contributions
H.Z. collected part of the data and wrote the main body of the article, S.L. collected part of the data, and X.W. and F.L. provided advice on medical aspects.
Disclosure Statement
H.Z., S.L., X.W., and F.L. have no conflict of interest to disclose.
Funding Information
No funding was received for this article.