
Abstract
Introduction:
The overexpression of proinflammatory cytokines in obesity has suggested an association between obesity and inflammation. In this study, we aimed to predict the success of weight loss at the end of the first year of patients who underwent laparoscopic sleeve gastrectomy (LSG) for morbid obesity using hemoglobin, albumin, lymphocyte, and platelet (HALP) score and modified HALP (m-HALP) score.
Materials and Methods:
Patients were divided into two groups according to the success of weight loss. The groups were compared in terms of HALP score, m-HALP score, demographic parameters, and preoperative laboratory tests. The diagnostic performance measurements of the m-HALP score were calculated. In addition, logistic regression analysis was performed for the factors affecting weight loss in the first year after LSG.
Results:
Seventy-two patients were evaluated. The median m-HALP score of the patients with an excess weight loss percentage (EWL%) <60 threshold was 562 (416.6–891.9), the median m-HALP score of the patients with an EWL% above the 60 threshold was 394.3 (347.9–543), and the difference between the outcome groups was significant (P = .002).The accuracy of m-HALP score in identifying the patients whose EWL would be <60% 1 year after the surgery was 63.9 (95% confidence interval = 51.7–74.9).
Conclusion:
This study showed that the m-HALP score is effective in predicting weight loss after bariatric surgery.
Introduction
According to recent studies, obesity is a severe public health issue that is becoming more prevalent in both adult and pediatric populations. Obesity is a serious disease on its own, and it paves the way for many important health problems. Bariatric surgery has been shown to be effective in achieving both sustainable weight loss and improving obesity-related comorbidities. Bariatric surgery continues to be the only effective and sustainable treatment method in individuals with a body mass index (BMI) of 35 and above. Today, there are many bariatric surgical procedures, but laparoscopic sleeve gastrectomy (LSG) is one of the most applied procedures. 1
Achieving sustainable weight loss after bariatric surgery depends not only on the surgery but also on the patient. It is known that the patient's healthy eating habits and regular physical activity affect as much as the impact of surgical technique in achieving sustainable weight loss.2–5
The overexpression of proinflammatory cytokines in obesity suggests that there is an association between obesity and inflammation. With obesity, adipose tissue increases, and hypoxia occurs as a result of insufficient blood flow to feed the accumulating adipose tissue. The resulting hypoxia causes inflammation by overexpressing proinflammatory cytokines and increasing macrophages in the tissue. 6 It has been asserted that obesity is associated with an increased degree of this inflammation. Weight loss induced by surgery or alternative methods leads to decreased expression of proinflammatory markers in both adipose tissue and plasma of obese individuals and a decrease in the number of macrophages in adipose tissue. 7
The hemoglobin, albumin, lymphocyte, and platelet (HALP) score has been demonstrated to be a predictive indication in a variety of malignancies. It is used as a marker of inflammation and is especially useful for geriatric patients. 8 It was subsequently asserted that low platelet value is a more noteworthy indication of inflammation and mortality than high platelet value, leading to the development of the modified HALP (m-HALP) score. 9
In this study, we aimed to predict the success of weight loss at the end of the first year of patients who underwent LSG for morbid obesity using HALP score and m-HALP score.
Materials and Methods
Patients who underwent sleeve gastrectomy owing to morbid obesity in the department of general surgery in University of Health Sciences, Ümraniye Training and Research Hospital between January 2021 and May 2022 were analyzed retrospectively. Patients with a BMI of 35 or above and who were approved for surgery by preoperative multidisciplinary council evaluation were included in the study. Other nonoperative treatment methods (dietary regulation and medical treatment) were applied to all patients for at least 6 months before surgery. Patients who underwent other bariatric surgical procedures other than LSG and who lacked data were excluded from the study. This study was approved by the Umraniye Training and Research Hospital Ethics Committee (May 15, 2023-215590918).
The data on preoperative and postoperative first year weight, BMI, and excess weight loss (EWL) percentage were recorded, along with demographic information including the patients' age and gender. Leukocyte (WBC), hemoglobin (HGB), platelet (PLT), lymphocyte (LY), monocytes, neutrophil (NE), glucose, platelet–lymphocyte ratio (PLR), neutrophils–lymphocyte ratio (NLR), albumin (ALB), alanine aminotransferase (ALT), and aspartate aminotransferase (AST) values were recorded at the patient's application for surgical preparation.
The HALP score was calculated using the formula hemoglobin (g/L) × albumin (g/L) × lymphocyte (/L)/platelet (/L), whereas m-HALP was calculated using the formula; hemoglobin (g/L) × albumin (g/L) × lymphocyte (/L) × platelet (/L). 9
BMI was calculated using the formula body weight (kg)/height (m2). The ideal weight of the patients was calculated as 25 × height (m2), so that the ideal BMI was 25 kg/m2. EWL% value was calculated using the formula; initial weight (kg)—first year weight (kg)/initial weight (kg)—ideal weight × 100. 10
The receiver operating characteristic (ROC) curve analysis was performed and the cutoff value was determined for the m-HALP scores of the patients. According to this value, patients were divided into two groups as high- and low-scoring group. The same grouping could not be performed for HALP score because of insignificant ROC curve distribution. The fact that the EWL value was >60% at the end of the first year was considered as success.10,11
The groups were compared in terms of HALP score, m-HALP score, demographic parameters, preoperative laboratory tests. The diagnostic performance measurements of the m-HALP score were calculated. In addition, logistic regression analysis was performed for the factors affecting weight loss in the first year after LSG.
In this study, the primary outcome was to evaluate the effect of m-HALP score on predicting successful weight loss after LSG. The second outcome was to determine the parameters that affect successful weight loss at the end of the first year of the LSG operation.
Statistical analysis
We used SPSS 29 for the statistical analysis of the data. The normality of the continuous data was tested using Shapiro–Wilk. Continuous data with a normal distribution were presented as mean (±standard deviation), and group comparisons were performed using the Student's t-test. Continuous data that did not follow a normal distribution were presented as median (25th to 75th quartiles), and group comparisons were made using the Mann–Whitney U-test. Categorical data were presented as frequency (%) and group comparisons were conducted using the chi-square test. For the assessment of diagnostic performance, ROC was used. The optimal cutoff points were determined by the Youden's index. For multivariable analysis, binary logistics was used. Multicollinearity was checked and the variables demonstrating high correlation were excluded from the model. The goodness of fit was tested using Hosmer and Lemeshow test. The level of significance was set to P < .05.
Results
Of the 129 patients who fulfilled the inclusion criteria, 57 were excluded because of various reasons, resulting in a total of 72 patients included in the final analysis. Patient flow chart is given in Figure 1.

Flow chart.
The patients had a median age of 34 (27–46) years, with 58 patients (80.6%) being women. The median BMI before the surgery was 44.4 kg/m2 (42.5–48), and 1 year after the surgery the median BMI decreased to 26.8 (23.9–32.4). The median EWL% was 91.2% (62.9%–104.8%) at the end of first year. There were 18 (25%) patients whose EWL% was below the 60% threshold first year after the surgery. Basic characteristics, preoperative laboratory results, and univariable analysis of the variables are given in Table 1.
Basic Characteristics, Preoperative Laboratory Results and Univariable Analysis of the Variables Between the Outcome Groups
The bold p values are statistically significant.
BMI, body mass index, EWL: Excess weight loss, NLR, neutrophil–lymphocyte ratio; PLR, platelet–lymphocyte ratio; SD, standard deviation.
Primary outcome measures
The median HALP score of the patients with an EWL% below the 60 threshold was 5.4 (4.5–6.6), median HALP score of the patients with an EWL% above the 60 threshold was 5.7 (3.9–6.9), and the difference between the outcome groups was not statistically significant (P = .835).
The median m-HALP score of the patients with an EWL% below the 60 threshold was 562 (416.6–891.9), median m-HALP score of the patients with an EWL% above the 60 threshold was 394.3 (347.9–543), and the difference between the outcome groups was significant (P = .002; Table 2).
Effect of Hemoglobin, Albumin, Lymphocyte, and Platelet Score and Modified Hemoglobin, Albumin, Lymphocyte, and Platelet Score on Weight Loss
The bold p values are statistically significant.
EWL, excess weight loss; HALP, hemoglobin, albumin, lymphocyte, and platelet; m-HALP, modified HALP.
The area under the curve (AUC) of the m-HALP score was calculated as 0.744 (95% confidence interval [CI] = 0.612–0.875; Fig. 2). Setting the cutoff value to the optimal point, which is m-HALP = 400, the sensitivity of the m-HALP score in identifying the patients whose EWL would be <60% 1 year after the surgery was 94.4% (95% CI = 72.7%–99.8%), specificity was 53.7% (95% CI = 39.6%–67.4%), positive likelihood ratio was 2.04 (95% CI = 1.5–2.78), negative likelihood ratio was 0.1 (95% CI = 0.001–0.68), and accuracy was 63.9 (95% CI = 51.7–74.9). Measures of diagnostic performance of the m-HALP score are given in Table 3.
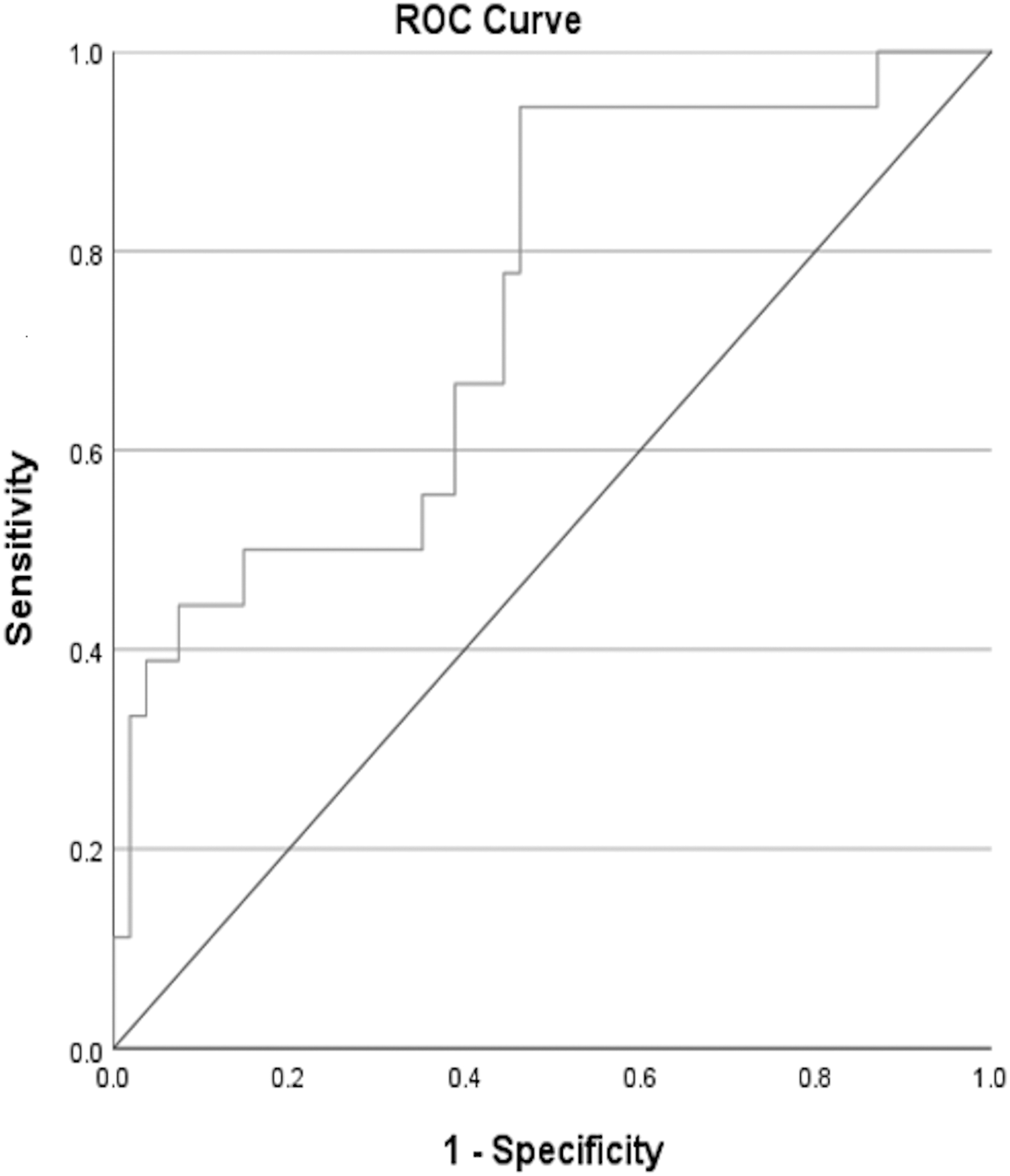
The receiver operating characteristics curve of the m-HALP score in identifying the patients whose EWL would be <60% 1 year after the surgery. EWL, excess weight loss; m-HALP, modified hemoglobin, albumin, lymphocyte, and platelet.
Diagnostic Performance Measures of the Modified Hemoglobin, Albumin, Lymphocyte, and Platelet Score in Identifying the Patients Whose Excess Weight Loss Would be Below 60% 1 Year After the Surgery
Values in parentheses indicate 95% CI.
For the logistic regression analysis, we dichotomized the m-HALP score from the optimal cutoff value (m-HALP = 400). Lymphocyte and neutrophil–lymphocyte ratio variables were excluded from the model owing to multicollinearity. For the final model, age, m-HALP score, and preoperative BMI variables were chosen. The assumption of goodness of fit was met (Hosmer and Lemeshow P = .976). The model was able to explain 57.4% of all the variance (Nagelkerke R2 = 0.574) and was able to identify 86.1% of all the patients correctly. Preoperative BMI, m-HALP score, and age were found to be independent predictors of unsuccessful procedure. The most valuable predictor was found to be preoperative BMI (Wald statistics = 9.385; Table 4).
Logistic Regression of the Potential Predictors of Unsuccessful Population
BMI, body mass index; m-HALP, modified hemoglobin, albumin, lymphocyte, and platelet.
Discussion
We did not find any significant difference between the outcome groups in terms of HALP score. But patients who had >60% EWL 1 year after the surgery, had significantly lower m-HALP scores in their preoperative laboratory test. Moreover, m-HALP score showed moderate performance in identifying patients whose EWL would be <60% 1 year after the surgery. Also, m-HALP had very high sensitivity and very low negative likelihood ratio at its optimal cutoff value (m-HALP = 400), indicating that m-HALP can be used as a screening tool before surgery to detect patients who are not going to benefit the procedure optimally. In addition, the m-HALP score was found to be an independent predictor of unsuccessful procedure among preoperative BMI and age, being the second most valuable predictor. This finding implies that the m-HALP score could potentially hold substantial importance in future prediction score modeling studies. In the group of successful patients with EWL% >60% at postoperative first year after LSG, lymphocyte, mean age, platelet, and m-HALP score levels were found lower and NLR level was found higher.
The HALP score, which was used for the first time to predict the prognosis in gastric cancer, has subsequently been used in many malignancies such as renal cell cancer and colorectal cancer.12–14 Hemoglobin and albumin were used to assess the nutritional status, whereas lymphocytes and platelets were utilized to assess the immune function in the HALP score.
The first two parameters of the m-HALP score, hemoglobin and albumin, reveal nutritional status. The main protein in plasma is albumin, which is sometimes referred to as a negative acute phase reactant. Because both these groups included people with adequate nutritional status, there was no significant difference between them for these parameters in our study between the low BMI and high BMI groups. A proportional change between BMI and the levels of lymphocytes and platelets was discovered in a study that evaluated the effects of obesity on biochemical parameters in the literature.15,16 In our research, we revealed that patients with low platelets, lymphocyte, and BMI values lost weight more effectively.
Ferhat et al. in their study on the efficacy of HALP score to predict weight loss success in the first year after surgery in patients undergoing LSG found that patients with a high HALP score lost weight more effectively. Furthermore, they did not encounter a significant change in the NLR value although they discovered a large decline in the PLR value in the group of patients with a low HALP score. 17 In our research, we discovered that the HALP score was ineffectual at predicting patients' success in losing weight in the first year after surgery; however, the lower m-HALP score was substantially associated with improved weight loss in the first year after LSG. In addition, there was no association in our study between the patients' preoperative PLR values and the weight loss observed in the first year after surgery; however, the preoperative NLR value was shown to be considerably higher in the patient group with EWL >60%.
Guerreiro et al. showed that younger patients had considerably better long-term weight loss success when they looked at the effects of gender and age of patients on metabolic syndrome remission after surgery. 18 Similarly, Sisik et al. discovered that younger age and lower BMI values were positively associated with better EWL% values in preoperative evaluation. 19 In our study, we also revealed that the average age of patients with EWL >60% was statistically significantly younger in the first year after surgery.
No study in the literature has examined the relationship between m-HALP score and weight loss after LSG. Salih et al. in their study aimed at estimating the mortality of patients with an m-HALP score in elderly patients with acute heart failure. They found that the mortality of patients with a low m-HALP score is higher and emphasized that this condition is especially associated with low platelet count. 9
In our study, we revealed that the patient group with low platelet count and, consequently, low m-HALP score reached significantly better weight loss at the end of the first year. It is necessary to explain the discrepancy in platelet values between our study and this study. The situation may be explained by the fact that the average platelet value of the patient group in the reference article with the high platelet value and low mortality is even lower than the average platelet value in the patient group in our study with the low platelet value and more successful weight loss. The preoperative low lymphocyte values, one of the parameters of the m-HALP score that we used in our study, can be explained by the formation of less inflammation, resulting in better weight loss, but no studies evaluating the relationship of a lower preoperative platelet value with better weight loss have been found. In this aspect, our study is important in terms of shedding light on the research of this issue.
It is critical to identify the contributing factors and address them before surgery for patients who have high lymphocyte, high platelet, and indirectly high m-HALP score values during the preoperative period. In this context, designing prospective studies focusing on patients with high inflammatory parameters during the preoperative period will be a better guide in demonstrating the predictive usefulness of these inflammatory parameters and m-HALP scoring.
Limitations
This study also includes some limitations. The fact that the study design is retrospective and evaluates only the weight loss of patients at the end of the first year is the most conspicuous limitations. In addition, because hemoglobin and albumin values, which are the parameters of the m-HALP scoring used in the study, are directly related to the nutritional status, the use of this scoring to evaluate weight loss in bariatric surgery may be considered controversial.
Conclusion
Predicting the success of weight loss after bariatric surgery is an important step and will be a guide in determining the patient population in which surgery will show positive results. this study showed that the m-HALP score is effective in predicting weight loss after bariatric surgery. New studies with large populations are needed as there are not enough studies in the literature to prove this.
Young age, low lymphocyte count, low platelet count, low m-HALP level, and a high NLR level stand out as crucial indicators of successful weight loss.
Footnotes
Acknowledgment
The authors thank Mehmeh Muzaffer Islam for the assistance of biostatistics.
Authors' Contributions
Research concept and design, M.T.D. and A.Ş.; Collection and/or assembly of data, M.T.D.; Data analysis and interpretation, M.T.D.; Writing the article, M.T.D. and A.Ş.; Critical revision of the article, M.T.D. and A.Ş.; Final approval of article, M.T.D. and A.Ş.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.