
Abstract
Introduction:
The pediatric choledochal cyst with hepatic duct stenosis occurs postoperative hepatolithiasis, recurrent cholangitis, or pancreatitis. The laparoscopic hepatic ductoplasty can prevent these incidences.
Objectives:
To determine the characteristic of hepatic duct stenosis, laparoscopic treatment, and outcomes in systematic review and meta-analysis.
Methodology:
We searched the published studies on PubMed, Scopus, and Cochrane Library databases from January 1985 to April 2022 in English language. This protocol was registered to PROSPERO (CRD42022332145).
Results:
Nine published studies and 412 patients were included. The meta-analysis revealed that the locations were the confluence of the left and right hepatic ducts 43.1%, the left or/and the right hepatic duct 8.3%, and the unclassified location 60.4%. These characteristics included a membranous/septum appearance (44.7%) and a circumferential/relative stenosis (22.7%). The laparoscopic techniques were the wide hilar Roux-en-Y hepaticojejunostomy (28.5%), the excision of membranes/septum (26.5%), and the mixed hepatic ductoplasty (45.0%). The outcomes revealed a minor bile leakage of 3.8% and minimal bleeding. The meta-analysis showed no statistical difference between laparoscopic and open techniques in hepatolithiasis (0% versus 2.00%), anastomosis stricture (4.83% versus 10.00%), and no recurrent cholangitis. There was no conversion rate but showed a trend the prolonged operating time in laparoscopy.
Conclusion:
Laparoscopic hepatic ductoplasty is safe and effective. The characteristics and location can be feasible laparoscopic procedures. So, hepatic ductoplasty decreases hepatolithiasis, anastomosis stricture, or recurrent cholangitis and may increase minor bile leakage. The systematic review registration was PROSPERO system with CRD42022332145.
Introduction
The pediatric choledochal cyst develops postoperative hepatolithiasis and complications such as anastomosis stricture, cholangitis, and pancreatitis.1–3 Their etiology is the coincidence of hepatic duct stenosis.2–5 The previous report demonstrated not only extrahepatic duct dilatation but also intrahepatic bile duct involvement, such as hepatic duct stenosis.1,6,7 Hepatic ductoplasty during complete excision of pediatric choledochal cyst and Roux-en-Y hepaticojejunostomy reconstruction can prevent these long-term complications 6 rather than standard Roux-en-Y hepaticojejunostomy. 8
According to the classification of hepatic stenosis, there are two types depending on characteristics: web/membranous or septum appearance and circumferential/relative stenosis. 5
Therefore, several techniques depend on the site and characteristics, such as widening the stenotic part by hepatic duct excision, web excision, or hilar aggressive hepatic ductoplasty (combined method) for increased lumen diameter and bile flow.1,2,5,7
In the laparoscopic era, hepatic ductoplasty was developed during the definite operation of the choledochal cyst with several techniques, 8 but there was no role or feasibility indication, and their outcomes were still controversial. So, our objectives are to determine the characteristic of hepatic duct stenosis, laparoscopic feasibility, treatment, and outcomes in a systematic review and meta-analysis.
Materials and Methods
The electronic searching method was conducted according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines through the following databases: PubMed, Scopus, Cochrane Library database, Web of Science, and Google Scholar. Medical subject heading terms and keywords were searched in the titles and abstracts in English language with the combination of “choledochal cyst” OR “congenital bile duct dilatation,” AND “hepatic duct stenosis” OR “ bile duct stenosis” OR “Hepatolithiasis” AND “laparoscopy.”
The search method was restricted by age <18 years from January 1975 to April 2022. The relevant studies were searched by hand for additional reports and suggested by the journal publishers. The abstracts and full-text studies were reviewed to evaluate the eligibility criteria.
Screening of the published studies for inclusion and exclusion was followed by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) methodology (Fig. 1). All reviewers (J.N., J.A., and S.C.) screened the titles and abstracts with the decision to be reviewed through using Rayyan (www.rayyan.ai). The eligibility criteria were all cases of pediatric choledochal cyst with the coincidence of hepatic duct stenosis, the laparoscopic techniques or the comparison technique between laparoscopy or open approach, and their short-term or long-term outcomes such as operating time, length of stay (LOS), blood loss, bile leakage, conversion, anastomosis stricture, anastomosis leakage, hepatolithiasis, and recurrent cholangitis.

PRISMA flow diagram of systematic review of literature. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
The risk of bias and quality of evidence were determined by 3 reviewers independently using the Risk Of Bias In Non-randomized studies-of Intervention (ROBINS-I tool) for cohort study and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system. The level of evidence was classified according to Oxford Center for Evidence-Based Medicine (OCEBM) guidelines.
Statistical analyses were determined using categorical data using the number, percentage, and odd ratio (OR). The mean, median, interquartile range, standard deviation, and mean difference (MD) for continuous data were analyzed at a P value <.05. The eligible studies' heterogeneity was assessed using the chi-square test with a significant P value of <.1 and I2 < 40%. The Review Manager version 5.4.1 was used for meta-analysis. This study was begun after the protocol was registered and approved by the international prospective register of systematic reviews: PROSPERO (CRD42022332145).
Results
Nine studies were included after searching from electronic databases and using the eligibility criteria among 412 patients with pediatric choledochal cysts included in this study. These studies were six case series studies and three retrospective studies (Table 1). Only five studies reported the incidence of hepatic duct stenosis in pediatric choledochal cysts with 48.0% (range 22.9%–62.5%) (Fig. 2).
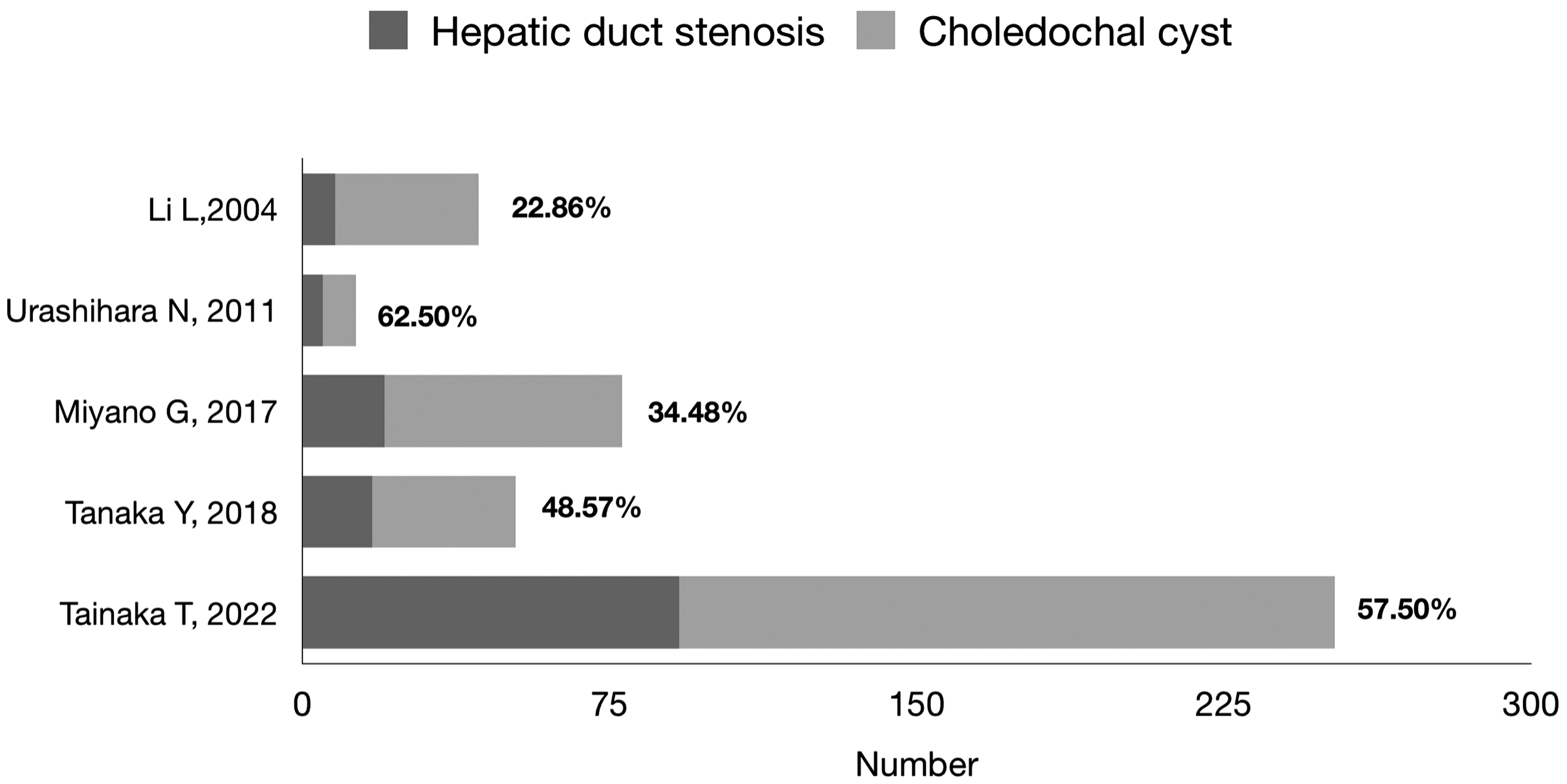
The cumulative incidence of hepatic duct stenosis in pediatric choledochal cyst.
Characteristic of Eligibility Study
ROBINS-I tool, Risk Of Bias In Non-randomized Studies of Intervention.
GRADE, Grading of Recommendations Assessment, Development, and Evaluation; IQR, interquartile range; LOS, length of stay.
According to the classified location and characteristics, 8 there were 282 sites of hepatic duct stenoses. The cumulative incidence of characteristics revealed the circumferential type at 44.7% (126 sites), the septum/membranous type at 22.7% (64 sites), and the unclassified type at 32.6% (92 sites). All characteristics of hepatic duct stenosis were identified during intraoperation with a meticulous probe or instrument to describe the features and locations. The most common location was the hilar hepatic duct, 28.0% with 53 sites of the total location 189 sites (33 sites of extrahepatic duct and 20 sites of hilar hepatic duct). The other locations were bilateral hepatic duct in 20 sites (10.6%), the right hepatic duct in 5 sites (2.6%), the left hepatic duct in 9 sites (4.8%), and unclassified locations in 102 sites (54.0%) of the total location 189 sites.
The feasible laparoscopic technique depends on the finding and location. For circumferential/relative hepatic stenosis (Fig. 3), widening the diameter of the hepatic duct before anastomosis is the concept of this technique. So, there were 2 types of operation in 69 sites (28.5%) (lateral side incision 71.1% [49 sites] and vertical incision 28.9% [only 20 sites of extrahepatic duct stenosis]). For the septum/membranous type, the operating technique was excision of the hepatic wall of the septum or membrane to release obstruction in 64 sites (26.5%) and anastomosis of hepatic duct mucosa transversely (Fig. 4).

The hepatic duct stenosis—circumferential/relative stenosis.

The hepatic duct stenosis—membranous/septum appearance.
The other technique was the hilar hepatic ductoplasty, which combined the excised septum or membrane and the widening of circumferential hepatic stenosis in 109 sites (45.0%), depending on the preoperative and intraoperative findings. Therefore, the laparoscopic technique was indicated by the characteristics, location, and surgeon preference.
The overall outcome of laparoscopic hepatic ductoplasty was reviewed in short-term and long-term outcomes depending on the operative techniques. For the short-term outcome, the operative time was 315–517 minutes (three studies) and LOS was 10–12 days (two studies). The bile leakage was eight sites (overall cumulative incidence of 3.2% and range of 3.8%–33.3% from all included studies). All laparoscopic hepatic ductoplasty had no conversion.
The subgroup analysis for meta-analysis comparing laparoscopy and open technique in hepatic ductoplasty in operating time and blood loss revealed statistical significance in prolonged operative time (MD: 123.00, 95% confidence interval [CI]: 92.35 to 152.65, and P value <.001) and lower blood loss (MD: −62.00, 95% CI: −83.3 to −40.17, and P value <.001) in the laparoscopic group (Fig. 5A, B). In the long-term outcome, the follow-up period was 0.25–9.3 years.

The meta-analysis between laparoscopic and open hepatic ductoplasty.
It is still the short follow-up period studies. There were hepatolithiasis, anastomosis stricture, and recurrent cholangitis. The cumulative incidence was two sites (2.9%) in hepatolithiasis, seven sites (10.1%) in anastomosis stricture, and no recurrent cholangitis (seven studies) from this systematic review. The subgroup analysis for meta-analysis comparing laparoscopy and open technique in hepatic ductoplasty in hepatolithiasis and anastomosis stricture revealed no statistically significant difference (only 1 of 50 sites in open technique for hepatolithiasis with OR: 0.25, 95% CI: 0.01 to 0.632, P value .40, and 3 of 62 sites in laparoscopic group versus 5 of 50 sites in open group with OR: 0.63, 95% CI: 0.06 to 6.15, P value .069) (Fig. 5C, D).
Discussion
Hepatic duct stenosis is the coincidence with pediatric choledochal cysts 22.9%–62.5%, increasing this coincidence in Asia.7,13,15–20 Preoperative imaging is necessary for detecting hepatic duct stenosis, especially choledochal cyst type IVa of Todani's classification. Ultrasonography, computed tomography, magnetic resonance cholangiopancreatocography, endoscopic cholangiopancreatocography, or intraoperative cholangiography is the preferred imaging to detect these lesions depending on the guidelines in each institute. However, the important point is the intraoperative evaluation of the hepatic duct stenosis during definite surgery.
The laparoscopic procedure has a magnified view that can identify the characteristic and the location near the bifurcation of the hepatic duct or segmental hepatic duct, which is proximal to the hepatic hilar. Meticulous probing into the hepatic duct lumen can be classified as a septum/membranous appearance or circumferential/relative stenosis, which indicates the feasibility of the hepatic ductoplasty technique. Otherwise, the probing technique could determine whether the downstream bile flow was caused by stenosis and characteristics together.
In our systematic review, all laparoscopic hepatic ductoplasty techniques can be performed as an open technique without conversion. This feasibility of laparoscopic hepatic ductoplasty during the definite operation can be classified as dependent on the characteristic of hepatic duct stenosis—widening the anastomosis, excised septum/membrane, or mixed technique. For the widening of the stenosis, the procedure depends on the surgeon's preference for vertical or lateral incision of the hepatic duct wall.
The important point is widening anastomosis without injury to the hepatic duct's vascular supply, which is close to the incision site. Our result showed that the septum/membranous type only excised the septum or membranous type before anastomosis. Still, some literature showed the combined laparoscopic technique (hilar aggressive hepatic ductoplasty) if they found the combined lesions.13,15
Therefore, the short-term and long-term outcomes after laparoscopic hepatic ductoplasty revealed a bile leakage rate of 3.8%–33.3%, which had a higher cumulative incidence than the open hepatic ductoplasty (0%–1.38%)1,14 and prolonged operative time because it is reflecting from the difficult technique, wide anastomosis, and the surgeon experiences, but there was the minimal bleeding in a laparoscopic procedure.
For the long-term outcome, the literature review found that the cumulative incidence of hepatolithiasis and anastomosis stricture was 2.6%–33.3% and 5.8%–10.0%.1,3,9,11–15,21,22 The literature review showed the higher incidence of hepatolithiasis in standard Roux-en-Y hepaticojejunostomy (23.85%) when compared with hepatic ductoplasty (3.83%) without difference in anastomotic stricture or leakage. 8
Our result was a decreased trend of hepatolithiasis (2.9%) and anastomosis stricture (10.1%) because the laparoscopic hepatic ductoplasty had the magnified view and meticulous procedure to identify the stenotic part and performed the anastomosis. For hepatolithiasis prevention, all laparoscopic techniques had lower cumulative incidence because of wide biliary-enteric anastomosis, and releasing septum/membrane can increase the bile flow. Otherwise, hepatolithiasis removal through the hepatic duct during the definite operation as much as possible can be helpful for prevention.
However, all laparoscopic procedures have limitations in the proximal segmental hepatic duct. This is the initial meta-analysis of the comparison between the open and laparoscopic hepatic ductoplasty, which found the trend of prolonged operative time and decreased bleeding but no statistical significance in hepatolithiasis and anastomosis stricture.
This study had many limitations. The first, our study was the systemic review of the case series and retrospective studies, which had a variety of outcomes and were difficult for comparison or meta-analysis. Second, the long-term development of hepatolithiasis and anastomosis stricture needs long observation periods, but our systematic review had a short observation period. So, the hepatolithiasis reflected from bile stasis may correlate with the anastomosis stricture, which caused biliary stenosis and calculus formation. The long-term observation should be an advocate for surveillance. Therefore, it is challenging to evaluate hepatolithiasis and anastomosis stricture.
Conclusion
Laparoscopic hepatic ductoplasty is safe and effective. The characteristics and location can be feasible in all laparoscopic hepatic ductoplasty in pediatric choledochal cysts. So, hepatic ductoplasty decreases hepatolithiasis, anastomosis stricture, or recurrent cholangitis, and may increase minor bile leakage.
Footnotes
Acknowledgment
The authors thank Prof. Hiroo Uchida, Nagoya University Hospital, Nagoya, Japan, for the inspiration in advance laparoscopic technique for choledochal cyst.
Authors' Contributions
J.N. contributed to conceptualization, methodology, investigation, software, resource, formal analysis, data curation, writing—original draft, visualization, supervision, and project administration. J.A. was involved in investigation and formal analysis. C.K. carried out investigation and formal analysis. S.C. oversaw formal analysis and writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.