
Abstract
Aim:
To evaluate the oncological and functional outcomes of 167 patients who underwent laparoscopic radical prostatectomy (LRP).
Materials and Methods:
The retrospective study included 167 patients who were treated with LRP due to clinically localized prostate cancer between January 2007 and April 2012. Most of the patients were treated with the extraperitoneal approach. Preoperative evaluations included age, serum prostate-specific antigen (PSA) level, and biopsy Gleason score. Perioperative evaluations included duration of operative time and anastomosis time, blood loss (milliliter), and complications. Postoperative evaluations included length of hospital stay and catheterization time. Continence and erectile function were evaluated both pre- and postoperatively. The patients who used no pads or no more than one pad daily and the ones who had only a few urine leakages on effort or exertion were accepted as continent. Postoperative potency was defined as the ability to achieve sexual intercourse with or without the use of PDE-5 inhibitors.
Results:
Mean age and mean operative time were 62.4 ± 6.0 years and 220.5 ± 45.6 minutes, respectively. Mean anastomosis time was 35.6 ± 9.8 minutes. Mean serum PSA level and mean Gleason score were 17.5 ± 9.97 ng/mL and 6.16 ± 0.42, respectively. Pelvic lymphadenectomy was performed in 94 patients and nerve-sparing procedures in 61 patients. The pathological analysis revealed positive surgical margin in 35 patients (20.9%). Bilateral and unilateral nerve-sparing LRP procedures were performed in 51 (30.5%) and 10 (6%) patients, respectively. At 12 months after surgery, 3 (1.8%) patients were using 2 or more pads per day, 19 (26.4%) patients were satisfied with erection, hardness, and duration of intercourse, and 9 (12.5%) patients had an erection with insufficient hardness and duration.
Conclusion:
LRP is an acceptable method in localized prostate cancer due to its perioperative and early postoperative results.
Introduction
Prostate cancer is the second most common cancer in men worldwide, and it can be detected in a wide spectrum between clinically insignificant cancer and advanced stage cancer.1,2
Radical prostatectomy remains the gold-standard treatment for localized prostate cancer.3,4 With technological developments, minimally invasive surgical methods such as laparoscopic radical prostatectomy (LRP) and robot-assisted laparoscopic prostatectomy (RALP) have become more popular. 5 The oncological and functional outcomes of LRP and RALP are comparable with those reported for previous open retropubic radical prostatectomy (ORP) series. 5
LRP was first performed by Schuessler et al. in 1992. 6 The operation was considered difficult because the operative time was unacceptably prolonged. However, LRP was later accepted as a standard procedure due to the common belief that minimally invasive surgery would become a favorable method in Europe. Since the first LRP attempt, many urologists have acknowledged that the conventional anatomic retropubic radical prostatectomy can be adapted to laparoscopy.7,8
The aim of this study was to evaluate the oncological and functional outcomes of 167 patients who underwent LRP.
Materials and Methods
The retrospective study included 167 patients who underwent LRP due to clinically localized prostate cancer between January 2007 and April 2012. Radical prostatectomy operations were performed in a single center (Haseki Training and Research Hospital) by two experienced surgeons (A.H.T. and M.B.). Preoperative parameters, including age, serum prostate-specific antigen (PSA) level, prostate volume measured on transrectal ultrasonography, biopsy Gleason score, and serum biochemical parameters were evaluated. The histopathological analyses were performed by uropathologists using 2005 updates and 2014 WHO/ISUP consensus.9,10 Adjuvant hormonal therapy (AHT) was performed in the patients with positive surgical margins (PSM), metastasis in the regional lymph node, an initial PSA level >20 ng/mL, and pathological T3 or T2 disease with a Gleason score >7. Adjuvant external beam radiotherapy (EBRT) was performed in the patients with PSM, seminal vesicle invasion, pathological T3 or T4 disease, and postoperative continuous rising PSA values.
In our series, LRP was performed in most of our patients (134/167; 80%) using the ascending extraperitoneal approach (Heilbronn technique).11,12 The patients were positioned supine and placed in a 20–30° Trendelenburg position with both arms adducted. A 12-mm infraumbilical trocar was placed using the open Hasson technique. This port was used for removing the tissues after surgery and telescope. Four additional trocars (two 10-mm and two 5-mm) were inserted under endoscopic guidance in a “W” configuration following the creation of pneumoretroperitoneum (highest pressure: 15 mmHg). Once the entry to the space of Retzius was gained via an extraperitoneal approach, the space of Retzius was dissected and the sixth trocar (5-mm) was placed in the suprapubic region to retract the prostate anteriorly.
The endopelvic fascia was bilaterally incised and then the plexus was secured by inserting two consecutive polyglactin sutures (Vicryl MH 2/0) between Santorini's venous plexus and urethra, followed by the insertion of an endoscopic suture (Vicryl SH 2/0) in the prostate base to prevent backflow. The urethra was excised, and the prostatic apex was detached from the rectum.
The vessels coursing posterolateral to the prostate were clipped by Hem-o-lok (Weck, Teleflex Medical, IL) clips. The bladder neck dissection was initiated on the anterior wall. Subsequently, the posterior wall was incised and the retrovesical region was entered. Both vas deferens and seminal vesicles were dissected and then clipped by Hem-o-look (Weck, Teleflex Medical, IL) clips. When the prostate was completely freed, it was placed in an endobag and preserved in the space of Retzius until the end of anastomosis. The vesico-urethral anastomosis was performed using the van Velthoven running stitch technique with two 3/0 PDS RB-1 needles in different colors. 13 Following the anastomosis, the endobag was grasped with an endodissector inserted via the 12-mm trocar and then extracted via the infraumbilical port. The remaining 33 patients (20%) were treated using the transperitoneal method.
Pelvic lymph node dissection was performed in the patients with a Gleason score ≥7 and a PSA level >10 ng/mL. Unilateral or bilateral nerve-sparing procedures (NSP) were used in the patients with preoperative potency, a PSA level <10 ng/mL, and a Gleason score ≤7. Biochemical recurrence was defined as a serum PSA level ≥0.2 ng/mL in at least two consecutive measurements. Operative time was defined as the interval (minutes) between the initial incision (lower abdominal, periumbilical) and the complete closure of all wound sites or trocar incisions. Operative times and intraoperative blood loss (milliliter) and transfusion were recorded for each patient.
Postoperative hospital stay and urethral catheterization time were also recorded for each patient. Complete recovery was defined as return to everyday activities such as performing activities of daily living, exercising, driving, doing housework independently, and engaging in leisure activities.
In the LRP patients, cystographic evaluation was performed on postoperative days 7–10 and the urethral catheters were removed in the patients who did not have anastomotic leakage. In the patients with anastomotic leakage, the catheters were removed 7 days later, when no leakage was radiologically detected.
Continence and erectile functions were examined both pre- and postoperatively in all the patients. Data on postoperative incontinence and erectile dysfunction were obtained via telephone interviews. Following the catheter removal, the continence outcomes were evaluated, and the patients were advised to undertake a pelvic floor exercise program (Kegel exercises). The patients who used no more than one pad daily and had only a few urine leakages on effort or exertion were accepted as continent. 14 Postoperative potency was defined as the ability to achieve sexual intercourse with or without the use of PDE-5 inhibitors.
Results
In our series, mean age and mean serum PSA level were 62.4 ± 6.0 years and 17.5 ± 9.97 ng/mL, respectively. Six patients had a history of TUR-P. Table 1 presents the preoperative characteristics of our patients. The distribution of clinical stages was as follows: 38.2% T1, 57.6% T2, 3% T3a, and 1.2% T3b.
Patient Characteristics
Overall mean operative time was 220.5 ± 45.6 minutes with a mean anastomosis time of 35.6 ± 9.8 minutes. Extraperitoneal approach was performed in 134 (80%) patients. Pelvic lymphadenectomy was performed in 94 (56.2%) and NSP were undertaken in 61 (36.5%) patients (51 bilateral and 10 unilateral). The overall mean estimated blood loss was 325.6 ± 130 mL and perioperative blood transfusion was required in 50 patients. Table 2 presents the perioperative results of the patients. Mean length of hospital stays, and mean catheterization time were 5.6 ± 3.4 and 10.3 ± 2.2 days, respectively.
Perioperative Results
Conversion to open surgery was required in 2 patients due to hemorrhage (n = 1) and oblique dissection (n = 1). Disrupted anastomosis occurred in a patient and repaired by open surgery in the early stage (24 hours). Rectal injury occurred in 3 patients and repaired via laparoscopy. Early complications included orchitis (n = 2) and herpes sepsis (n = 1) and all of them were treated by medical therapy. The patient with herpes sepsis was treated and followed-up in the intensive care unit and discharged at the late stage (day 21). Bladder neck contracture (BNC) was detected in 4 patients (2.4%) and treated by internal urethrotomy. Bladder perforation occurred in a patient and repaired via laparoscopy.
In pathological staging, most of our patients were classified at pT2. Table 3 presents the postoperative pathologic results of our patients. PSM were observed in 35 (20.9%) patients. AHT was postoperatively performed in 120 (72%) patients, and 35 (21%) patients received AHT with adjuvant radiotherapy.
Postoperative pathologic Results
At the postoperative third month visit, 1 (0.6%) patient had continuous incontinence, 7 (4.2%) patients were using 0–1 pads daily and had stress incontinence, and 12 (7.2%) patients were using 2 or more pads per day. The other patients were using 0–1 pads per day (Table 4). In the patient with continuous incontinence, artificial urethral sphincter was implanted at 12 months after surgery and the patient had no complaint of incontinence thereafter. At 12 months after surgery, only 3 (1.8%) patients were using 2 or more pads per day.
Postoperative Functional Results
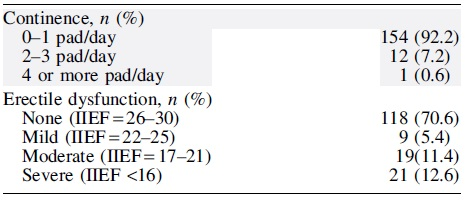
IIEF, International Index of Erectile Dysfunction.
Bilateral and unilateral nerve sparing LRP procedures were performed in 51 (30.5%) and 10 (6%) patients, respectively. At the postoperative first-year visit, 127 (76%) patients were satisfied with erection, hardness, and duration of intercourse with or without oral medical phosphodiesterase type 5 inhibitors (PDE5i) therapy (Table 4). It was revealed that all but one of the patients with improved postoperative potency with or without PDE5i treatment had undergone NSP.
Discussion
Radical prostatectomy remains the standard treatment for localized prostate cancer.3,4 Nevertheless, it is also disadvantageous since it leads to several serious complications, including hemorrhage, pain, incontinence, impotence, and BNC. LRP, when compared to open surgery, is minimally invasive and has been recommended as the standard treatment for prostate cancer over the last years. 15 In addition to providing better anatomical viewing conditions and minimal hemorrhage, LRP and RALP are reported to offer same or better functional outcomes and similar oncological outcomes compared to open surgery.13–,17
Recent studies have found no oncological risk associated with the PSM rates in ORP and LRP. In our study, the pathologic outcomes, particularly the PSM rate, were in line with the literature. In a large series reported by Anastasiadis et al., the PSM rate was revealed as 26.5%.17,18 Qi et al. reported the PSM rate as 45.9%.18,19 In the current systematic review by Moretti et al., the PSM rate was found 20.7% in LRP patients, and it was emphasized that ORP and RALP patients had similar PSM rates compared to LRP patients. 17 In our study, overall PSM rate was 20.9%. Literature shows that PSM rates vary between 6.2% and 27.5% for pT2 cancers and between 17.2% and 68.0% for pT3 cancers.15,20–27 These variations may result from the differences in patient selection, surgical skill, surgical procedures, preparation of specimens, and pathological evaluations. 28
In our study, the PSM rates were 10.79% for PT2 and 60.7% for pT3 cancers. Bladder neck preservation, NSP, and apical dissection are reported to be associated with PSM. 22 In a large series of LRP patients, Stolzenburg et al. reported that the low PSM rates in their pT2 patients (9.7%) can be attributed to the small number of patients who underwent the nerve-sparing LRP procedures. 29 Preserving the maximum urethral length during the apical dissection to improve the continence is closely associated with PSM, and the PSM rate in the prostatic apex is reported to rise up to 47%. 23 Similarly, the highest PSM in our study was measured in the prostatic apex (45%).
LRP, RALP, and ORP are associated with high prevalence of continence recovery. Nevertheless, the physiological mechanism of continence recovery after radical prostatectomy remains unknown. Kaye et al. maintained that the continence recovery after radical prostatectomy relies on the preservation of functional and structural integrity of the sphincter and its nerve supplies. The authors also reported that a meticulous apical dissection along with the preservation of the bladder neck may lead to early continence recovery. 30
In laparoscopy, the apical dissection is reported to allow minimal hemorrhage and a larger operative area since it offers less damage on the external sphincter muscle of urethra and genitourinary diaphragm. 22 Continence rates in the early period after LRP vary between 65% and 90%.14,31,32 Byung Kuk So et al. defined the social continence as using 0–1 pads daily and they reported a 94.7% continence rate at 1-year follow-up. 33 In our study, the patients had a high continence rate (92.2%) at 6-month follow-up, which can be attributed to the fact that we accepted the patients who used 0–1 pad daily as continent.
BNC, also known as anastomotic stricture, is an undesirable side effect detected in 3%–20% of ORP patients.34,35 The experience of the surgeon is the primary risk factor for BNC, followed by increased perioperative blood loss and smoking history.36,37 BNC can be prevented by ensuring a good mucosa-to-mucosa anastomosis.34,36 Comparative studies have shown that the overall incidence of BNC is lower in LRP when compared to open surgery.31,34,35 This situation can be explained by the fact that the anastomosis in LRP is tension-free and the mucosa-to-mucosa anastomosis is created under direct vision. 38 In line with the literature, BNC was present in 4 (2.4%) of our patients.
Preservation of sexual function has an important impact on quality of life in the patients treated with radical prostatectomy. Sexual function outcomes after laparoscopic or open radical prostatectomy depend on the number of neurovascular bundles preserved at surgery, the age, race, educational level, and preoperative potency of the patient, and the extent of tumor.39–41 The preservation of neurovascular bundles provides positive contribution in ORP, LRP, and RALP.40,41 Herrmann et al. reported that the potency rates in ORP, LRP, and RALP vary between 21%–90%, 39%–72%, and 36%–84%, respectively. 42 In our series, the overall potency rate was 76% and it was similar with publications.
Preservation of neurovascular bundles is an important factor in the preservation of sexual function. In the present study, 14.3% of the patients had unilateral nerve sparing and 85.7% had bilateral nerve sparing, and it was revealed that the rates of achieving sexual intercourse with or without the use of drugs were higher in the patients with bilateral nerve sparing compared to the patients with unilateral nerve sparing.
A meta-analysis, investigating the factors affecting the sexual function recovery following radical prostatectomy, evaluated 22 reports (4983 patients), published between 1985 and 2007, with study population ≥50 patients, ≥1 year follow-up, nerve-sparing status declared, and no preoperative erectile dysfunction. It was revealed that the recovery rates were higher in single-center series compared to multicenter series (60% versus 33%), in the studies reporting ≥18-month follow-up compared to the studies with <18-month follow-up (60% versus 56%), and in the patients over 60 years of age compared to the patients below 60 (77% versus 61%). However, the rates for laparoscopic and open surgery were almost similar (58% versus 57%), whereas the robot-assisted radical prostatectomy led to a higher rate (73%). 43
Our study was limited because the sample size was small, and the study was a retrospective analysis with a short postoperative follow-up period. Prospective studies with large series and long-term follow-up are needed to evaluate oncological and functional outcomes of LRP patients.
Conclusion
LRP remains a difficult procedure with a steep learning curve. Nevertheless, LRP is advantageous since it facilitates the dissection of neurovascular bundles and the prostatic apex by providing enhanced visibility of these structures. Although RALP is a more popular surgical method, depending on the oncological and functional outcomes of our study, we believe that it is possible to perform LRP in experienced centers. It should be kept in mind that LRP is an alternative surgery to open radical prostatectomy in localized prostate cancer surgery, especially in centers where access to robotic technology is not possible.
Footnotes
Acknowledgment
The authors express gratitude to everyone who helped in clinical processes and operations.
Authors' Contributions
M.K.: writing original draft, methodology, conceptualization, and investigation; M.B.: project administration; A.E.: data curation and investigation; A.H.T.: data curation and formal analysis; S.V.: writing review and editing and validation; A.Y.M.: supervision and methodology.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.