
Abstract
Introduction:
Minimally invasive surgery for ventral hernia repair (MIS-VHR) with mesh in retromuscular plane can be performed by either transabdominally (TA-RM) or via enhanced view totally extraperitoneal approach (eTEP). Although both techniques offer the mesh extension in the best anatomical space, closure of hernia defect, avoidance of traumatic fixation, the superiority of one approach over another is not established. This systematic review and meta-analysis were set up to analyze safety and efficacy of eTEP in comparison with TA-RM.
Materials and Methods:
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) framework was used as guideline to conduct systematic search of literature. Studies that provided comparative data of MIS-VHR using eTEP versus TA-RM were identified. Primary outcomes were major complications. These were defined as grade III–IV according to Clavien–Dindo classification. Secondary outcomes included: surgical site infection (SSI) rates, seroma rates, surgical site occurrence requiring procedural intervention (SSOPI), minor complications (Clavien–Dindo grade I–II), intraoperative complications, recurrence rate, postoperative ileus, duration of surgery, postoperative pain. Random- and fixed-effects models of statistical analysis were used. Risk difference (RD) was computated for binary outcomes (major and minor complications, SSI, seroma, SSOPI, recurrence, ileus) with 95% confidence intervals. I2 test was used to assess statistical heterogeneity. Risk of bias assessment was performed using Newcastle–Ottawa framework.
Results:
There were 3 observational studies that enrolled 370 participants. In the eTEP group there were 166 patients and, in the TA-RM group there were 204 patients. There was no significant RD with regard to major complications (RD −0.02 [−0.06 to 0.02], test for overall effect: Z = 0.86 [P = .39]). There was no significant RD in occurrence of minor complications, SSI, seroma, SSOPI, recurrence, ileus.
Conclusions:
Both eTEP and TA-RM were found to have equal safety profile. Further high-quality studies evaluating patient reported outcomes and late recurrence may be useful.
PROSPERO registration number: CRD42023429160.
Introduction
Over the last three decades minimally invasive surgery for ventral hernia repair (MIS-VHR) has undergone evolution in several directions. This included modifications in the approach (hybrid, laparoscopic, robotic), the plane of mesh placement (intraperitoneal, preperitoneal, retromuscular, totally extraperitoneal), mesh characteristics, and fixation devices. The first description of MIS-VHR dates to 1993, when LeBlanc et al. described intraperitoneal onlay mesh (IPOM). 1 It remains to be the widely used technique, although the main criticism remains to be consequences of adhesiogenic effect of intraperitoneal mesh. Adhesions, bowel obstruction, enterocutaneous fistulas are recognized sequalae of IPOM.2–4 Other undesirable outcomes of IPOM are related to traumatic fixation of the mesh, mesh bridging, and cosmetic effects related to bridging. Chelala et al. proposed the technique of fascial approximation to close the hernia defect in patients undergoing IPOM in 2003. 5 This technique is widely referred to as IPOM+ and is aimed to overcome problems related to bridging.
However, the superiority of IPOM+ over IPOM is yet to be established in high-quality studies. 6 Transperitoneal (transabdominal) preperitoneal (TA-PP) and retromuscular (TA-RM) techniques of mesh repair were developed to solve drawbacks of IPOM.7–9 MIS-VHR using TA-RM involves retromuscular placement of mesh above the posterior rectus sheath and resembles gold standard open Rives–Stoppa operation.10,11 The enhanced view totally extraperitoneal (eTEP) operation has been described as the new approach to the retromuscular space. 12 In all techniques of preperitoneal and retromuscular mesh placement, the advantage is mesh extension in the extraperitoneal space, closure of hernia defect, avoidance of traumatic fixation, cost saving on mesh, and avoidance of fixation devices. eTEP is believed to be associated with lower risk of visceral injury owing to totally extraperitoneal space of dissection, although this technique is associated with more difficult hernia content assessment and may be considered to have a longer learning curve.
eTEP can be considered advantageous for patients with pneumoperitoneum intolerance. Uncertainty exists about the best extraperitoneal MIS-VHR technique. Systematic reviews and meta-analyses reported the short-term outcomes of eTEP approach for MIS-VHR.13,14 The systematic review of Maatouk et al. assessed safety and feasibility of transabdominal preperitoneal approach for MIS-VHR. 15
We are not aware of systematic reviews that compared eTEP with TA-RM. The aim of this study was to explore noninferiority between eTEP and TA-RM in short-term outcomes.
This systematic review and meta-analysis were initiated to gather comparative data on major and minor complications, surgical site occurrence rates (seroma and surgical site infection) including the ones that required procedural interventions, ileus rates, postoperative pain, and recurrence in patients undergoing eTEP versus TA-RM. Where it was possible, we also aimed to collect and analyze information available in included studies on individual circumstances of adopting both techniques as well as switching from one technique to another.
Materials and Methods
Search strategy
The project was registered with PROSPERO prospectively (CRD42023429160). Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) framework was used as guidelines to conduct systematic search of literature. 16
The search terms were designed to identify studies that provide direct comparison of eTEP and TA-RM modifications of MIS-VHR. Designated search terms (including their synonyms and variants) and their combination using the Boolean AND/OR operators were used: laparoscopic, robotic, minimally invasive, ventral hernia repair, umbilical hernia repair, incisional hernia repair, e-TEP, sublay repair, retromuscular, retrorectus, Rives–Stoppa.
Medline and Embase databases were comprehensively searched. Searches had no time restriction and covered time period from the date of inception of each database to June 3, 2023. Database searches included studies published in English language. No restrictions were placed on regional state to ensure that relevant studies are not missed. Two reviewers looked for relevant publications that provided direct comparison of eTEP and TA-RM and modifications of these techniques in patients undergoing MIS-VHR. Manual search of all shortlisted publications was performed to screen for potentially eligible studies. Detailed algorithms of search for each database are available in Supplementary Appendix S1.
Inclusion criteria
Studies published in English that fulfilled the following criteria were included: (1) studies that compared two techniques of retromuscular mesh placement in patients undergoing predominantly midline MIS-VHR: eTEP and its modifications with TA-RM and its modifications for uncomplicated hernia, and (2) full text articles.
Exclusion criteria
Studies were excluded from analysis: (1) studies in which it was not possible to extract data from the published results, (2) studies that contained re-published data, (3) studies published in other language than English, and (4) publications that are editorials, comments, letters, review articles, conference abstracts, retractions, and case reports.
Outcome measures
Primary outcomes for this study were major complications. These were defined as grade III–IV according to Clavien–Dindo classification. 17 Secondary outcomes included the following: surgical site infection (SSI) rates, seroma rates, occurrences at surgical site that necessitate procedural intervention (SSOPI), cumulative outcome of minor complications (defined as grade I–II complications of Clavien–Dindo classification), intraoperative complications, recurrence rate, postoperative ileus, length of surgery, length of stay (LOS), postoperative pain, and quality of life. SSOPI was defined as any wound reopening or debridement, excision of sutures, transcutaneous drainage, posterior wall dehiscence causing strangulation and requiring reoperation or mesh removal. 18
Study selection
Study eligibility and methodological quality assessments were independently performed by two investigators (Y.T. and A.K.) using a standardized data form according to the predetermined selection criteria. Senior author (D.J.P.) was approached to resolve differences of opinion.
Data extraction
Data extraction from selected studies was performed by two reviewers (A.K. and I.D.). Following data were extracted: basic characteristics (author, year, sample size); patient characteristics; characteristics of hernia; outcomes of comparison. Disputes were resolved by discussion. If consensus was not reached a senior third person (D.J.P.) had been involved.
Risk of bias assessment
Independent assessment of included studies for quality and validity was performed by two investigators using the Newcastle–Ottawa score. Selection of patients, comparability of the study groups, and assessment of outcome were calculated, respectively, and then these scores were added up to get a cumulative score where the maximum possible total score was 9, and studies with scores ≥7 were defined as high quality. 19 Consensus discussion was used to resolve disagreements.
Statistical analysis
Revman software, version 5.3 (Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen), was used to perform meta-analysis. Fixed- and random-effects models were utilized. Risk differences (RD) were computed for binary endpoints using the Mantel–Haenszel method. A 95% confidence interval (CI) was identified. Forrest plots were used for graphical presentation of results. Between-study heterogeneity was analyzed by the I2 test. 20 If the I2 statistic was >50%, heterogeneity was declared as significant, a random-effects model statistics were used.
Results
Study selection
Primary search identified 620 publications. There were 209 duplicate studies. Primary screening that included analysis of titles and abstract eliminated 398 studies. Ten studies were precluded after full text screening. Articles of the remaining three studies after full-text analysis were accepted into the review and meta-analysis.21–23 The PRISMA flow diagram is given in Figure 1.
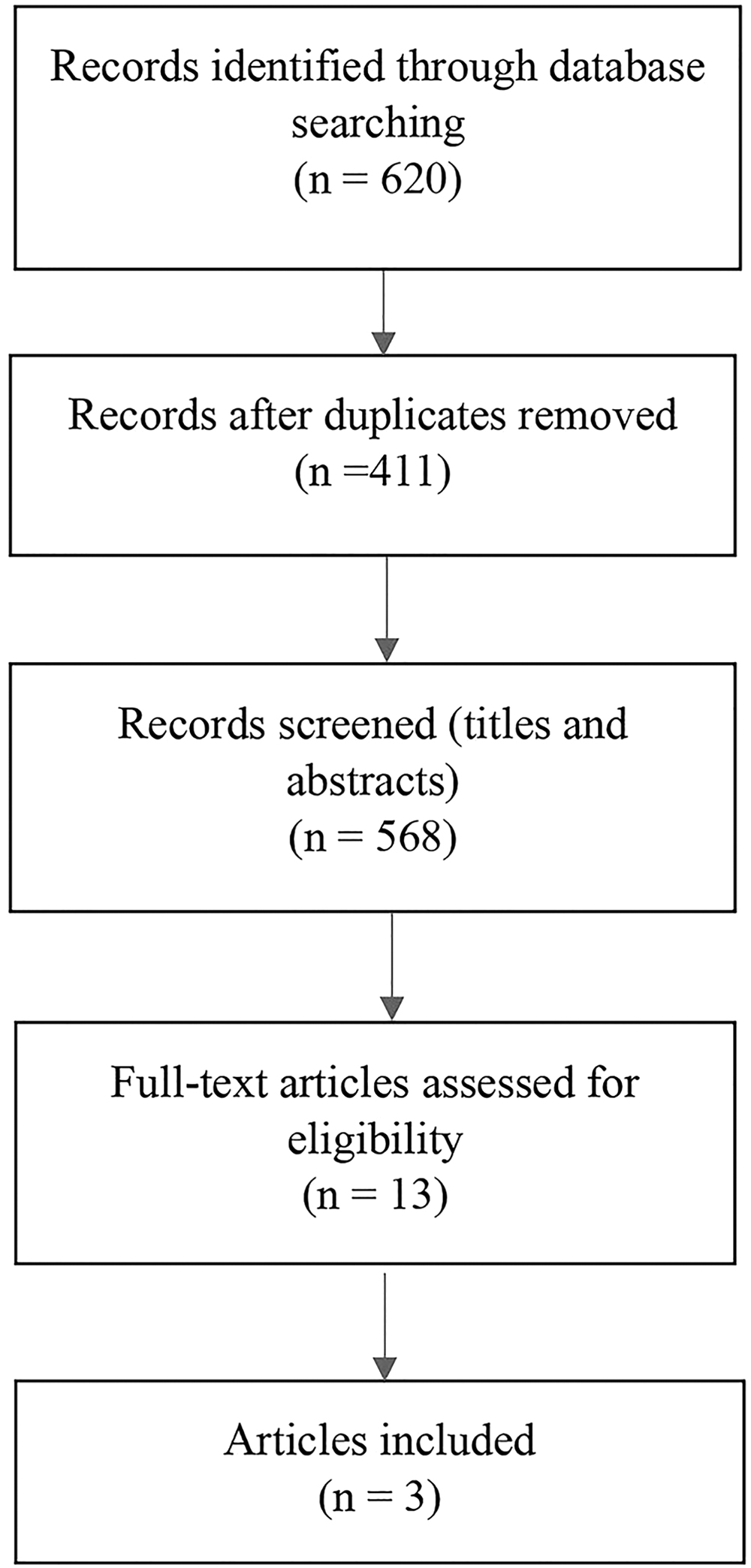
Flowchart of the literature search.
Study characteristics
Three observational studies that included 370 patients were included in the analysis.21–23 These studies included participants who underwent MIS-VHR repair using eTEP technique and TA-RM technique. In all three studies patients in both groups had robotic surgery. A total of 166 were allocated and received intervention in the eTEP group and 204 patients in the TA-RM group.
In the study of Olivier et al. a retrospective analysis was provided for a group of patients who had robotic TA-RM between April 2019 and December 2019. 21 The same surgeon performed robotic eTEP between December 2019 and January 2022. 21 Both eTEP and TA-RM techniques were new to the surgeon and database was collected during the learning curve of the surgeon. 21 The transabdominal hernia approach in the study of Olivier et al. was described as robotic transabdominal retromuscular umbilical mesh repair, and the extraperitoneal approach was regarded as inverted total extraperitoneal repair owing to initial development of extraperitoneal plane in the suprapubic region and advancement of the plane in a “bottom-up” (caudal-to-cranial) direction. 21
In the study of Zaman et al., a retrospective data of robotic MIS-VHR by a surgeon with initial experience in TA-RM (January 2012–March 2016) and eTEP (April 2018–August 2019) was reported. 22 In the study of Kudsi et al. the observational retrospective data from participants who had robotic MIS-VHR at a single center during the study period February 2013–October 2019 were obtained. 23 Over time, and at the surgeon's choice, there was a transition of preference from robotic TA-RM (beginning of the study period) to the robotic eTEP that was more commonly performed at the late stage of the data collection. 23
All patients in the study of Olivier et al. were operated for midline hernias and no adjunctive procedures were performed. 21 Eighty-four percent of patients in both groups in the study of Zaman et al. had surgery for midline defects. 22 There was no significant difference between groups in the rate of concurrent procedures (20%, P = .55), and the most common concurrent procedure reported was bilateral groin hernia repair. 22 In the study of Zaman et al., 10% of patients in the eTEP group as opposed to 22% in the TA-RM group had transversus abdominis release (TAR) (P = .02). 22 The majority of patient in the study of Kudsi et al. were operated for midline hernias and the rate of TAR did not differ statistically between the eTEP and TA-RM groups. 23 Study characteristics are given in Table 1.
Preoperative Characteristics
Median and interquartile range.
Mean and standard deviation.
BMI, body mass index; eTEP, extended totally extraperitoneal repair; NP, not provided; PSM, propensity score matching analysis; RCC, retrospective cohort controlled; RPCC, retrospective analysis of a prospectively maintained database; TA-RM, transabdominal retromuscular.
Risk of bias
Journal articles were assessed to analyze study quality and risk of bias. The nonrandomized design of included studies and lack of multicenter recruitment raise concern of selection bias. Studies of Olivier et al. and Zaman et al. provided comparison of two techniques between two patient groups of similar baseline characteristics, hence no major concerns with comparability.21,22 In the study of Kudsi et al. propensity score matching technique was used to adjust for imbalance in patient characteristics between the studied groups. 23 However, the statistical technique of propensity score matching risks to introduce model dependence and impair generalizability of results to a wider population. 24 The fact that sensitivity analysis was not performed to confirm that results are the same despite group differences increases the possibility of selection and interpretation bias.24,25 The risk of bias summary using Newcastle–Ottawa score is provided in Table 2.
Newcastle–Ottawa Score for Observational Studies
Primary outcomes
Major complications (Clavien–Dindo III–IV)
In the study of Olivier et al. a reoperation to treat small bowel obstruction caused by a rupture of the posterior rectus sheath (grade IIIB) after an eTEP approach was required for 1 patient. 21 In the study of Zaman et al. in the TA-RM group, there were 4 episodes of complications in a total of 4 patients that necessitated procedural intervention and required general anesthesia. 22 Two patients developed mechanical intestinal obstruction caused by intraabdominal adhesions requiring laparotomy. 22 There were 2 patients who had SSI that required excision and drainage. 22 In the eTEP group—2 patients required drainage under local anesthetic. 22 In the study of Kudsi et al. there was no difference in the major complication rate. 23
In the TA-RM group, in one episode there was need in percutaneous evacuation of seroma, in one episode a patient required mesh explantation owing to deep SSI, 1 patient required re-intervention owing to infected peritoneal dialysis catheter and peritonitis, and 3 patients required intensive care unit (ICU) admission owing to acute respiratory deterioration and adrenal failure, which was associated with steroid dependence (complications grade-IIIA, grade-IIIB, grade-IIIB, grade-IVA, respectively). Although the last four events may be considered being not directly related to the hernia surgery, the significance of the severity of these events is high. 23 There was little information in the report detailing perioperative management and subsequent events of patients with renal failure, chronic liver pathology, and steroid dependence. 23
In the eTEP group, there was one episode of transcutaneous drainage owing to SSI and ICU admission was needed in another patient owing to hepatic encephalopathy associated with previously diagnosed chronic liver disease (grade-IIIA and grade-IVA, respectively). 23 There was no significant RD between two studies in major complications when meta-analysis was performed (RD −0.02 [−0.06 to 0.02], test for overall effect: Z = 0.86 [P = .39]; Fig. 2).
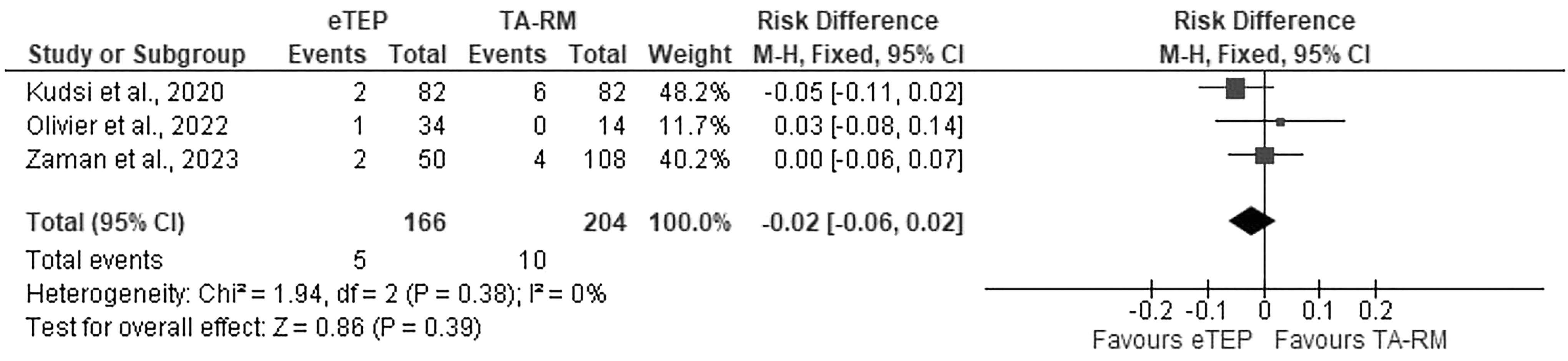
Forrest plot 1. Major complications. e-TEP, enhanced totally extraperitoneal repair; TA-RM, transabdominal retromuscular repair.
Secondary outcomes
Surgical site infection
There were no reports of SSI in the study of Olivier et al. 21 In the study of Zaman et al. there was one reported episode of SSI in the eTEP group and three episodes in the TA-RM group. 22 There were four episodes of SSI reported in the TA-RM group and one episode in the eTEP group in the study of Kudsi et al. 23 There was no difference between two groups in the occurrence of SSI (RD −0.02 [−0.06 to 0.01], test for overall effect: Z = 1.18 [P = .24]; Fig. 3).

Forrest plot 2. SSI. e-TEP, enhanced totally extraperitoneal repair, TA-RM, transabdominal retromuscular repair; SSI, surgical site infection.
Seroma
There was no difference between two groups in the occurrence of seroma (RD −0.04 [−0.19 to 0.12], test for overall effect: Z = 0.46 [P = .65]; Fig. 4).
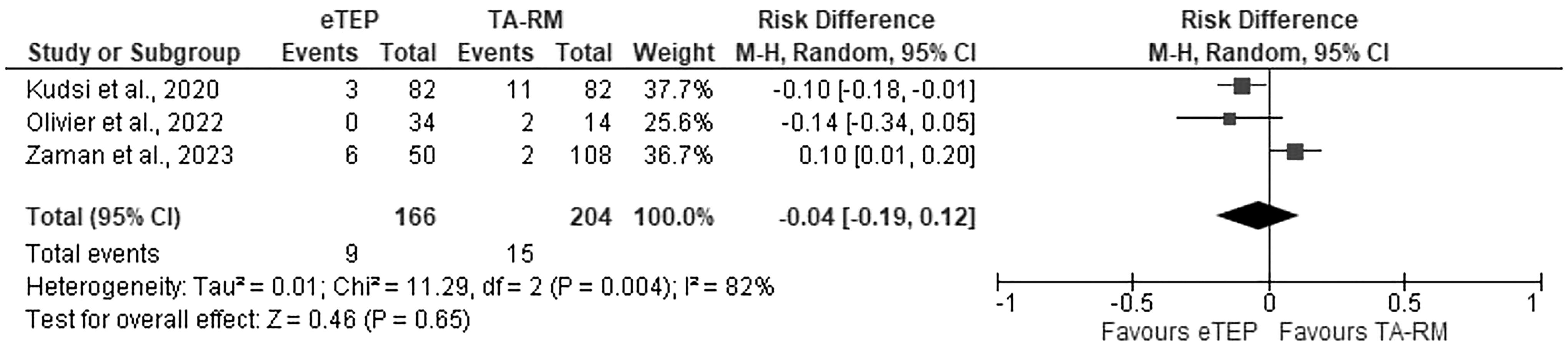
Forrest plot 3. Seroma. e-TEP, enhanced totally extraperitoneal repair, TA-RM, transabdominal retromuscular repair.
Cumulative outcome of minor complications (Clavien–Dindo I–II)
Among minor complications, not related to the operative site, there were rare reports of superficial vein thrombosis in the lower extremity and ischialgia.21–23 Meta-analysis demonstrated no risk difference in minor complications between two groups (RD −0.1 [−0.27 to 0.08], test for overall effect: Z = 1.09 [P = .28]; Fig. 5).
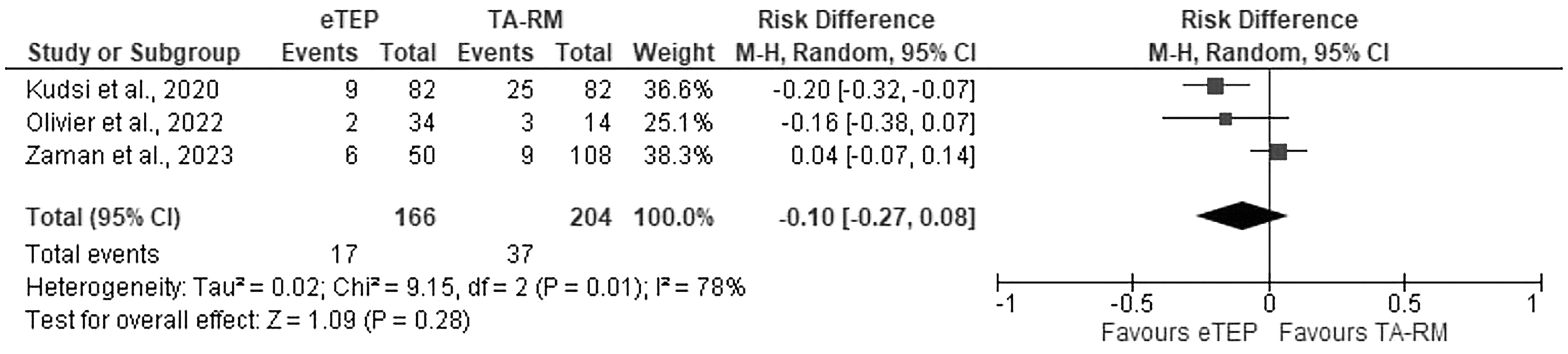
Forrest plot 4. Minor complications. e-TEP, enhanced totally extraperitoneal repair, TA-RM, transabdominal retromuscular repair.
Surgical site occurrence requiring procedural intervention
In the study of Olivier et al. there were no SSOPI in the TA-RM group, whereas 1 patient in the eTEP group required return to theater for a rupture of the posterior wall of the rectus sheath. 21 In the study of Zaman et al. there were two reported episode of seroma drainage in the eTEP group, whereas in the TA-RM group 2 patients had SSI that required debridement. 22 In addition, 2 patients had seroma that required drainage owing to chronic discomfort. 22 In the study of Kudsi et al. 3 patients in the TA-RM group required percutaneous seroma drainage, whereas in the eTEP group there was one SSOPI. 23 There was no difference between two groups in the occurrence of SSOPI (RD −0.01 [−0.04 to 0.03], test for overall effect: Z = 0.38 [P = .71]; Fig. 6).
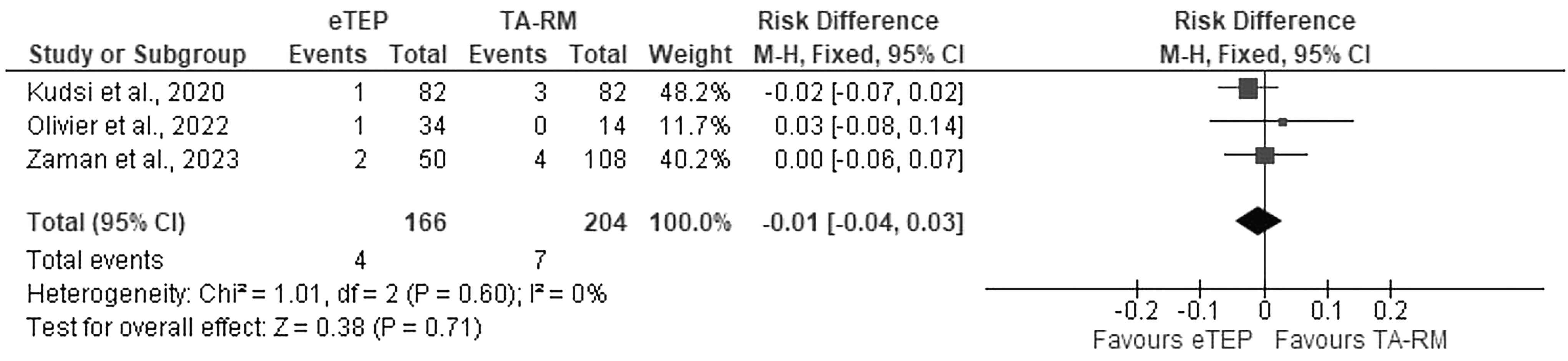
Forrest plot 5. SSOPI. e-TEP, enhanced totally extraperitoneal repair, SSOPI, surgical site occurrences requiring procedural interventions; TA-RM, transabdominal retromuscular repair.
Recurrence
Although no recurrences were registered in studies of Kudsi et al. and Oliver et al., there were 2 registered recurrences in the eTEP group and 12 in TA-RM group in the study of Zaman et al.21–23 The median follow-up in the study of Kudsi et al. for eTEP group was 15 months and for the TA-RM it was 35 months. 21 The average follow-up for the entire patient group in the study of Kudsi et al. was registered as 14.6 months. 23 In the study of Zaman et al. the follow-up period for both patient groups was 1 year. 22 The average time to recurrence was reported to be 9.17 months in the eTEP group and 11.05 months in the TA-RM group. 22 When meta-analysis was performed, there was no RD in the recurrence rate (RD −0.02 [−0.09 to 0.05], test for overall effect: Z = 0.58 [P = .56]; Fig. 7).
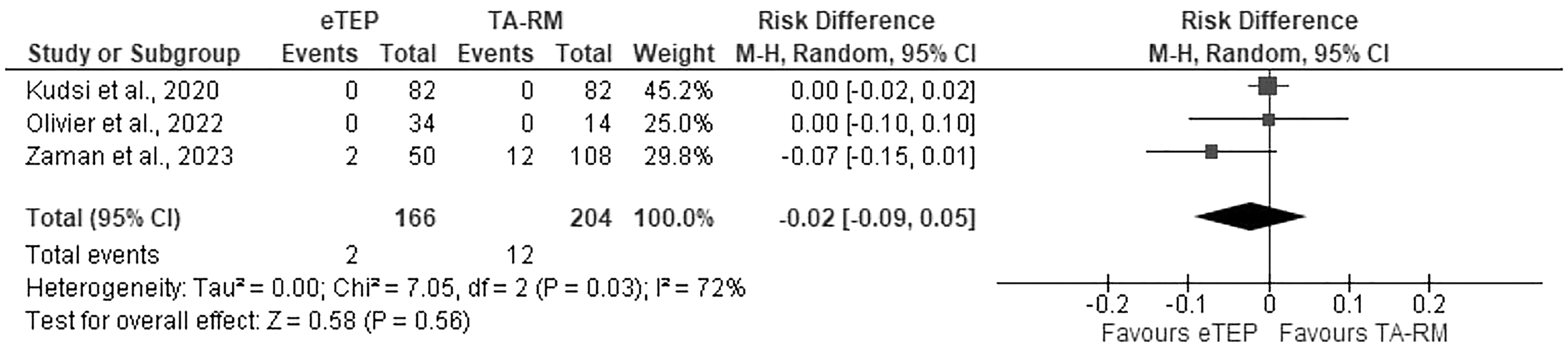
Forrest plot 6. Recurrence. e-TEP, enhanced totally extraperitoneal repair, TA-RM, transabdominal retromuscular repair.
Ileus
Study of Kudsi et al. and Zaman et al. analyzed occurrence of postoperative ileus.22,23 In both studies ileus was reported in TA-RM group only, with the rate of ileus being 2.4% in the study of Kudsi et al. and 2.8% in the study of Zaman et al.22,23 The findings of no difference were borderline in the meta-analysis, although statistical significance of one technique over another in this outcome was not shown (RD −0.03 [−0.06 to 0.00], test for overall effect: Z = 1.71 [P = .19]; Fig. 8).
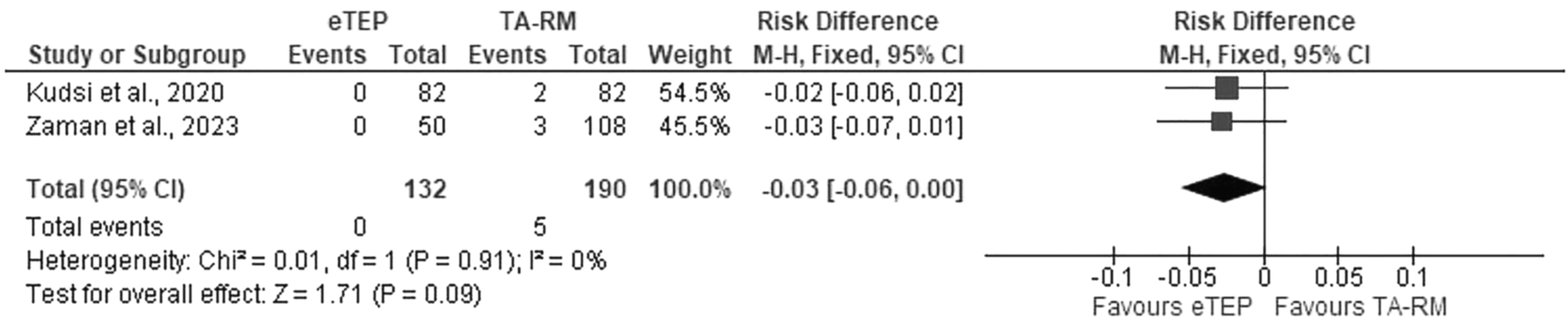
Forrest plot 7. Ileus. e-TEP, enhanced totally extraperitoneal repair, TA-RM, transabdominal retromuscular repair.
Conversion and intraoperative complications
There were no record of complications during surgery or conversion to another procedure in both groups in the study of Olivier et al. 21 In the study of Zaman et al. 1 patient (2%) had conversion to open surgery because of difficulties with approximation of wound edges despite posterior component separation and 2% had conversion from the eTEP to the TA-RM. 22 Among the 108 TA-SM cases, only 79% received intended treatment. 22 There were two conversions to open for the following reasons: devitalized skin intraoperatively and full thickness bowel injury on port insertion introduction. 22 Nineteen patients (18%) had IPOM repairs owing to disintegration of the peritoneal flap after dissection. 22 There were 2% of patients who required mesh-free closure because of contamination concerns. 22
In the study of Kudsi et al. intraoperative complications occurred in 4.9% cases of TA-RM repair as compared with no intraoperative complications in TEP-RM group. 23 All complications that occurred during surgery were reported to happen during adhesiolysis. 23 Two patients had intestinal injuries at serosal depth. 23 One patient had enterotomy, and another had a bladder opening. 23 No conversions were reported. 23 However, a skin incision was required to insert the prosthesis in 3.7% of patients in the TA-RM group and 4.9% patients in the TEP-RM group (P = 1.000). 23
Operative time and LOS
In the study of Kudsi et al. operative time for eTEP was found to be significantly lower (median of 122 [range 88–185] minutes in eTEP group versus median of 161.5 [97–240] minutes in TA-RM group, P = .015). 23 In the study of Olivier et al., the median intraoperative time was 158 minutes (range 95–260) in the eTEP group, and 195 minutes (90–330) in the TA-RM. 21 The median LOS for both groups was reported to be 1 day. 21 In the study of Zaman et al. the mean operative time for the eTEP group was 158.3 (±90.6) and for the TA-RM group it was 155.8 minutes (±65.2; P = .84). 22 Mean LOS was 1.3 (±1.2) in the eTEP versus 2.2 (±3.0) in the TA-RM. 22 Owing to variability in reporting operative time and LOS meta-analysis was not performed.
Pain and quality of life
In the study of Kudsi et al. the median (interquartile range) postoperative pain scores were recorded when leaving postanesthesia care facilities (early postoperative period). 23 These did not differ significantly between the two groups (P = .541; 5 [3–6] in TA-RM versus 5 [4–6] in TEP-RM). 23 The quality-of-life data were not provided. Owing to insufficient data meta-analysis on postoperative pain and quality of life was not feasible.
Assessment of reporting biases
Reporting bias was not assessed as there was insufficient number of studies.
Discussion
Our study did not identify significant difference between eTEP and TA-RM in major complications and secondary outcomes. Studies included in our review reported different rate of intraoperative complication and conversion rate. Equally, our report demonstrated variability in operative time between two procedures. Based on results of our review and meta-analysis we were not able to demonstrate superiority of one technique over another if both are performed robotically. As far as we are concerned, this is the first systematic review and meta-analysis that provided direct comparison of eTEP and TA-RM techniques of MIS-VHR.
There are limitations in our study. Our review is based on observational studies and the total number of included studies is low. Important confounding that one should be mindful of when reading our review and the one we could not control for is variability in technical operative experience between surgeons who performed operations for patients included in study. Surgical experience and completion of learning curve for new procedure affect clinical outcomes. 23 Data of individual databases of included studies were mostly performed by surgeons who were early in their learning curve for both techniques. At the same time, all three research groups represent high volume abdominal wall reconstruction centers. Therefore, safety data from the review may not be representative of other centers with less or more experience in eTEP and TA-RM. Another limitation of our study is that the included studies were heterogenic in clinical data such as patient and hernia characteristics and operative description.
Giving existing uncertainty and clinical equipoise at present there is no sufficient evidence to advocate one technique over another in MIS-VHR surgery. Further high-quality studies evaluating patient reported outcomes and late recurrence in various modification of MIS-VHR may be useful.
Footnotes
Authors' Contributions
Y.T.: study registration (lead), conceptualization and methodology (lead), data search (lead), selection of studies (lead), data synthesis (lead), writing (lead).
I.D.: data extraction (equal), data synthesis (supporting), writing (supporting).
A.K.: study registration (supporting), selection of studies (supporting), data extraction (equal), editing (supporting).
D.J.P.: conceptualization (supporting), writing reviewing (supporting), editing (lead).
Availability of Data and Material
Data available on reasonable request.
Disclosure Statement
Y.T., I.D., and A.K. have no conflicts of interest or conflicting financial ties to disclose.
D.J.P. receives fees for professional education and consultancy from Johnson and Johnson and Medtronic.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.