
Abstract
Introduction:
The use of mesh for paraesophageal hernia repair is controversial due to concerns about long-term complications. This study aimed to investigate whether preoperative imaging characteristics of diaphragmatic hernia could predict the need for mesh repair.
Methods:
The records of all patients who underwent laparoscopic diaphragmatic hernia repair between September 2015 and September 2022 were reviewed. Patients' preoperative computerized tomography (CT) imaging was reviewed and was correlated with mesh repair.
Results:
A total of 53 patients were included in the study. Volumetric measurements were obtained from preoperative CT scans to assess hiatal defect area (HDA) and hernia sac volume (HSV). Mesh repair was required in 43.4% of cases, all among types II–IV. The mesh repair group had a higher mean hiatal neck height (50.8 ± 16.35 versus 43.22 ± 17.08 mm, P < .032) and higher HSV (708.53 ± 577.6 versus 346.866 ± 321.65 cm3, P < .003). There was also a borderline difference in HDA mean values (23.78 ± 17.22 versus 16.8 ± 10.41 cm2, P < .059).
Conclusions:
Preoperative HSV on CT scans can be a valuable predictor for the need for mesh repair during hiatal hernia surgery, aiding surgical planning and decision-making. Further research is needed to validate these findings and optimize hernia repair outcomes.
Introduction
Hiatal hernias (HH) are common among the adult population and have been reported to affect 10%–50% of the population in varying degrees. Symptomatic patients are usually initially managed nonsurgically. Patients who remain symptomatic, although optimal medical therapy are offered surgical repair of their hernia. 1 Crural closure is one of the most difficult technical steps during the repair, and primary closure is preferred. Mesh repair is indicated in certain situations in which suture repair is not possible. Crural suture tension is assessed subjectively by the surgeon based on his experience performing the procedure rather than objective hernia characteristics.
The purpose of this study was to determine whether preoperative imaging characteristics of diaphragmatic hernia correlate with the need for mesh repair rather than suture repair. Establishing such a relationship may aid the surgeon in surgical planning and intraoperative decision-making.
Materials and Methods
Study population
Institutional review board approval was obtained for this study. The records of all patients who underwent hiatal hernia repair in a university hospital between September 2015 and September 2022 were reviewed. Data regarding patients' demographics, comorbidities, hernia type, preoperative symptoms, operative details including mesh repair, the need for relaxing incision, length of stay, postoperative outcomes including early and late complications, and hernia recurrence were collected. Patients' preoperative imaging was reviewed. Patients were included in the study if the entire extent of the crural defect and sac was visible on the preoperative chest and/or abdominal computerized tomography (CT) scans.
CT measurements
CT scans were performed on a Philips iCT family 256, 2 detector rows 2 × 128, with radiation dose, adjusted for scanner type. The data abstractors used the Picture Archiving and Communication System (iSite PACS version 12.1.5.1046; Carestream, Quantum Medical Imaging LLC, Rochester, New York) to archive the images for interpretation and to obtain measurements. Volumetric analysis software performed three-dimensional (3D) reconstruction with volumetrics of all HH with preoperative CT scans available. CT images were loaded into a common multiplanar reformat package, which displayed images in three orthogonal planes. All CT measurements were performed by a single radiologist and then independently verified by 2 other radiologists.
Using the following steps, multidimensional rotation of CT images allowed visualization of the entire hiatal defect, simulating the surgeon's view during repair (Fig. 1). To begin, a frontal and sagittal plane line was established to determine the length (cm) and diameter (mm) of the left and right crura (Fig. 1A). Another frontal plane was made to measure the neck height (mm) (Fig. 1B). The neck width (mm) was then measured using a transversal plane (Fig. 1C).
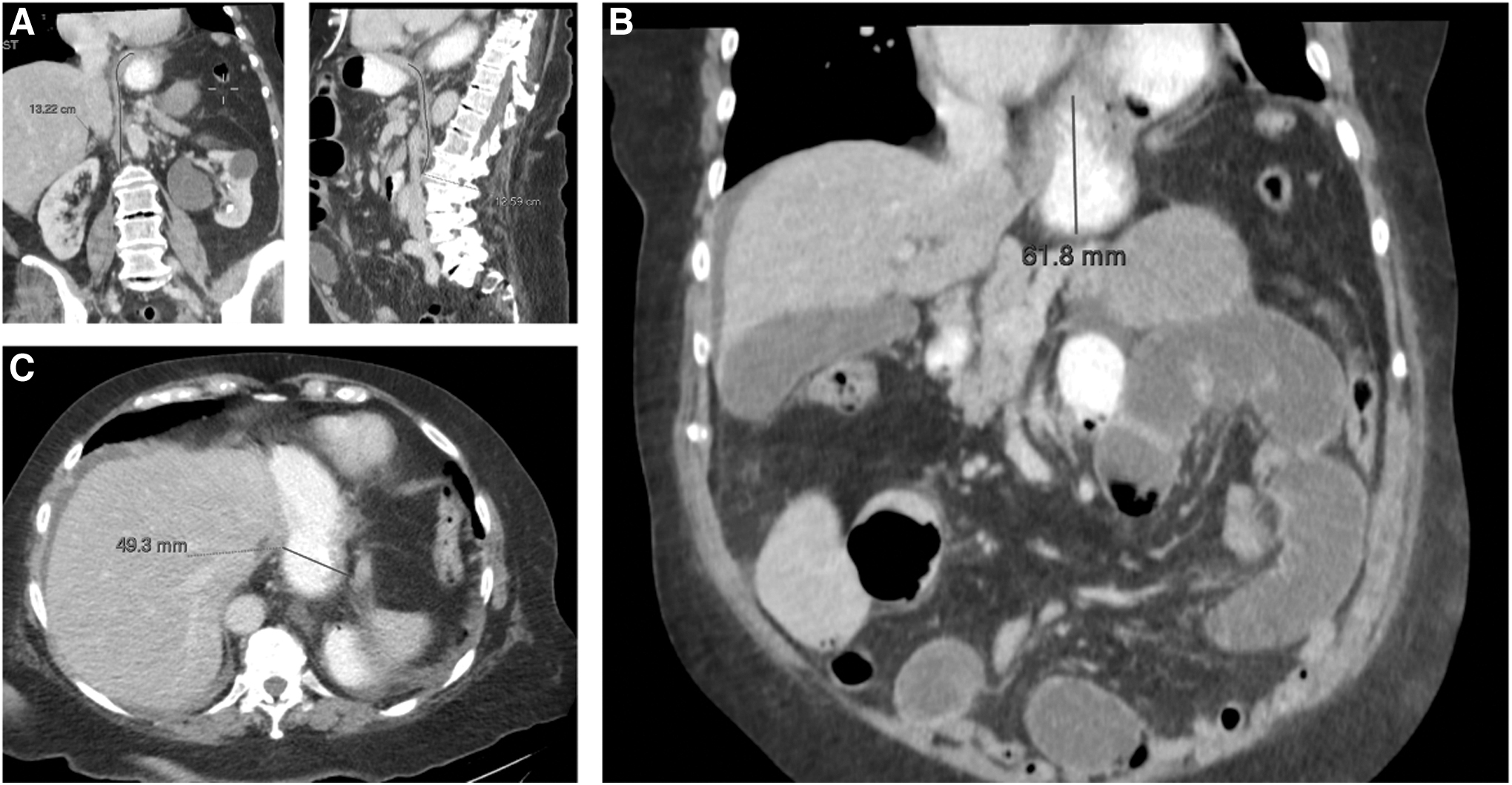
Visualization and measurements of CT parameters.
The inner margin of the hiatus was manually outlined with a polygon tool, yielding a measured hiatal defect area (HDA) (Fig. 2A). To obtain the hernia sac volume (HSV) measurements, the entire intrathoracic hernia sac was manually outlined on multiple sequential axial images, yielding volume measurements based on a sum of exact area dimensions according to integrative algorithms used by the software (Fig. 2B).
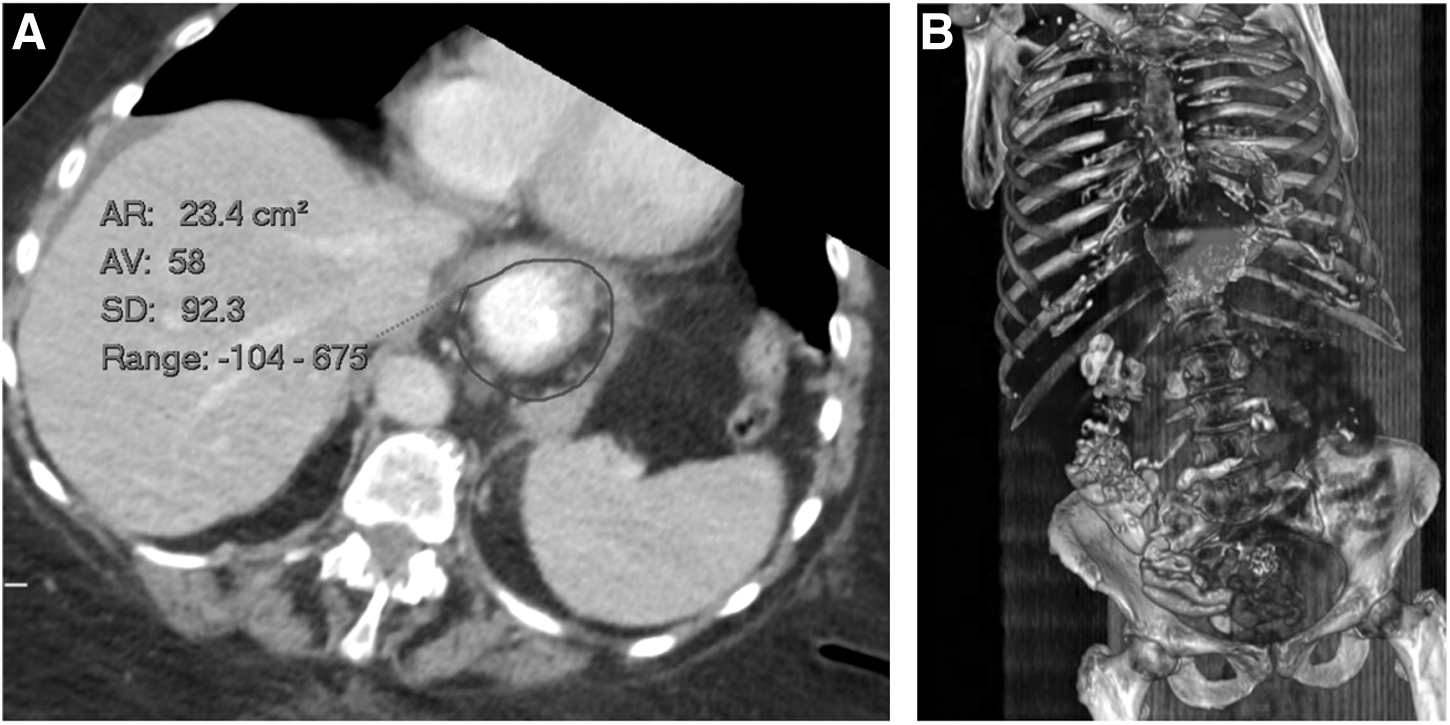
Visualization and measurements of HSV and HDA.
Operative techniques and outcome
All hernias were repaired laparoscopically by a single surgeon. After opening the peritoneum at the neck of the hernia, the sac was dissected off the mediastinum by blunt and sharp dissection. Once the entire sac had been reduced and 2–3 cm of intra-abdominal esophagus obtained, the short gastric vessels were divided. Primary crural repair was attempted in all patients. In cases where tension developed over the suture line, mesh repair was employed, with or without the right crural relaxing incision. In cases a relaxing incision was performed, a C-shaped synthetic composite mesh covering the relaxing incision and crurorrhaphy was placed. Either complete or partial fundoplication was performed in all cases, depending on preoperative esophageal motility evaluation.
Statistical analyses
Categorical and nominal variables are reported by prevalence and percentages, and continuous variables are reported as means ± standard deviations and skewed variables as a media. Continued variables between the various study groups were tested for normality by the Shapiro–Wilk test. For abnormal distribution, nonparametric tests will be performed (Mann–Whitney test) to compare the 2 groups. Categorical and nominal variables were analyzed by Pearson's chi-square (χ 2 ) test. A logistic regression model containing HSV and HDA was generated. Receiver operating characteristic (ROC) curve (Fig. 5) determines when a specific index will aid in predicting the use of a mesh repair.
All statistical tests were carried out with a significance level of 0.05 (two-sided). All reported P values were rounded to three decimal places. The Statistical Package for Social Sciences for Windows was used for all statistical analyses (version 22; IBM SPSS Statistics for Windows; IBM Corporation, Armonk, NY).
Results
A total of 82 patients underwent diaphragmatic hernia repair during the study period. Of these, 53 patients met the inclusion criteria and were included in the study. The mean age was 70 ± 8.5 years (70 ± 9.06 years for mesh repair cases versus 70.03 ± 8.2 years for suture repair, P = .74; Table 1). Most patients were female (66%). Mesh repairs were required in 23 cases (43.4%).
Cohort Characteristics
Bold values considered significant if P < 0.05.
GI, gastrointestinal.
Most HH were type III (52.8%), followed by type IV and type II hernias. No type I hernias required mesh repair (0%, P = .023). Most mesh-repaired hernias were type III. Preoperative complaints were similar between groups (Table 1).
Mesh repair patients were more likely to have relaxing incisions (18 [100%] versus 0 [0%], P = .0001). Other operative details and outcomes were similar between groups (Table 2). Hernia and postoperative characteristics are also detailed in Table 2.
Operative Details and Outcomes
Mean, days.
Mean, months.
All included patients had preoperative CT imaging suitable for volumetric analysis, of whom 23 cases (43.4%) underwent mesh repair. Volumetric measurements of this subset of patients are reported in Table 3. The mesh repair group had a higher mean hiatal neck height (50.8 ± 16.35 versus 43.22 ± 17.08 mm, P < .032) and higher HSV (708.53 ± 577.6 versus 346.866 ± 321.65 cm3, P < .003). There was also a borderline difference in HDA mean values (23.78 ± 17.22 versus 16.8 ± 10.41 cm2, P < .059) (Fig. 3).

Correlation between volumetric measurements and mesh repair. Mann–Whitney test analysis of patients' mean ± SEM. *P < .05, **P < .005. SEM, standard error of the mean.
Computerized Tomography Imaging Variables
Bold values considered significant if P < 0.05.
HDA, hiatal defect area; HSV, hernia sac volume.
Hernia sac volume
Among all patients, the mean HSV was 506.83 ± 483.34 cm3. A statistically significant relationship was found between several preoperative complaints and the degree of HSV. Patients who presented with complaints such as hoarseness, dysphagia, epigastric abdominal pain, and heartburn had lower HSV compared with those who did not. Patients who presented with shortness of breath had higher HSV than those who did not (hoarseness: 68.28 ± 87.27 versus 524.37 ± 484.59, P = .038; dysphagia: 220.44 ± 185.71 versus 566.77 ± 505.82, P = .014; epigastric abdominal pain: 281.19 ± 188.344 versus 672.3 ± 564.1, P = .003; heartburn: 368.93 ± 379.59 versus 607.96 ± 530.57, P = .027; and shortness of breath: 802.84 ± 248.92 versus 475.34 ± 493.03, P = .015) (Table 4 and Fig. 4).
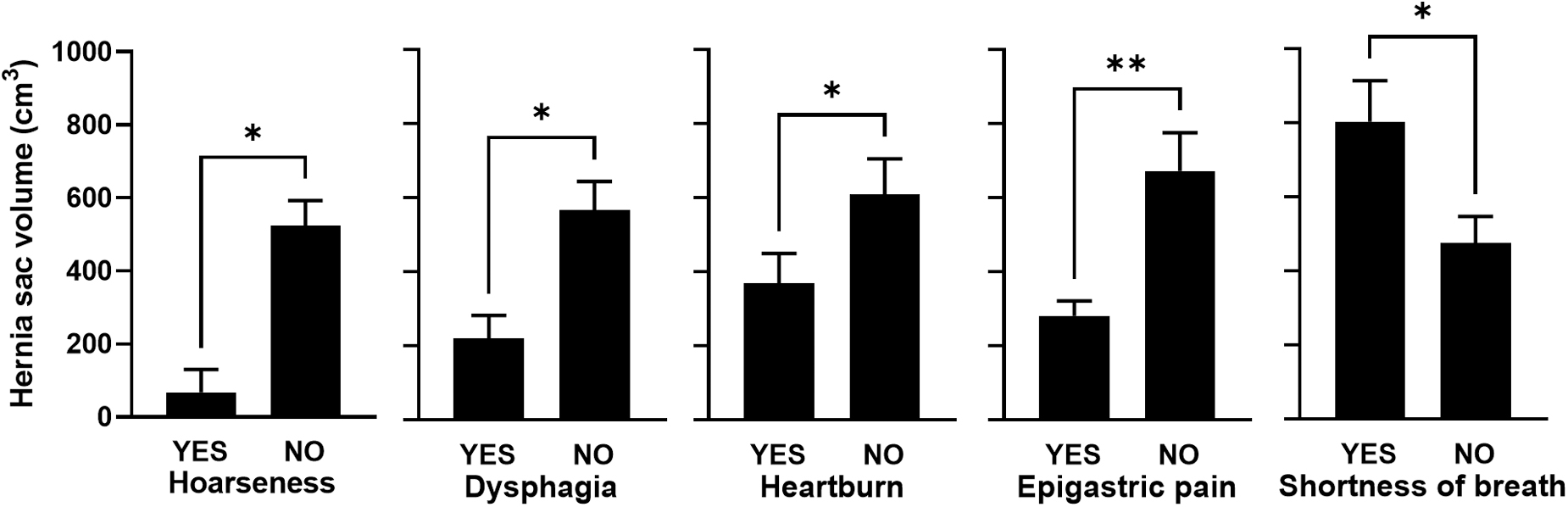
Correlation between HSV and preoperative complaints. Mann–Whitney test analysis of patients' mean ± SEM. *P < .05, **P < .005. HSV, hernia sac volume; SEM, standard error of the mean.
Correlation Between Radiological Data and Preoperative Complaints
Bold values considered significant if P < 0.05.
HDA, hiatal defect area; HSV, hernia sac volume.
A higher rate of mesh repair was found among patients with HSV >360 cm3 (Table 5) (58.6% versus 25%, P = .014). This patient group presented more frequently with incarceration (27.6% versus 4%, P = .026) and gastric volvulus (17.2% versus 0%, P < .041). Preoperative dysphagia and epigastric pain were more frequent among patients with HSV <360 cm3 compared with patients with HSV >360 cm3 (dysphagia: 29.2% versus 6.9%, P = .037; epigastric abdominal pain: 66.7% versus 20.7%, P = .001) (Table 5).
Univariate Analysis of Preoperative and Postoperative Findings by Hernia Sac Volume and Hiatal Defect Area
Bold values considered significant if P < 0.05.
GI, gastrointestinal; HDA, hiatal defect area; HSV, hernia sac volume.
Hiatal defect area
The overall mean size of HDA was 19.48 ± 14.16 cm2. Patients who presented with complaints of epigastric pain and heartburn had lower HDA compared with those who did not. Patients who presented with shortness of breath had higher mean HDA compared with those who did not (epigastric abdominal pain: 14.06 ± 8.39 versus 23.33 ± 16.16, P = .019; heartburn: 15.37 ± 11.35 versus 22.64 ± 15.42, P = .038; and shortness of breath: 28.5 ± 7.70 versus 18.54 ± 14.39, P = .031) (Table 4).
Analysis of preoperative and postoperative findings about the mean of the HDA is summarized in Table 5. Higher rates of volvulus were found among patients with HDA <25 cm2 (68.8% versus 29.7%, P = .01).
HSV and HDA as mesh repair predictors
At ROC curve analysis, the area under the curve is statistically significant (P = .003, odds ratio [OR] = 3.6), indicating that HSV can differentiate between patients who had mesh repair and those who did not. HSV values >360 cm3 have a sensitivity of 0.783 and a 1 − specificity of 0.483 for predicting mesh repair (Fig. 5A).
The ROC curve for HDA is statistically significant (at the 10% level), indicating that it is possible to differentiate between patients who had mesh repair and those who did not (P = .06). An HDA >22.8 cm2 results in a specificity of 0.719 and a 1 − specificity of 0.3 for predicting mesh repair (Fig. 5B).
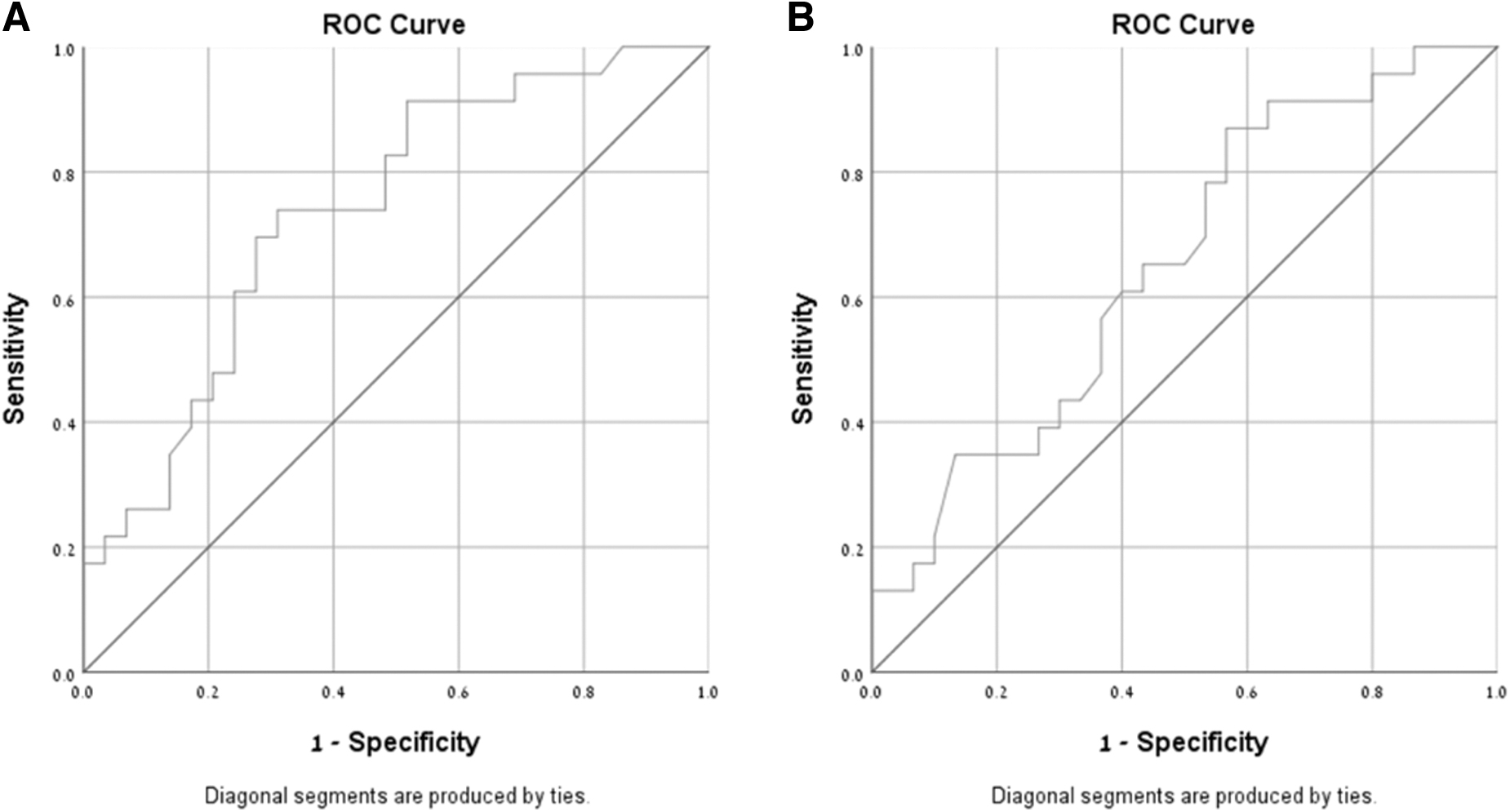
ROC curve.
In a multivariate logistic regression analysis of mesh repair (Table 6), no specific preoperative symptoms were independently associated with mesh repair.
Multivariate Analysis of Mesh Repair and Computerized Tomography Variables
Bold values considered significant if P < 0.05.
CI, confidence interval; HDA, hiatal defect area; HSV, hernia sac volume; OR, odds ratio.
Higher HSV was the only factor among the imaging measurements independently associated with mesh repair (OR = 1.036, 95% confidence interval [CI]: 1.006–1.066, P = .018).
To avoid biasing the results, which could have arisen due to the inclusion of the group that was classified with a type I hernia and did not undergo any mesh repair, the statistical analysis was also performed without the inclusion of this group.
Even when only the more complex types of hiatal hernia (II–IV, n = 46) were analyzed, HSV was associated with the use of mesh (OR = 1.031, 95% CI: 1.002–1.061, P = .039).
Discussion
Diaphragmatic hernia repair is challenging, and many surgeons prefer primary repair, avoiding potential long-term complications associated with the mesh. Mesh repair may be unavoidable, however, when repairing large hernias. Excessive tension or crural disruption has been linked to postoperative re-herniation, recurrent symptoms, and the need for revisional surgery. Hernia repairs should ideally be tension-free. However, in large defects, performing a tension-free repair in the hiatus is technically very difficult. The use of mesh repair, however, is controversial.
Unlike other hernia repair, in which the mesh passively supports the intra-abdominal viscera, any prosthetic mesh used in hiatal repair may encounter the esophagus, increasing the risk of esophageal erosion and other complications, such as severe dysphagia in cases of recurrent herniation through the mesh. Moreover, mesh repair has not been shown to reduce long-term recurrence rates. 2 However, according to some surgeons, using mesh in the hiatus is safe, and the outcome is acceptable.2,3 Significant tension over the suture lines, which can lead to early repair failure, mandates using mesh during repair in some cases.
Over the past two decades, the use of CT scans for evaluating abdominal and thoracic symptoms has increased exponentially and is frequently obtained as part of the preoperative evaluation.4,5 Few studies have shown a correlation between radiological parameters of diaphragmatic hernias and surgical outcomes. A barium esophagram or endoscopy can be used to estimate the size of a hiatal hernia, with giant hernias requiring more complex repairs.3,6–9 Recurrence has also been linked to the mean diameter of the hiatus (above 10 cm in some cases).2,10
With the increased use of high-resolution CT, as well as advances in and availability of 3D reconstruction software, new avenues of preoperative imaging research and clinical utility have emerged. 11 However, the use of volumetric analysis for surgical planning in laparoscopic surgery has remained limited, and a correlation between hiatal hernia dimensions and repair techniques has yet to be established. Using these preoperative CT imaging parameters and their ability to determine which patients can benefit from mesh repair may assist the surgeon in surgical planning and intraoperative decision-making.
HSV has been shown to predict the difficulty of hernia repair, especially when the volume is large, and the defect is wide. 12 HSV has been shown to be the main factor associated with the need for emergency surgery, with high HSV increasing the likelihood of emergency surgery.10,13 A link between HSV and re-herniation was discovered during operative measurement. 3 However, this relationship is only measured evaluatively rather than empirically. 3 HDA was also linked to the need for emergency surgery. Furthermore, HSV and HDA have been linked to hernia incarceration, volvulus, and fundoplication. 10
Failure to address tension is a leading cause of re-herniation. Diaphragmatic relaxing incisions have been described in patients with large hiatal defects who cannot be primarily repaired without significant tension over the suture line.14–16 In the repair of HH, this technique reduces hiatal tension and facilitates primary hiatal closure. 15 Therefore, it is conceivable that we demonstrated that the use of relaxing incisions is frequently performed in conjunction with the use of mesh. In these cases, the mesh can be placed over the incision and away from the esophagus.
In this study, the analysis revealed that patients with type I hernias did not have mesh repair, whereas patients with grades III and IV did. Furthermore, we found no correlation between preoperative complaints and the use of mesh, as well as the likelihood of recurrence or postoperative complications.
A review of the imaging indices revealed a correlation between mesh repair and HSV, HDA, and neck height. HSV and HDA were also associated with several preoperative complaints. Higher HSV and HDA were associated with larger hernias. Larger hernias exert less pressure on the organs within the hernia sac, which may explain why preoperative symptoms such as dysphagia, epigastric pain, and heartburn are less common. However, more pressure is applied to the organs of the chest and lungs, which can cause shortness of breath and breathing difficulties. We also found a relationship between higher HSV and chronic gastric volvulus. In these cases, it may be due to increased mobility within the hernia sac.
Regarding the significance of developing a prediction model for mesh repair based on the simulation parameters examined, we found that the two parameters HDA and HSV may predict mesh use, with HSV having a higher significance. As a result, it is possible to conclude that patients with HSV >360 and/or HDA >22.8 are more likely to require mesh repair. Furthermore, each additional 1 cm3 increase in HSV results in a 3.6% increased likelihood of requiring a mesh repair, with a 36% risk increase per 100 cm3 of HSV. These preoperative measurements can potentially aid the surgeon in intraoperative decision-making.
The study's limitations include its retrospective nature and a variable period from CT imaging to surgery. Further research is required to ascertain these results.
Conclusions
The use of CT imaging and volumetric analysis can be helpful in determining which patients might need mesh repair in the presence of large HH. HSV and HDA may be useful tools for aiding surgeons in preoperative planning and intraoperative decision-making.
Footnotes
Authors' Contributions
All authors confirm the following: study conception and design, data collection, analysis and interpretation of results, and article preparation.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.