
Abstract
Introduction:
Empyema secondary to pneumonia is a common condition. A significant number of patients will require surgical intervention for drainage and decortication. The aim of this study was to identify predictive factors for surgical intervention.
Materials and Methods:
The medical records of patients who were diagnosed with empyema secondary to pneumonia between the years 2010 and 2019 in a university hospital were included in the study. Patients who underwent surgical intervention were defined as group A and nonoperative treatment as group B. Clinical and laboratory data were collected from medical records and patients' chest computerized tomography (CT) scans were reviewed.
Results:
A total of 194 patients were included in the study—86 patients were included in group A and 108 patients in group B. Several parameters on admission were found to have a statistically significant correlation with surgical intervention: younger age, higher systolic blood pressure, and elevated white blood count. Multivariant analysis showed that younger age was found to have a statistically significant correlation with operative intervention (adjusted odds ratio = 0.971, P = .023). A statistically significant correlation between surgical intervention and survival (adjusted hazard ratio [HR] = 1.762, P = .046) and an inverse correlation between age and survival (adjusted HR = 0.050, P < .001) were found. Surgical intervention was associated with increased survival irrespective of age. A total of 42 CT scans were available for review. The mean density of the empyema fluid in group A was higher by 4.3 hounsfield units compared to group B (P < .067).
Conclusions:
Younger age was found to be associated with surgical intervention among patients suffering from empyema secondary to pneumonia. Surgical intervention was associated with increased long-term survival, irrespective of patients' age. Several radiologic characteristics were associated with the need for surgery in this study: empyema fluid density, pleural thickening, and fluid loculations. Additional prospective studies are required to ascertain these results.
Introduction
Complicated parapneumonic effusion is the most common cause of pleural empyema, with up to 20% of the cases requiring surgical intervention.1,2 Other interventions include drainage and fibrinolytics with variable success rates. 3 Several studies have tried to identify factors associated with the need for surgical intervention among this patient group with inconsistent results.4,5 The aim of this study is to identify early prognostic factors for surgical intervention among patients with parapneumonic empyema.
Materials and Methods
Institutional review board approval was obtained for this study. The records of all patients who were discharged from hospitalization with diagnosis of “empyema” between the years 2010 and 2019 in a university hospital were reviewed. Patients over 18 years with parapneumonic empyema were included in the study. Exclusion criteria included patients with thoracic empyema secondary to other reasons, patients with nonthoracic empyema, incomplete data, empyema diagnosis without diagnostic pleural fluid analysis.
The cohort was divided into two groups: group A was defined as all patients who were planned for surgical intervention, group B included all patients who were treated nonoperatively. Data collected included demographics, clinical data—vital sign upon admission, laboratory data including white blood count (WBC), C-reactive protein (CRP), fluid analysis values, nonsurgical interventions: chest drain placement, fibrinolytics instillation, length of stay, and survival during the study period. For patients who had computerized tomography (CT) available for review, the following data were collected: volume of pleural fluid, pleura thickness, pleural enhancement, air bubbles, extrapleural fat enhancement, and fluid loculations (Fig. 1). The following definitions were used:
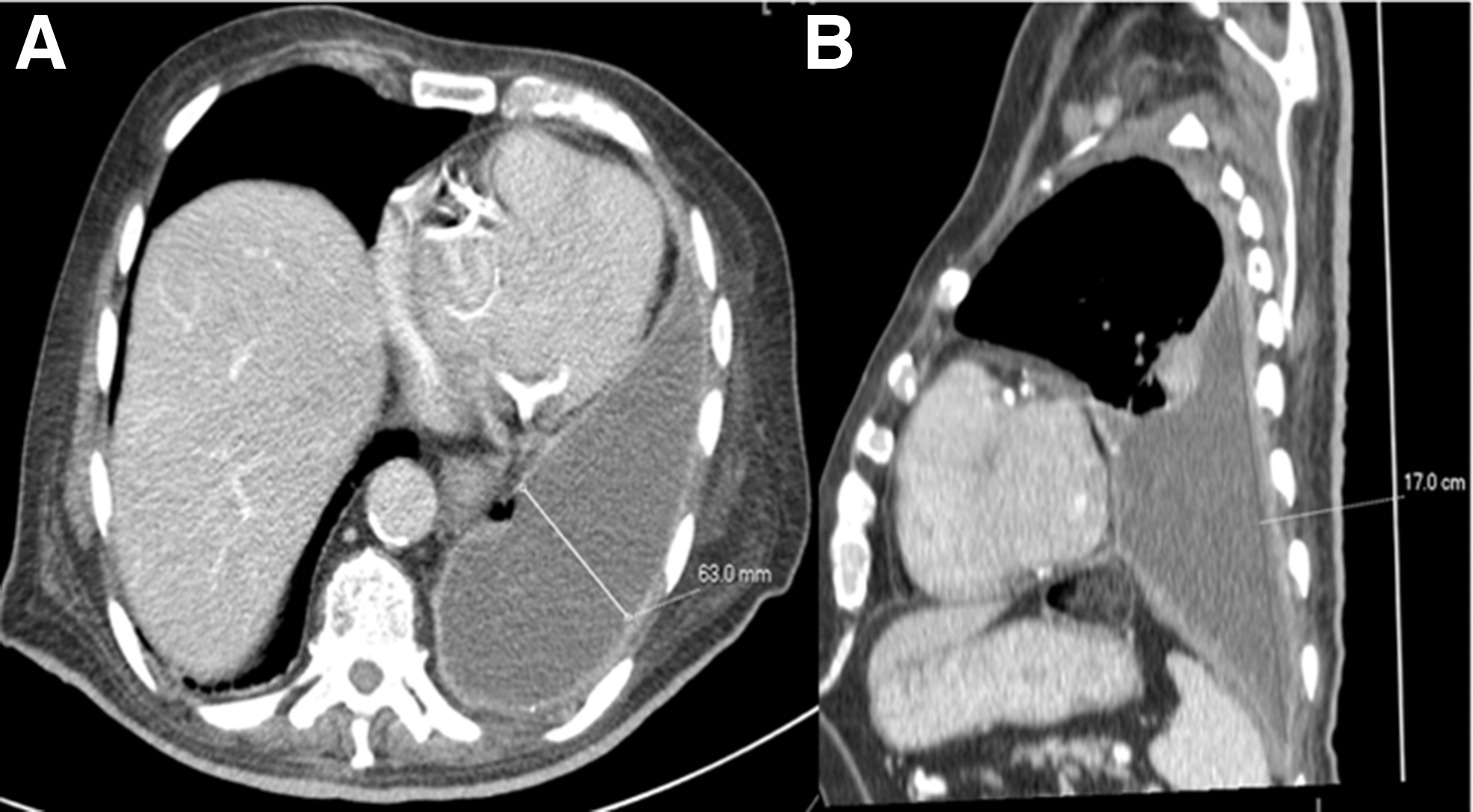
Examples of radiologic findings on chest CT of a patient suffering from pleural empyema.
Pleural fluid volume was calculated as D2*L – D that was defined as maximal fluid depth in the axial CT plane, L was defined as maximal fluid depth in the sagittal CT plane (Fig. 2).
Thickened pleura: >3 mm on an axial CT plane.
Fluid density was calculated as an average of 3 points measurement and expressed in Hounsfield units scale (HU).
Split pleural sign: thickened visceral and parietal pleura with interposing fluid.

Example of pleural fluid volume estimation in a patient suffering from pleural empyema using chest CT. An estimation of pleural fluid volume using the D2*L formula, where D is the maximal depth of the pleural fluid in the axial plane
All CT scans were performed with Philips Brilliance 64 (Eindhoven, The Netherland) CT scanner. All studies included 3 mm slices, and included only intravenous contrast contrast studies performed before any invasive intervention.
Statistical analysis
Associations between dichotomies were tested by chi square test and Fisher's Exact test. Student t-test was used to test association between paired groups. Mann–Whitney's test was used to compare nonpaired groups. Kaplan–Meier functions were constructed and differences in survival were tested by Log Rang test. The association of surgical intervention and long-term survival was tested using cox regression multivariate model. All test used were two-tailed, statistical significance was defined as P < .05.
Results
A total of 194 patients were included in the study. Of these, 86 were planned for surgical intervention (group A), and 108 were treated nonoperatively (group B). Two patients of group A declined surgery. The cohort's characteristics are listed in Table 1. The mean age of group A was lower compared to group B (52.4 versus 62.4 years, P < .001) with a lower rate of ischemic heart disease (IHD) (7% versus 30%, odds ratio [OR] = 0.34, P = .018). WBC upon admission was higher among group A comparted to group B (19K versus 16.1K, P = .05) with a slightly higher CRP levels (21.6 versus 19.4, P = non-significant). The rate of positive fluid cultures was lower among group A compared to group B (35% versus 52%, OR = 0.5, P = .019). Most patients had Gram-positive bacterial growth (53%), 17% were Gram-negative, 17% were polymicrobial, 10% were anaerobes, and 3% were fungi. No difference in organism growth was found between the groups. No difference was found between the groups in time-to-drainage. A higher rate of fibrinolysis was administered in group B, and this was borderline significant (45% versus 33%, P = .079). No difference was found among groups in regards to pleural fluid culture results (Table 2).
Comparison of Baseline Characteristics Between Study Groups
Bold value indicates statistically significant at P < 0.05.
For mean difference + or – signs precede the numeric value.
Counting from the first day of hospitalization.
BPM, beats per minute; CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; DM, diabetes mellitus; IHD, ischemic heart disease; LDH, lactate dehydrogenase; OR, odds ratio; WBC, white blood count.
Organism Growth in Cultures from Pleural Fluid Samples
ESBL, extended spectrum beta lactamase.
Admission-to-drainage time was similar between groups—3.9 ± 6.9 days for group A and 4.4 ± 5.7 days for group B (P = .59). Among group A, 84% of the patients underwent pleural drainage, 3% did not undergo any drainage, and 13% had missing data. In group B, 80% of the patients underwent pleural drainage, 5% did not undergo drainage, and 14% had missing data (P = .32). No difference was found in the average time for the initiation of fibrinolytic therapy from admission—group A—9.3 ± 12.3 days, group B—8.3 ± 7.6 days (P = .7). The rate of fibrinolytic therapy was lower among group A compared to group B (33% versus 45%). A statistically borderline association was found between fibrinolysis and nonoperative management (OR: 0.58, P = .079), but no significant statistical differences were found between the groups regarding pleural space drainage.
Among group A, 46% underwent thoracotomy and 54% underwent thoracoscopy. In-hospital mortality was lower among group A (7% versus 17%, OR = 0.35, P = .028). A higher rate of long-term survival was found among group A during the study period (88.79 versus 64.34 months, P < .001). Age was also found to be associated with longer survival (hazard ratio [HR] = 1.055, P < .001). Multivariate analysis showed that surgery conferred survival benefit regardless of age (adjusted HR = 1.762, P = .046) (Fig. 3).
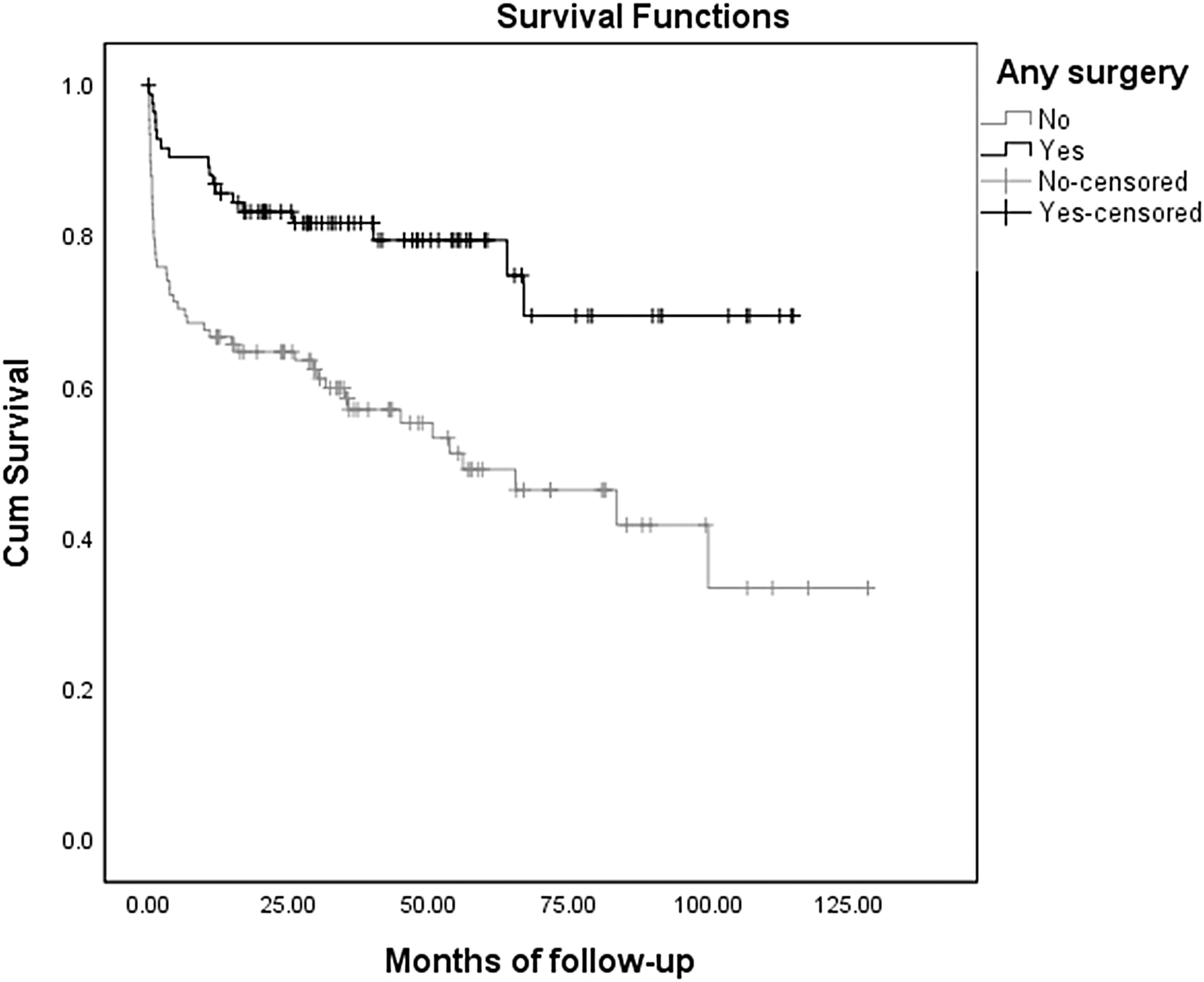
Long-term survival between groups. Kaplan–Meier survival analysis comparing survival between surgery and nonoperative groups. The X-axis represents the time in months, and the Y-axis represents the cumulative percent of patients. The mean-difference found between the two groups was 24.45 months (P < .001).
Forty-two patients had CT scan available for review which met the inclusion criteria (group A—N = 20, group B—N = 22). A trend toward a slightly higher fluid density was found among group A (15.3 versus 11.1 HU, P = .067, Table 3).
Comparison of Radiological Findings on Thoracic Computerized Tomography with Contrast Between Study Groups
For mean difference + or – signs precede the numeric value.
HU, hounsfield units.
Discussion
The purpose of this study was to identify prognostic factors for the need of surgical intervention among patients with parapneumonic empyema. Several prognostic factors were identified—lower systolic blood pressure, higher WBC levels, and a higher density of the pleural fluid per chest CT. The differences between the groups were small, although statistically significant, and their clinical significance is limited. Surgical intervention was associated with lower in-hospital mortality and a higher long-term survival. Surgical decision-making takes into account patient's age and comorbidities, and this introduces selection bias to our results—group B was older with a higher rate of IHD. It is important to mention that several studies have compared patients' age to pneumonia and empyema development and hypothesized that the inflammatory reaction may be inversely related to age. Metlay et al. 6 analyzed symptoms report among patients with pneumonia of different age groups. They found significant decreases in reported symptoms with increasing age. Kelly et al. 7 found no decrease in systemic cytokine levels among patients with community-acquired pneumonia. Falguera et al. 8 reported of several prognostic factors for the development of pleural effusion and empyema among 4715 patients with community acquired pneumonia. Of the patients who developed pleural effusion, 30% had empyema. They found that age <60 years, alcoholism, pleuritic pain, tachycardia >100/minute, and WBC >15,000/mm3 were associated with empyema development. Our results agree with most of these findings. Younger patients may develop a more aggressive disease process that may, in turn, lead to increased tendency to operate.
Several studies have attempted to identify prognostic factors for intervention among empyema patients. A meta-analysis by Heffner et al. 9 showed that pH <7.21 was associated with the need to drain a complicated pleural effusion. Kim et al. 10 found that younger age <50.5 years and shorter duration of complaints <4.5 days were independent predictive factors for the failure of medical treatment in patients with empyema. Some of these findings are in agreement with our results, indicating that younger patients may develop a more aggressive disease course.
Study limitations
This study compared retrospective results of patients with parapneumonic empyema. Younger patients were more prone to undergo surgical intervention. Due to the retrospective nature of this study, this may indicate selection bias, as the age and co-morbidities of the patients may have affected the surgical decision.
Conclusions
Younger age was found to be associated with intention to operate in patients suffering from empyema secondary to pneumonia. Surgical intervention was associated with lower in-hospital mortality and increased long-term survival, irrespective of patients' age. Additionally, several radiologic characteristics were associated with the need for surgery in a smaller group of patients in this study: empyema fluid density, pleural thickening, and fluid loculations. Additional prospective studies are required to ascertain these results.
Footnotes
Authors' Contributions
All authors confirm the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.