
Abstract
Background:
A ban on neodymium magnets was lifted by the U.S. Consumer Product Safety Commission in 2016. Pediatric gastroenterologists and surgeons were increasingly tasked with removing these problematic objects. The purpose of this study was to assess the utility of single-incision laparoscopic surgery (SILS) in the management of ingested magnets.
Patients and Methods:
This is a single-center, retrospective assessment of surgical interventions for ingested magnets. International Classification of Disease, 10th revision codes were used to identify 349 patients ≤21 years of age evaluated for foreign body ingestion over a 4.5-year period. A medical record review helped isolate 29 (8.3%) magnet ingestions, 9 requiring surgical intervention. RedCap was used for analysis.
Results:
Of 9 surgical patients, 7 underwent SILS intervention by 1 surgeon. Another surgeon performed an open operation, whereas a third performed a multiport operation. Of the 7 SILS cases, 3 were completed without conversion to open. In one of these cases, bowel resection with primary anastomosis was performed. For SILS cases, average operating room time was 109 minutes (38–170 minutes), time to enteral feeds was 23 hours (0.28–79.2 hours), and hospital length of stay (LOS) was 3.8 days (1.96–6.68 days). Thirty-day readmission for SILS was 14.3%. No other complications were observed.
Conclusions:
SILS has been safely utilized for magnet retrieval. It offers an ability to identify the affected intestinal segment and an opportunity to intervene extracorporeally through an uncapped port. In addition, knowing where matted bowel is located can direct a limited incision during conversion to laparotomy. This may confer benefits of decreased pain, shortened time to enteral feeds, and decreased hospital LOS.
Introduction
Victims of their own curiosity, children often require assessment for foreign body (FB) ingestion. Consumed items are of varied type and pose unique challenges. The focus of this article is magnets, which have become increasingly problematic. Specifically, a novel application of single-incision laparoscopic surgery (SILS) is outlined.
Neodymium or rare-earth magnets are 5–10 times more powerful than standard ferrite magnets. In these times of uncertainty and restlessness, fidgeting toys “for adults” have become increasingly popular. Manufacturers of these “toys” have embraced use of neodymium magnets, in either stand-alone form or as part of more complex devices susceptible to deconstruction.
A ban on the sale of neodymium magnets was lifted by the U.S. Consumer Product Safety Commission in 2016. After 2017, a fivefold increase in the escalation of care for multiple magnet ingestions was reported. 1 There is a growing body of literature, from both pediatric gastroenterologists and surgeons, that aims to define the problem and create standardized management algorithms. Opinions regarding urgency of intervention between physician specialties are not always aligned. The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) proposed a management algorithm that utilizes presence or absence of symptoms to decide if serial imaging can safely be utilized when multiple magnets are ingested. 2 There are surgeons who advocate for immediate intervention, regardless of symptomatology, when either multiple magnets or a magnet and another metallic object are ingested.3–5
Historically, laparotomy was offered as the necessary intervention for magnet retrieval.5,6 Laparoscopy, however, has demonstrated applicability to this problem.3,7–12 Traditional multiport (MP) laparoscopy requires enlargement of one of the port sites in the event a complex intervention, such as bowel resection, is needed. This allows for externalization and more direct interaction with the bowel. SILS has been safely applied to a variety of surgical problems. We outline cases in which we utilized this approach when multiple magnets were ingested.
Methods
A retrospective chart review was performed to identify all cases of magnetic FB ingestion requiring surgical intervention from January 2018 to July 2022. We reviewed medical records of patients 21 years of age or younger with the following International Classification of Disease, 10th revision codes: T18.2XXA, T18.3XXA, and T18.8XXA. Patient charts were reviewed to exclude cases where no magnets were ingested. Because our aim was to look at surgical patients, we further excluded those where observation and/or endoscopy alone were utilized. The individuals requiring surgical intervention were classified as open, MP, or SILS patients (Fig. 1).
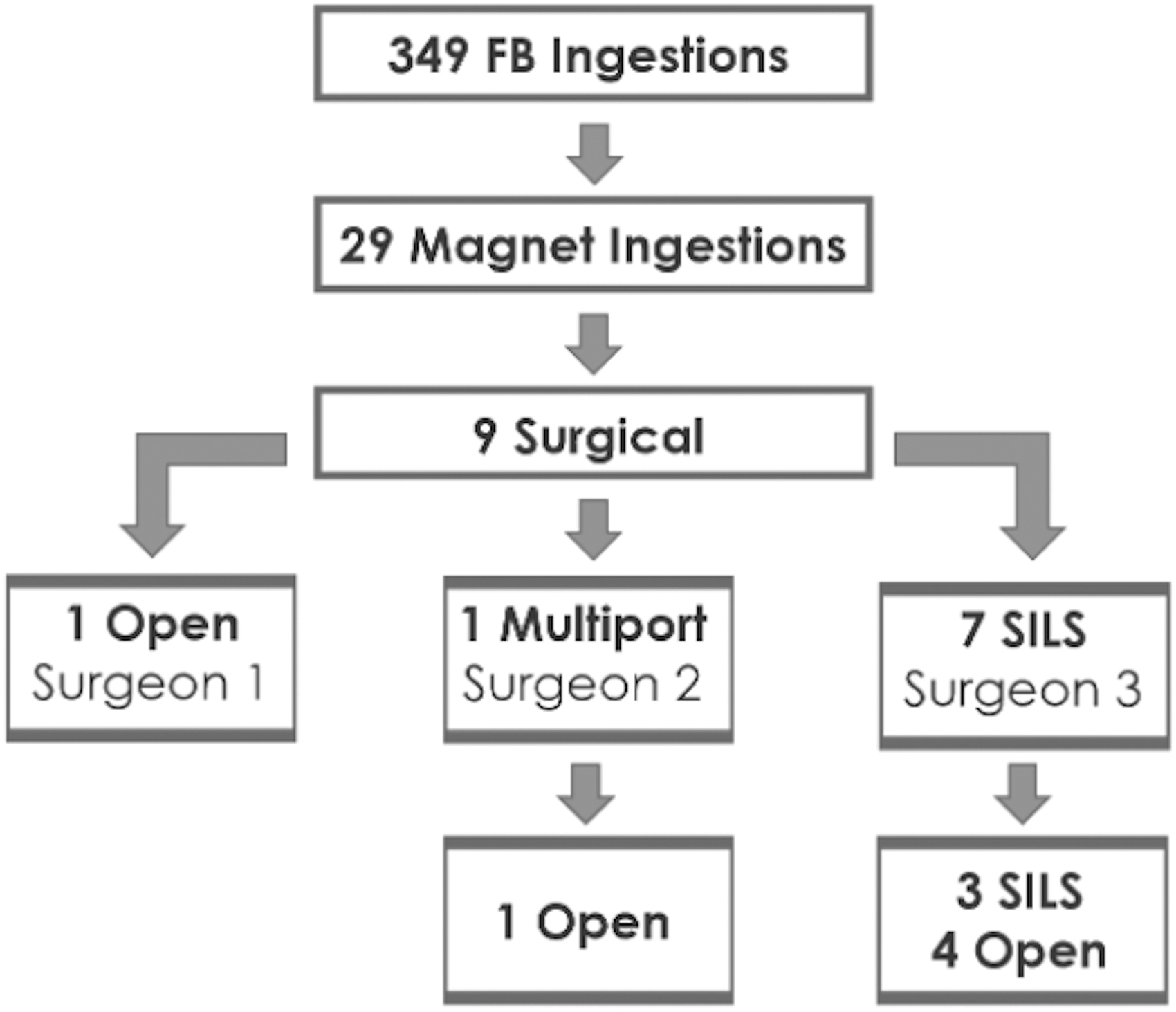
FB ingestions over 4.5 years. FB, foreign body.
Data gathered for each patient requiring surgical intervention included age, gender, neurologic status, history of prior ingestions, presence of a witness, time to presentation, presence and type of symptoms, imaging utilized, utilization of endoscopy, instances of conversion to laparotomy, number of magnets removed and presence of other metallic foreign bodies, operating room (OR) duration, time to first enteral feed postoperatively, hospital length of stay (LOS), enteric level where magnets were found, evidence of fistulation and/or perforation, requirement for and quantity of bowel resections, number of anastomoses, and length of bowel removed. This study was approved by the Orlando Health Institutional Review Board with a waiver of consent. All patient information was de-identified and maintained in a secure location. REDCap was used to process the data.
Results
During the 4.5-year study period, 349 FB ingestions were managed. Twenty-nine individual cases of magnetic FB ingestion were identified. Of these, 9 required surgical intervention. One patient, managed by the most senior partner, underwent immediate laparotomy. A second patient was managed via MP laparoscopy converted to laparotomy. The remaining 7 patients, all managed by a single surgeon, underwent SILS upfront. Three SILS cases (42.9%) did not require conversion to laparotomy. The remaining 4 (57.1%) patients required escalation to laparotomy. In 3 of these cases, magnets were found in the stomach (2) and duodenum (1). Localization required a combination of manual palpation and utilization of a sterile sleeved magnet, which could only be performed through a laparotomy. In the fourth case, 17 magnets were accompanied by a split lock washer (Fig. 2). In this case, which had the longest operative duration of the series at 170 minutes and required resection of 40 cm of small bowel, unique technical challenges could not be overcome with SILS alone.

Radiograph of 2-year-old who ingested 17 BBs and a split lock washer. BB, buckeyball.
For SILS cases, average OR duration was 109 minutes (38–170 minutes). Average time to enteral feeds in this group was 23 hours (0.28–79.2 hours), and hospital LOS was 3.8 days (1.96–6.68 days). Comparisons with laparotomy and MP procedures are given in Table 1. Thirty-day readmission for SILS was 14.3%. No wound infections or bowel obstructions were observed postoperatively.
Nine Patients Who Underwent Surgical Retrieval of Ingested Magnets
BB, buckeyball; LOS, length of stay; MP, multiport; OR, operating room; SILS, single-incision laparoscopic surgery.
Case 1
An asymptomatic 10-year-old boy was transferred onto the pediatric gastroenterology service after he reported disassembling and ingesting magnets removed from a fidgeting toy. Radiographically, these were 2.5 mm in diameter and were connected in the left upper quadrant. These were felt to be in the descending colon but were later noted to be hung up in the right lower quadrant. Pediatric surgery was consulted on the second hospital day. Given the size of these magnets and their persistence in the right lower quadrant, suspicion existed for their retention in the lumen of the appendix. He was taken to the OR for SILS, where this was confirmed when the appendix was noted to be attracted to the laparoscopic instruments. An SILS appendectomy was performed, effectively removing the five magnets (Fig. 3).

Appendix and chain of 2.5 mm intraluminal “Speks” removed from a 10-year-old male via SILS appendectomy. SILS, single-incision laparoscopic surgery.
Case 2
A 7-year-old girl was observed ingesting FBs. She was asymptomatic and presented 1.5 hours after the witnessed event. Radiographically, two buckeyball (BB) magnets were noted to be attached in the left upper quadrant. Pediatric gastroenterology, suspecting these were in the stomach, took her for endoscopic retrieval. No magnets were found in the stomach and an intraoperative consultation was made to pediatric surgery. An SILS assessment of the bowel was undertaken, during which no FBs could be found. The surgeon elected to extend his umbilical incision cephalad, and the magnets were ultimately found within the stomach. They were removed through a small gastrotomy.
Case 3
A 2-year-old girl was observed ingesting FBs. She was asymptomatic. Both pediatric gastroenterology and surgery were consulted after BBs and a coin were noted radiographically. The coin was suspected to be within the stomach but there were six BBs elsewhere. She was brought to the OR for SILS assessment, during which two magnets could be removed from the ileum. The remaining four magnets could not be found and conversion to laparotomy occurred. They were found within and removed from the third portion of the duodenum. No bowel resection was required. The intragastric coin was left to pass spontaneously, which it did not do and required take-back for endoscopic retrieval.
Case 4
A 2-year-old boy was observed ingesting FBs the evening before presentation. He was brought in when he developed abdominal pain and started vomiting. Three BBs were noted radiographically. He was brought to the OR, where SILS collection of the magnets from the ileum was performed (Fig. 4). Conversion to open was not required.

Externalized loops of fistulized bowel containing 5 mm “buckeyballs.”
Case 5
A crying 2-year-old boy presented with abdominal pain. Radiographically, numerous BBs were visualized. He was brought to the OR for SILS assessment. The jejunum was noted to be adherent to the transverse mesocolon, which was in turn adherent to the stomach. Conversion to laparotomy was deemed necessary, and the umbilical incision was extended in a cephalad direction. Fistulation between the posterior wall of the stomach and jejunum was noted, along with numerous other jejunal injuries requiring a 40 cm resection. After removing all 16 BBs, the gastrotomy was closed primarily. While his immediate postoperative course was uncomplicated, he developed significant oral aversion and the gastroenterology service placed a gastrostomy tube endoscopically.
Case 6
A 3-year-old girl presented with abdominal pain. Imaging revealed a centrally located ring of beads. Ingestion had been unwitnessed, and her parents did not feel these could be magnets. Pediatric gastroenterology admitted her and administered Golytely while monitoring radiographically for migration. When not observed, pediatric surgery was consulted. She was brought to the OR for SILS assessment. She was found to have a Meckel's diverticulum and matted jejunum. Twenty-two BBs were removed through an uncapped SILS port, after which an extracorporeal assessment and resection (7 cm) of the bowel was performed. No conversion to laparotomy was required. After primary anastomosis, the jejunum was returned to the abdominal cavity and a Meckel's diverticulectomy was performed.
Case 7
A 2-year-old girl presented with abdominal pain and vomiting. Radiographically, numerous BBs and a washer were visualized (Fig. 2). Pediatric gastroenterology was consulted, and a colonoscopy was performed. The foreign bodies were not found, and pediatric surgery was contacted. SILS assessment was performed. Numerous loops of bowel were matted and, after considerable time trying to proceed laparoscopically, the surgeon elected to convert to laparotomy. While removing the foreign bodies, three jejunal enterotomies were repaired primarily. There were numerous enterotomies in the ileum and intestinal resection was deemed necessary. A 40 cm segment of ileum was resected and a primary anastomosis performed. A split lock washer and 17 BBs were removed.
Case 8
An 8-year-old boy presented with abdominal pain and vomiting. BBs were visualized radiographically. He was brought to the OR, where a laparotomy was performed. Nine BBs had created three fistulas. These involved the cecum, adjacent to the base of the appendix, and the small bowel. No bowel resection was necessary, but the appendix was removed.
Case 9
A 12-year-old boy presented with abdominal pain and decreased appetite. BBs were noted radiographically, and he was brought to the OR for MP laparoscopy. Small bowel was noted to be configured in a hairpin. The umbilical incision was extended, and the surgeon proceeded with what they described as a “mini laparotomy.” Five BBs were removed, and the hairpin (14 cm) was resected.
Discussion
Opportunities for utilization of SILS in pediatric surgery are abundant and varied. The technique has been routinely applied by some to appendectomy, cholecystectomy, splenectomy, ovarian detorsion, and other straightforward procedures. Ingestion of multiple magnets by children, however, poses unique challenges. This article outlines one hospital's experience with the addition of SILS to the armamentarium used for magnet retrieval.
An SILS port helps overcome limitations innate to the more recently utilized MP laparoscopy, which requires conversion to laparotomy for extracorporeal manipulation of and interventions on the bowel. Through an uncapped SILS port, which has a built-in wound protector, affected loops of bowel can be delivered. This technique has been utilized in our patient population for magnet retrieval, closure of resultant fistulas and enterotomies, and even bowel resection with anastomosis. Use of SILS is not being proposed as a replacement for laparotomy, which has a role in certain instances, but rather is being offered as a starting point with escalation if needed.
This report is the first to describe application of SILS to the problem of magnet retrieval after ingestion. Although the population size reported is small, an objective of reporting is to begin speaking about the ability to apply this technique without added patient risk. In fact, decreased procedural invasiveness might encourage practitioners to abandon the practice of watchful waiting in favor of expedited surgical retrieval once multiple magnets or a magnet and a metallic FB have passed the pylorus. Reducing duration of magnet interaction through bowel loops may limit tissue trauma and decrease morbidity.
Following placement of an SILS port at the umbilicus, a global survey of the abdominal cavity is performed. A methodical approach is then taken to ensure the entirety of the mobile midgut is inspected and that matted bowel is localized to either the supraumbilical or infraumbilical regions, which helps guide direction and limit size of an incision when conversion to laparotomy is deemed necessary. The cecum, which usually has retroperitoneal attachments, is first inspected. The terminal ileum is identified at its confluence with the cecum and is run retrograde. Once matted bowel is identified, atraumatic laparoscopic graspers are gently locked onto the individual bowel loops and the abdomen is desufflated. The SILS port is uncapped and the graspers are used to bring the bowel loops up to its opening so that the graspers can be replaced with Babcock clamps.
If unable to bring the bowel up to the SILS port, which occurs when magnets are within the stomach and retroperitoneal structures, conversion to laparotomy is considered. If able to secure the bowel at the mouth of the SILS port, magnets can be withdrawn and resultant fistulas and enterotomies may be closed in a simple manner. When intestinal involvement is extensive, bowel can typically be delivered through the uncapped SILS port once intraluminal magnets have been withdrawn. After doing so, bowel resection with primary anastomosis may be performed extracorporeally if deemed necessary. A cautionary must be issued for the need to be generous with the fascial incision at the time of SILS port placement and to monitor for progression of bowel wall edema while creating the anastomosis, as this may make returning the bowel safely to the abdominal cavity a challenge.
After every intervention at the mouth of the SILS port, the bowel is inspected laparoscopically in a retrograde manner from the ileocecal valve. In doing so, missed injuries may be avoided and repair sites inspected. This process is repeated as necessary until the small bowel has been run from the terminal ileum to the Ligament of Treitz and all radiographically identified magnets are removed. If all magnets are not accounted for or there is significant concern for involvement of the stomach or retroperitoneal structures, conversion to an open procedure is considered.
In conclusion, SILS can be safely added to an armamentarium used to retrieve ingested magnets. Our study population was small, so it is difficult for comparisons among surgical approaches to be made. Average operative duration, time to initial feed, and hospital LOS all seem to be acceptable when SILS is utilized. It is the hope of the authors that this study will stimulate conversation about and an interest in this novel approach to magnet retrieval. Through more frequent application of SILS to this problem, multicenter prospective studies may be performed.
Footnotes
Acknowledgments
The authors thank Drs. Donald Plumley and Brenna Fullerton, whose patients are reported in this article. Alexandra Kirkland, RN (Manager of Quality, Process Improvement, and Patient Safety) and Jill Dykstra-Nykanen, RN (Director of Quality) are both greatly appreciated for their help in navigating Red Caps at Arnold Palmer Hospital.
Authors' Contributions
S.A.: Investigation, writing—review and editing. L.W.: Investigation, writing—review and editing. E.U.: Investigation, writing—review and editing. J.F.: Investigation, project administration, writing—review and editing. J.B.: writing—review and editing, Supervision. A.S.: Conceptualization, investigation, writing—original draft, visualization, supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.