
Abstract
Background:
Despite single-incision laparoscopic surgery (SILS) being a standard procedure, its main shortcomings include narrow operating space and instrument collisions. Although the proposal of single-incision plus one-port laparoscopic surgery (SILS + 1) reduces the operational difficulty, laparoscopic pancreaticoduodenectomy (LPD) involves complex digestive tract resection and anastomosis. To reduce the number of incisions while ensuring the quality of LPD, we propose a single-incision plus two ports LPD (SILPD + 2) procedure wherein a surgeon uses two trocars with a traditional layout while the assistant and scope assistant conduct subumbilical incision.
Methods:
Retrospective analysis was performed of the perioperative data of 64 patients who underwent total LPD at our department from January to June 2023, including their age, gender, surgical operation time, estimated bleeding loss, and postoperative complications. Based on the number of inserted trocars, the patients were assigned to the conventional LPD (CLPD) group (n = 55) with five incisions and the new SILPD + 2 group (n = 9).
Results:
A total of 64 patients were included in this study, including 55 in the CLPD group and 9 in the SILPD + 2 group. The SILPD + 2 group patients had lower age and body mass index when compared to the CLPD group patients, albeit there was no statistical significance. In both groups of patients, laparoscopic surgery was completed. Regarding the operation time, estimated blood loss, and intraoperative blood transfusion, the SILPD + 2 group showed no significant disadvantage.
Conclusion:
When compared to CLPD, SILPD + 2 reduced the surgical difficulty by reducing incisions, and there was no significant difference in the short-term prognosis outcomes.
Introduction
With the popularization of the concept of enhanced recovery after surgery 1 and the increasing demand for cosmetic results, some researchers have recommended single-incision laparoscopic surgery (SILS) as an extension of conventional laparoscopic surgery.2,3 However, due to the challenging nature of the procedure and the prolonged operation time, researchers4–7 have successively introduced single-incision plus one-port laparoscopic surgery (SILS + 1) as an improvement, which includes single-incision plus one-port laparoscopic pancreaticoduodenectomy (SILPD + 1). 8
Laparoscopic pancreaticoduodenectomy (LPD), considered one of the most complex surgeries in general surgery, involves intricate digestive tract resection and reconstruction. In our pursuit of ensuring the quality of pancreatojejunostomy (PJ) and hepaticojejunostomy, our team attempted a new approach known as single-incision plus two ports LPD (SILPD + 2), building upon the foundation of SILPD + 1. This report outlines our current findings.
Methods
A retrospective analysis was conducted on the clinical data of 64 patients who underwent LPD at the Hepatobiliary Department of the Second Hospital of Hebei Medical University from January 2023 to June 2023. The patients were divided into two groups: the SILPD + 2 group (n = 9) and the conventional LPD (CLPD) group (n = 55). We collected and analyzed general patient information, including sex, age, body mass index (BMI), surgical characteristics such as operation time, and estimated blood loss. Postoperative indicators, including postoperative length of stay, drainage tube retention time, and complications, were also assessed. All patients signed the informed consent before surgery.
The inclusion criteria were as follows
Patients who could tolerate surgery without signs of distant metastasis on preoperative examination.
Patients aged 15–85 years.
Patients with a BMI of >28 kg/m2 or aged >75 years were included in the CLPD group.
The exclusion criteria were as follows: Patients with intraoperatively detected distant metastasis or those requiring conversion to laparotomy were excluded.
Preoperative preparation
Computed tomography or magnetic resonance imaging scans were performed to confirm the presence of tumors in the pancreatic head, distal common bile duct, or around the ampulla. If necessary, positron emission tomography/computed tomography scans were conducted to exclude distant metastasis.
Correction of any abnormalities in the heart, lung, kidney function, anemia, or hypoproteinemia was done.
Patients with severe obstructive jaundice were treated with either percutaneous transhepatic cholangial drainage (PTCD) or endoscopic nasobiliary drainage (ENBD).
Surgical process
Surgeons in both groups positioned themselves on the right side of the patient, with the assistant and scope assistant on the left side and between the patient’s legs (Fig. 1). In the CLPD group, trocars were arranged according to traditional laparoscopic methods, with a 10-mm trocar below the umbilicus as the observation trocar and the remaining four trocars approximately centered around the observation trocar, forming a V-shaped pattern along the front line of the armpits and the midline of the clavicle on both sides. The SILPD + 2 group used a single incision under the umbilicus as the observation and scope assistant trocar, and the two operational incisions on the surgeon’s side were in the exact location as those in the CLPD group (Fig. 2).

Position of surgeons in single-incision plus two ports laparoscopic pancreaticoduodenectomy.

Distribution of surgical incisions in single-incision plus two ports laparoscopic pancreaticoduodenectomy.
The surgical procedures for both groups were identical. A preliminary exploration of the abdominal metastasis was performed to confirm the absence of metastatic lesions. The gastrocolic ligament was transected, and the duodenum and pancreatic head were freed using the Kocher technique. After checking the involvement of the mesenteric vessels, radical resection was performed. Subsequently, the hilar lymph nodes were cleared, and the gastroduodenal artery, right gastric artery, and gallbladder artery were sequentially resected. Finally, the pancreatic uncinate process and common hepatic duct were transected, and the gallbladder was removed. After specimen resection, digestive tract reconstruction was done using the Child method, followed by PJ, biliary-enteric anastomosis, and gastrointestinal anastomosis. PJ was performed using Hong’s single-stitch technique, 9 which involves inserting a pancreatic fluid drainage tube and performing duct-to-mucosa PJ. Continuous anastomosis of the anterior and posterior walls of the bile duct was performed for hepaticojejunostomy. Endoscopic linear cutters were used for gastrojejunostomy. The drainage tubes were placed at the upper and lower edges of the PJ postoperative.
The traditional laparoscopic instruments are still used in SILPD + 2 (Fig. 3), and the new device involved is a single-port device for disposal through a subumbilical incision (Fig. 4). Due to the small diameter of the trocar used by the assistant, auxiliary devices such as biological clips, needles, and endoscopic linear cutters are all inserted through a 12 mm trocar on the surgeon’s side to avoid lens shake. When cleaning the NO. 12, removing the pancreatic head, and performing other procedures in the right abdominal surgical area, the scope assistant should stand on the left side of the patient. For operations involving gastric cutting, gastric-intestinal anastomosis, and other procedures in the left abdominal surgical area, the scope assistant should stand on the right side of the patient between the surgeon and the assistant. There is no significant difference in the role played by assistants in the two surgeries. Most of the time, assistants stand between the patient’s legs to assist in important steps such as exposing the surgical area, using suction devices to clean up blood accumulation in the surgical area, or pulling sutures.

Traditional laparoscopic instruments used in single-incision plus two ports laparoscopic pancreaticoduodenectomy.
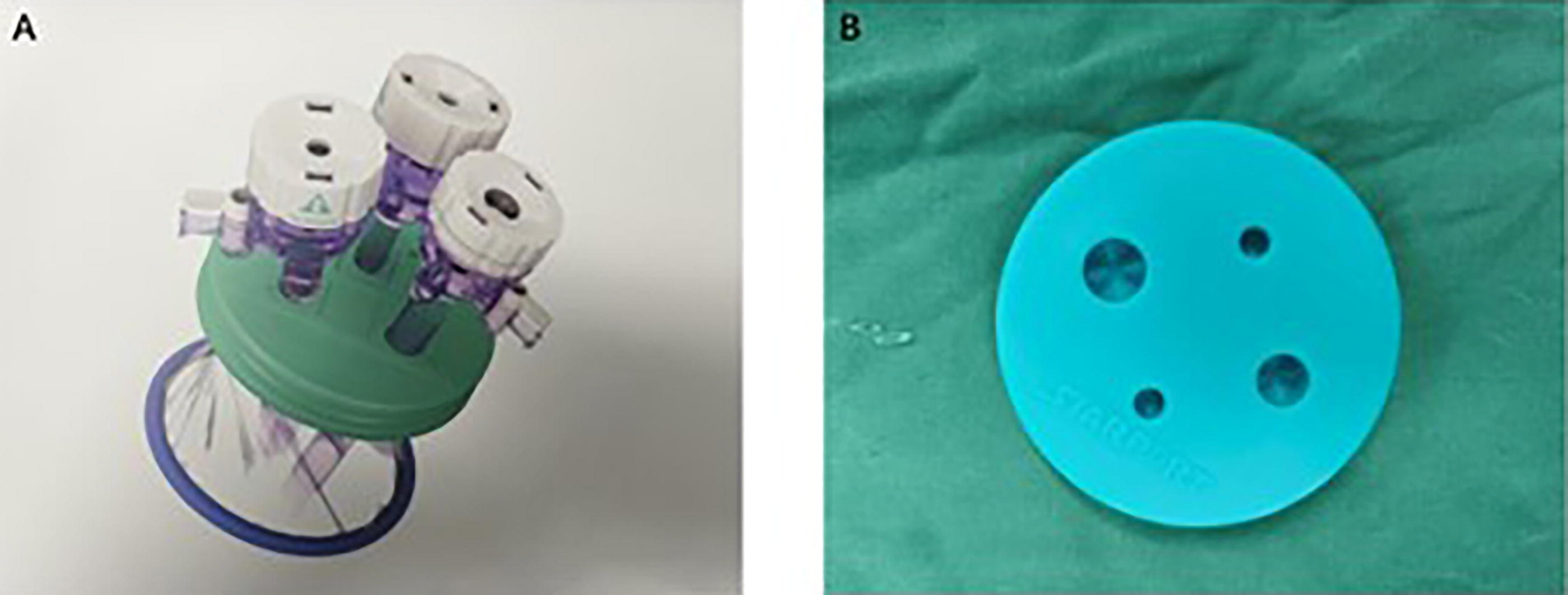
A. Trocars distribution B. Subumbilical incision device.
Postoperative management
In addition to routine treatments such as fluid replacement, acid suppression, and anti-infection measures, patients received somatostatin treatment for five days. If necessary, somatostatin treatment continued until the amylase level in the drainage fluid dropped below 5000 U/L. Postoperative pancreatic fistula was classified according to the 2016 update of the International Study Group 10 definition and grading. On the third day postoperatively, gastric tubes were removed based on gastric juice drainage volume and gastrointestinal function recovery. Starting from the fifth day postoperatively, the abdominal drainage tubes were gradually removed based on drainage volume and amylase levels in the drainage fluid.
Statistical analysis
Data analysis was performed using SPSS 26.0. Normally distributed measurement data were expressed as mean differences ± standard deviation (
Results
In this study, 64 patients were included, with 55 in the CLPD group and 9 in the SILPD + 2 group (Table 1). Although the SILPD + 2 group had a lower average age and BMI than the CLPD group, these differences did not reach statistical significance. In the CLPD group, 15 patients underwent either PTCD or ENBD, whereas only two patients in the SILPD + 2 group underwent these procedures. Both groups of patients successfully underwent the laparoscopic surgeries (Table 2). Regarding operation time, estimated blood loss, and intraoperative blood transfusion, the SILPD + 2 group did not demonstrate any significant disadvantages. The complication rates of pancreatic fistula and biliary fistula in the SILPD + 2 group were comparable to those in the CLPD group (Table 3). Except for one patient in the CLPD group who passed away after reoperation due to postoperative bleeding of the gastroduodenal artery stump, there were no other perioperative deaths in this study.
Preoperative Characteristics
ALB, albumin; ASA, American Society of Anesthesiologists Classification; BMI, body mass index; CLPD, conventional laparoscopic pancreaticoduodenectomy; ENBD, endoscopic nasobiliary drainage; PTCD, percutaneous transhepatic cholangial drainage; SILPD + 2, single-incision plus two ports laparoscopic pancreaticoduodenectomy.
Intraoperative Indicators
CLPD, conventional laparoscopic pancreaticoduodenectomy; MPD, main pancreatic duct; SILPD + 2, single-incision plus two ports laparoscopic pancreaticoduodenectomy.
Postoperative Characteristics
CLPD, conventional laparoscopic pancreaticoduodenectomy; DGE, delayed gastric emptying; SILPD + 2, single-incision plus two ports laparoscopic pancreaticoduodenectomy.
Discussion
LPD is considered a cornerstone procedure for treating tumors in the pancreatic head, distal common bile duct, and periampulla. Compared with open pancreaticoduodenectomy (OPD), LPD, with its smaller incision, offers advantages such as rapid postoperative recovery and shorter length of stay.11,12 To reduce postoperative pain and enhance cosmetic outcomes, both gynecological and thoracic surgeries have used SILS,2,3 and SILPD has also garnered some attention.13,14 Nevertheless, the constrained operative space, collision of surgical instruments, and prolonged operation time have posed challenges to LPD.
The proposal and application of SILS + 1
SILS involves fewer trocars than conventional laparoscopic surgery, resulting in a reduced availability of instruments. As a novel approach to treating gastrointestinal malignant tumors,15,16 SILS has been used in distal pancreatectomy and radical resection of sigmoid colon cancer.17,18 Numerous studies6,19 have demonstrated that SILS + 1 yields reliable short-term outcomes compared with traditional laparoscopic surgery. A study on SILS + 1 for myomectomy 20 even indicated that, in contrast to SILS, SILS + 1 significantly reduces operation time without statistically significant differences in postoperative complications. Furthermore, SILS + 1 is believed to shorten the learning curve for SILS. When dealing with complex LPD, some researchers have proposed the technique of SILPD + 1. Cai’s research showcased that SILPD + 1 significantly reduces operation time compared with CLPD while maintaining a similar postoperative complication rate. Leveraging the additional trocar, their surgical team successfully implemented SILPD + 1, even incorporating vascular resection and reconstruction. This further underscores how increased incisions can alleviate surgical complexity.
Our center’s exploration and improvement of SILPD + 1
Despite the advantages of SILPD + 1 in reducing some of the shortcomings of SILS, our center encountered certain limitations during its initial implementation:
Increased laparoscope shaking amplitude when surgeons operated with their right hand
Extensive instrument movement during procedures such as PJ, hepaticojejunostomy, and gastrojejunostomy leads to collisions of instruments and limited maneuverability.
When withdrawn from the right single incision after SILPD+1, the drainage tubes were overcrowded and prone to leakage, complicating postoperative management.
To ensure high-quality hepaticojejunostomy and PJ, optimize abdominal fluid drainage, and mitigate the risk of postoperative complications, our team attempted a new approach, SILPD + 2. In this technique, the assistant and scope assistant use the subumbilical incision for specimen extraction. In contrast, the surgeon uses two independent trocars on the right side of the patient, positioned similar to CLPD.
Compared with CLPD, SILPD + 2 reduces the number of incisions on the assistant side, thereby minimizing postoperative pain and the variability associated with different assistants, but also does not disrupt the operating surgeon’s established habits from traditional laparoscopic surgery. Additionally, SILPD + 2 enables the placement of drainage tubes horizontally along the upper and lower edges of PJ, similar to CLPD. The drainage tubes inserted through the two incisions on the surgeon’s side effectively drain the abdominal fluid, reducing the risk of abdominal infection, biliary fistula, or pancreatic fistula resulting from fluid accumulation. The improved accessibility for suturing and the use of endoscopic linear cutters further enhance the smoothness of the operation and reduce the vibration and shaking of the laparoscope. The increased surgical space for suturing is also conducive to the swift and high-quality completion of digestive tract reconstruction.
Difficulties encountered during surgery and solution
The difficulties encountered in the new surgical technique are mostly caused by the change in the position of the assistant. After the original operation trocars on the left side of the patient were canceled, our team began to search for new positions for assistants. This process extended the surgical time. Afterward, it was determined that the assistant should stand between the patient’s legs, and the scope assistant should choose a new layout to stand on both sides of the patient according to the different operating areas of the surgeon.
Under the premise of ensuring the sufficient and stable vision, the subumbilical incision results in limited operating space for the assistant, which reduces the auxiliary role of the operator compared to LPD. Moreover, the scope and the assistant’s instruments are inserted into the abdominal cavity through a single-incision device beneath the navel. However, there can be significant problems with insufficient space between the instruments, resulting in frequent collisions and a chopstick-like effect. To address this issue, we have opted to utilize a 3D laparoscopic lens with a rotating head, which allows it to avoid coming into contact with other instruments. And the assistant uses as many suction devices as possible to complete the exposure of the surgical area and the removal of fluid, reducing the collision caused by switching instruments.
The most dangerous step in the entire specimen resection process is the separation between the pancreatic uncinate and the portal vein. The assistant standing in the foot position with a suction device in the right hand can complete the exposure of the pancreas and portal vein and the extraction of fluid in the gap in a straight direction. This is more convenient than the traditional left-side position of the assistant. When performing complex procedures such as cleaning lymph nodes NO. 12 or PJ, although the assistant can complete the task of pulling tissues and sutures, it is still not safe to handle situations such as difficult anastomosis due to the thin diameter of the pancreatic duct, difficult separation due to severe tissue adhesion, or vascular bleeding, which can increase the operation time and risk. This still requires the surgical team to improve the quality of surgical completion.
Limitations
Nonetheless, our study has certain limitations, including a small sample size in the SILPD + 2 group and its retrospective nature. Larger-scale studies are warranted further to validate the safety and efficacy of this approach. Additionally, patient selection was not randomized, with a bias toward younger patients with a lower BMI in the SILPD + 2 group. Although some single-port surgeries use flexible single-port laparoscopic instruments to solve sword fighting problems, due to economic constraints, this equipment was not used during the initial stage of SLPD + 2 in our center.
Conclusion
Compared to CLPD, SILPD + 2 reduces surgical complexity while minimizing incisions, with no significant differences observed in short-term prognostic outcomes. Future large-scale studies are needed for further validation.
Footnotes
Authors’ Contributions
Z.X. and X.L. were responsible for data collection and organization. J.L. was responsible for the interpretation of imaging data. The other authors participated in the surgery. The authors have all read and approved this final article.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.