
Abstract
Background:
Laparoscopic gastrectomy for gastric cancer has become widespread as minimally invasive surgical treatment, but use of laparoscopic total gastrectomy (LTG) remains limited because of the technical difficulty and complexity of lymphadenectomy at the splenic hilum. Surgical techniques and initial experiences with the surgical approach to the upper side of the gastrosplenic ligament during LTG are introduced.
Materials and Methods:
Between January 2019 and December 2022, 57 patients with proximal gastric cancer underwent LTG using this approach.
Results:
Regarding the extent of lymphadenectomy, D1+, D2, spleen-preserving D2 + 10, and D2 + 10 with splenectomy were performed in 31, 18, 4, and 4 patients, respectively. Operative time was 341 (192–724) minutes, and estimated blood loss was 30 (0–515) g. There were no conversions to laparotomy and no postoperative complications of Clavien–Dindo grade ≥III.
Conclusions:
The present procedure is safe and feasible and provides an excellent operative view at the splenic hilum, making it easier to determine exactly the extent of lymphadenectomy in accordance with cancer progression
Introduction
Recently, laparoscopic gastric surgery has been more widely performed as an optional treatment modality for patients with gastric cancer, especially in Asian countries that have high incidences of gastric cancer.1,2 Many studies have already reported the safety and efficacy of laparoscopic gastric surgery for gastric cancer.3–5 However, the use of laparoscopic total gastrectomy (LTG) remains limited because of the high technical demands of splenic hilar lymphadenectomy and esophagojejunostomy. Because of the complexity of the vascular anatomy at the splenic hilum, splenic hilar lymphadenectomy is technically challenging even for skilled surgeons.6,7
In accordance with the 5th Japanese Gastric Cancer Treatment Guidelines, dissection of splenic hilar lymph nodes (LNs) with or without splenectomy is not included in the definition of standard-D2 lymphadenectomy during total gastrectomy and could be considered extended lymphadenectomy exceeding D2 for advanced proximal gastric cancer with the greater curvature invasion. 8 Then, it is necessary to determine exactly the extent of lymphadenectomy (D1+, D2, D2 + 10) at the splenic hilum according to cancer progression.
In this study, the technical details and our initial experience with the surgical approach to the upper side of the gastrosplenic ligament during LTG for proximal gastric cancer are reported.
Materials and Methods
Patients
Between January 2019 and December 2022, 57 (31 male, 26 female) patients with proximal gastric cancer underwent LTG using a surgical approach to the upper side of the gastrosplenic ligament in our institution. The tumor stage was defined in accordance with the 15th Japanese classification of gastric carcinoma. 9 Radical lymphadenectomy was performed in accordance with the 5th Japanese Gastric Cancer Treatment Guidelines. 8 D1+ lymphadenectomy was performed in patients with early proximal gastric cancer (cT1). D2 lymphadenectomy was performed in patients with advanced proximal gastric cancer (≥cT2) without greater curvature invasion. Spleen-preserving D2 + 10 lymphadenectomy was performed in patients with advanced gastric cancer (≥cT2) invading the greater curvature and without splenic hilar LN metastasis, whereas D2 + 10 lymphadenectomy with splenectomy was performed in patients with splenic hilar LN metastasis.
There were no patients receiving preoperative chemotherapy in this series. This study was ethically approved by the Institutional Review Board of Ishikawa Prefectural Central Hospital in Japan (No. 2225). Written informed consent was obtained from all study participants.
Surgical procedures
Patient positioning
The patient was placed in the supine position with a 12° head-up tilt and the legs apart. Five trocars were placed in the upper abdomen and 10 mmHg carbon dioxide pneumoperitoneum was induced (Fig. 1). The surgeon stood on the right side of the patient, with the assistant surgeon on the left side and the camera operator between the patient's legs.
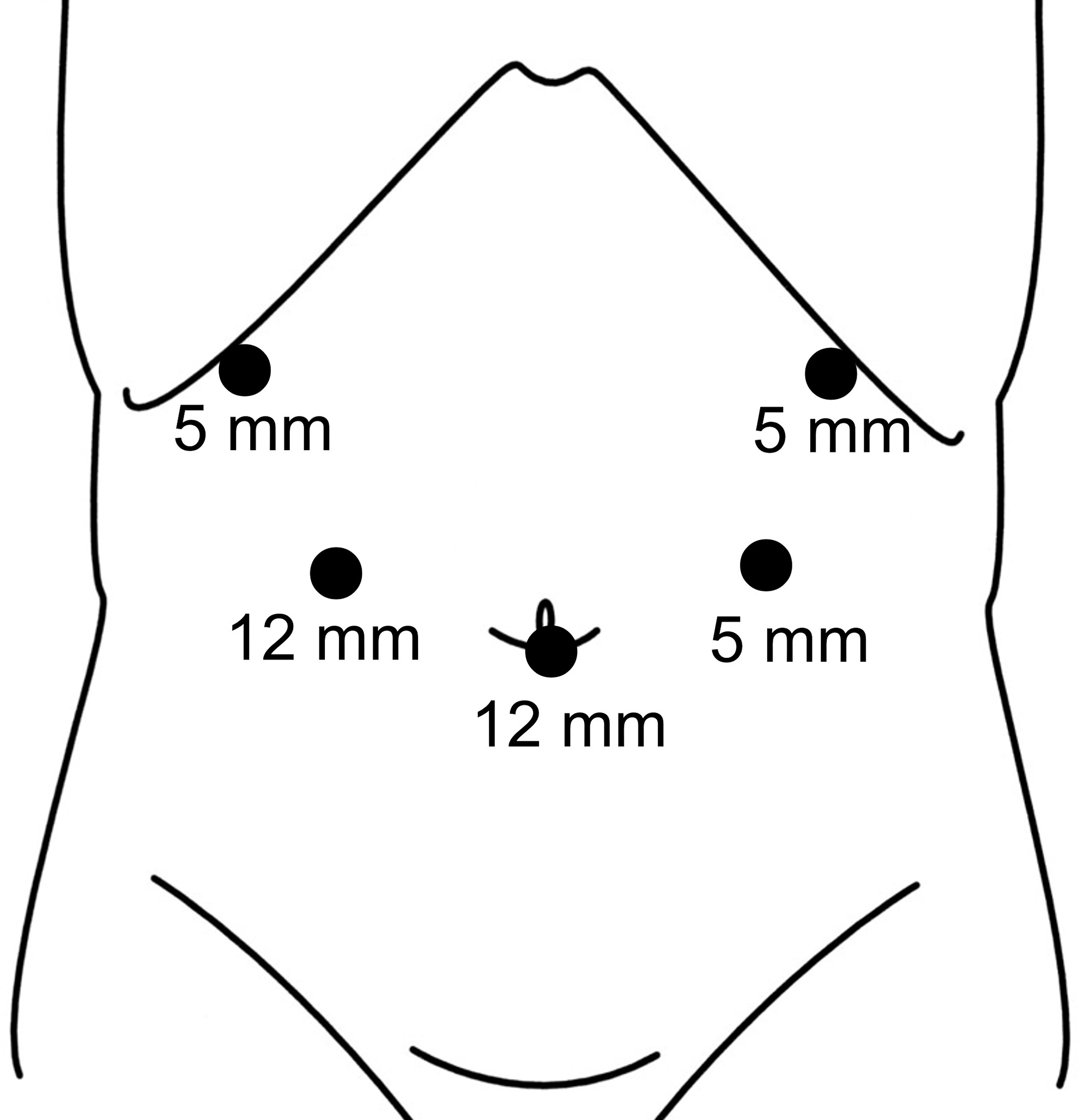
Trocar setting for laparoscopic total gastrectomy.
Surgical approach to the upper side of the gastrosplenic ligament
The greater omentum was divided toward the left up to the lower pole of the spleen. The left gastroepiploic artery was vascularized and divided at the level of its root. Dissection of No. 4sb LNs was then performed.
The fundus and upper body of the stomach were pulled up toward the upper left. The gastropancreatic fold was pulled up vertically, and the left side of the gastropancreatic fold was divided toward the left crus of the diaphragm (Fig. 2A). The gastrodiaphragmatic ligament was divided, and the upper pole of the spleen was exposed (Fig. 2B, C). The upper side of the gastrosplenic ligament was dissected from the retroperitoneum. The fundus of the stomach was pulled up vertically, and the gastrosplenic ligament was extended. Then, the dividing line of the gastrosplenic ligament was defined according to the extent of lymphadenectomy (D1+, D2, D2 + 10; Fig. 2D).

Procedure for the surgical approach to the upper side of the gastrosplenic ligament.
In D1+ lymphadenectomy, the gastrosplenic ligament was divided at the level of the root of the short gastric arteries (Fig. 3A). In D2 lymphadenectomy, LNs along the splenic artery (No. 11p and No. 11d) were dissected, and the gastrosplenic ligament was divided at the same level as for D1+ lymphadenectomy (Fig. 3B). In spleen-preserving D2 + 10 lymphadenectomy, No. 11p and No. 11d LNs were dissected, and the gastrosplenic ligament was divided at the level of the root of the short gastric arteries with dissection of splenic hilar LNs (No. 10) (Fig. 3C). In D2 + 10 with splenectomy, the pancreatic tail and the spleen were mobilized from the retroperitoneum. After dissection of No. 11p and No. 11d LNs, the splenic artery and the splenic vein were vascularized and divided at the level of the pancreatic tail. Dissection of splenic hilar LNs (No. 10) with splenectomy was completed (Fig. 3D).

The view of the splenic hilum after lymphadenectomy.
Procedural details are summarized in a supplemental video clip (Supplementary Video S1).
Results
This procedure was used in 57 patients who underwent LTG for proximal gastric cancer, including D1+ lymphadenectomy in 31, D2 in 18, spleen-preserving D2 + 10 in 4, and D2 + 10 with splenectomy in 4. Patient characteristics and surgical results are summarized in Table 1. Operative time was 341 (192–724) minutes, estimated blood loss was 30 (0–515) g, and no blood transfusion was required. Regarding the required time for lymphadenectomy at the splenic hilum, D1+, D2, spleen-preserving D2 + 10, and D2 + 10 with splenectomy required 24 (13–65), 45 (20–65), 65 (51–117), and 123 (84–137) minutes, respectively (Table 2). There were no intraoperative complications and no conversions to laparotomy in this series.
Characteristics and Surgical Results of All Patients Undergoing Laparoscopic Total Gastrectomy
BMI, body mass index; CD, Clavien–Dindo score; LTG, laparoscopic total gastrectomy.
Surgical Results
LN, lymph node; SHL, splenic hilar lymphadenectomy.
The overall postoperative morbidity rate was 10.5% (6/57). There were two cases of pancreatic fistula, two pulmonary infections, one abdominal infection, and one liver disorder. All postoperative complications were classified as Clavien–Dindo (CD) grade ≤II. There were no postoperative complications classified as CD grade ≥III and no mortality in this series (Table 1).
Discussion
In LTG for gastric cancer, lymphadenectomy at the splenic hilum is technically difficult, not only because of the complexity of the splenic vessels but also because of the deep and narrow operative space at the splenic hilum.6,10 This difficulty results in extending operative time and increasing the risk of severe injury to blood vessels and other organs in the splenic hilum. The latter can cause massive bleeding that sometimes requires blood transfusion and conversion to laparotomy. Several surgeons have reported feasible methods of laparoscopic splenic hilar lymphadenectomy during total gastrectomy.3,7,10 Zheng et al. suggested that knowledge of the vascular anatomical characteristics of the splenic hilum helped surgeons perform LTG safely and effectively. 10
The largest advantage of the present procedure is providing a good operative view around the splenic hilum. By dissecting the retroperitoneal space of the upper side of the gastrosplenic ligament, mobility and extensibility of the gastrosplenic ligament are improved. Thus, it is then possible to view the overall area of the gastrosplenic ligament and facilitate the safe and rapid identification of the splenic vessels and their branches in a deep and narrow space. Furthermore, the laparoscopic amplified view can more clearly visualize vessels, nerves, fascia, and other structures, thereby reducing the risk of injury to the splenic vessels, the spleen, and other organs at the splenic hilum.
Previous studies reported that intraoperative complications, which include injury to major vessels and other organs, were observed in 2.6%–4.4% of patients who underwent laparoscopic gastrectomy for gastric cancer.11,12 Particularly in LTG, it is important to fully understand the vessel anatomy at the splenic hilum to avoid major vessel or splenic injury because the splenic vessels at the splenic hilum are intricate and variable. Several surgeons reported that preoperative evaluation by three-dimensional computed tomography with angiography was helpful to achieve safe laparoscopic spleen-preserving splenic hilar lymphadenectomy.6,13
In the present series, there were no injuries to the spleen or splenic vessels, and no patients who required conversion to laparotomy or blood transfusion. Postoperative complications were reported in 12.0%–26.1% of patients who underwent LTG.3,14,15 In the present series, postoperative complications occurred in 6 of 57 (10.5%) patients, including pancreatic fistula in 2 (3.5%), pulmonary infection in 2 (3.5%), abdominal abscess in 1 (1.8%), and liver disorder in 1 (1.8%). All complications were classified as CD grade ≤II. There were no postoperative complications classified as CD grade ≥III and no mortality within 30 days following LTG, suggesting that the present procedure is technically feasible and can be performed safely without increasing postoperative morbidity and mortality rates.
In patients with advanced proximal gastric cancer (≥cT2) without the greater curvature invasion, the JCOG0110 trial demonstrated that prophylactic splenectomy should be avoided to improve operative safety and survival. 16 Therefore, in accordance with the 5th Japanese Gastric Cancer Treatment Guidelines, the definition of standard-D2 lymphadenectomy during total gastrectomy does not include the splenic hilar LNs (No. 10). 8 D2 + 10 lymphadenectomy with or without splenectomy could be considered extended lymphadenectomy exceeding D2 for advanced proximal gastric cancer with the greater curvature invasion.
D2 + 10 lymphadenectomy with splenectomy has been reported to increase the mortality rate and postoperative complications, including pancreatic fistula, abdominal abscess, and portal thrombosis, as well as compromising the immune system.17,18 To reduce the risk of these postoperative complications, LTG with spleen-preserving splenic hilar lymphadenectomy has been performed increasingly for advanced proximal gastric cancer with the greater curvature invasion.6,13,19 Several surgeons reported that laparoscopic spleen-preserving splenic hilar lymphadenectomy was feasible.14,19,20 Thus, for LTG, the extent of splenic hilar lymphadenectomy (D1+, D2, D2 + 10) must be defined exactly according to tumor progression.
In the present series, splenic hilar LNs (No. 10) were not dissected in D1+ lymphadenectomy for early proximal gastric cancer (cT1) and D2 lymphadenectomy for advanced proximal gastric cancer (≥cT2) without greater curvature invasion. Spleen-preserving D2 + 10 lymphadenectomy was performed in patients with advanced gastric cancer (≥cT2) invading the greater curvature and without splenic hilar LN metastasis, whereas D2 + 10 lymphadenectomy with splenectomy was performed in patients with splenic hilar LN metastasis. In this procedure, it is possible to define the extent of splenic hilar LNs precisely under the excellent operative view of the overall area of the gastrosplenic ligament and easily and safely determine the dividing line of the gastrosplenic ligament in accordance with the extent of lymphadenectomy (D1+, D2, D2 + 10).
Conclusions
In LTG, the present procedure can provide an excellent operative view at the splenic hilum, making it easier to determine the extent of lymphadenectomy at the splenic hilum precisely according to cancer progression.
Footnotes
Authors' Contributions
S.K. contributed to writing the article; T.T., K.H., and T.Y. gave technical support; K.G., and Y.S. gave conceptual advice; Y.O., S.T., and H.K. were in charge of review process; H.B. supervised the whole drafting process; all authors read and approved the final article.
Ethical Approval
This study was performed with approval of the Institutional Review Board of Ishikawa Prefectural Central Hospital in Japan (No. 2225).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.