
Abstract
Background:
Modified Anderson-Hynes pyeloplasty is currently preferred for ureteropelvic junction obstruction (UPJO). Extravasation of urine and anastomotic stenosis are the most common complications after Anderson-Hynes pyeloplasty, which are closely linked with the technique for anastomosis. However, there are currently no clear guidelines for the suture bite depth in suturing the anastomosis during pyeloplasty.
Objective:
To analyze the optimal suture bite depth in laparoscopic Anderson-Hynes pyeloplasty.
Study Design:
A total of 90 children aged 4–14 years with UPJO-induced hydronephrosis who were surgically treated in the First People's Hospital of Lianyungang from July 2019 to July 2022 were prospectively recruited. All received laparoscopic Anderson-Hynes pyeloplasty using 5-0 Vicryl continuous sutures. According to the suture bite depth, the patients were divided into group A (depth 1 mm, n = 46) and group B (depth 0.5 mm, n = 44). Operation time, postoperative drainage volume, time of ureteral stent removal, incidence of postoperative complications, and time to hydronephrosis resolution were compared between groups.
Results:
Group A showed significantly less postoperative drainage volume, and shorter time of ureteral stent removal and hydronephrosis resolution (all P < .05). Four cases in group B received replacement of a double-J stent. Except for 1 patient receiving reoperation for anastomotic stenosis caused by massive extravasation of urine, the replaced double-J stent was successfully removed from the remaining 3 patients at 3 months, and the symptoms of anastomotic stenosis disappeared. No significant difference was detected in the operation time between groups (P > .05).
Conclusion:
An appropriate deeper suture bite depth for anastomosis may reduce postoperative urine extravasation and related complications in children who received laparoscopic pyeloplasty for UPJO-induced hydronephrosis.
Introduction
Ureteropelvic junction obstruction (UPJO) is a common ureteral malformation in children. Modified Anderson-Hynes pyeloplasty is currently preferred for UPJO, 1 but may be accompanied with various complications, especially extravasation of urine and anastomotic stenosis that are closely linked with the procedures for anastomosis.2,3 No guideline consensus has reached about the suture bite depth in pyeloplasty, and its correlation with postoperative complications of pyeloplasty have been rarely explored. In the present study, we analyzed 90 children aged 4–14 years who had undergone UPJO-induced hydronephrosis for laparoscopic Anderson-Hynes pyeloplasty from July 2019 to July 2022. We compared surgical outcomes of two suture bite depths (1 versus 0.5 mm) for anastomosis suturing, thus providing references for improving UPJO treatment in children.
Methods
Subjects and clinical data
A total of 90 children (70 boys and 20 girls, age 4–14 years) with UPJO-induced hydronephrosis who were surgically treated with the modified Anderson-Hynes pyeloplasty in the First People's Hospital of Lianyungang from July 2019 to July 2022 were prospectively recruited. All patients were graded in American Society of Anesthesiologists (ASA) I-II according to the preoperative ASA Physical Status Classification System. Inclusion criteria: (1) UPJO-induced hydronephrosis preoperatively diagnosed by the color Doppler ultrasonography and magnetic resonance of the urinary system; (2) split renal function >10% examined by preoperative nuclide scanning; (3) moderate and severe hydronephrosis with an anterior-posterior diameter of ≥25 mm; and (4) unilateral hydronephrosis.
Exclusion criteria: (1) hydronephrosis caused by urinary stones, posterior urethral valves or other non-UPJO causes; (2) major underlying diseases and other comorbidities; and (3) younger than 4 years. Those with an admission registration number ending in an odd number were included into group A (n = 46), and the remaining were included into group B (n = 44). Clinical data of patients in group A and B are listed in Table 1. This study was approved by the Ethics Committee of the People's Hospital (KY-20160713002). Written informed consent was provided by guardians of recruited children.
Clinical Data of Recruited Children with Ureteropelvic Junction Obstruction-Induced Hydronephrosis (n = 90)
Significant difference was calculated as χ 2 .
Significant difference was calculated as t-value.
APD, anterior-posterior diameter; UPJO, ureteropelvic junction obstruction.
Surgical procedures
General anesthesia was performed using endotracheal intubation. The patient was placed in the lateral recumbent position, with the abdominal wall close to the bedside and the affected side upper and oblique to create a 75° angle to the dorsal side. Medical transparent adhesive film was used to protect the skin. The patient was fixed on the surgery table with medical tapes (Fig. 1). Pneumoperitoneum was established using carbon dioxide (CO2) insufflation into the abdominal cavity. The intra-abdominal pressure (IAP) was adjusted to 8–12 mmHg according to the body weight, and typically, an IAP of 10 mmHg was adopted.

The patient position.
Three small incisions (0.5 cm in size) were made at the upper edge of the umbilical ring (incision 1), 3–5 cm above (incision 2) and below it (incision 3). A 5 mm camera trocar was laterally inserted from incision 1 at 30°, and the other two working trocars were inserted from incisions 2 and 3. The lateral peritoneum and mesentery were dismembered on the right and left side, respectively, followed by the exposure of the ureteropelvic junction (UPJ).
The renal pelvis and ureter were both suspended using 2-0 Prolene sutures (Fig. 2). In brief, 2 needles were inserted by 2–3 cm above the skin projection of the UPJ alongside the anterior axillary line, with an interval of 3–4 cm. The first needle was inserted by 2 cm from the UPJ on the lateral side of the ureter and 1 cm from the UPJ on the lateral side of the renal pelvis; the second needle was inserted by 3 cm from the UPJ on the interior side. The renal pelvis was preserved.
The renal pelvis and ureter were suspended together.
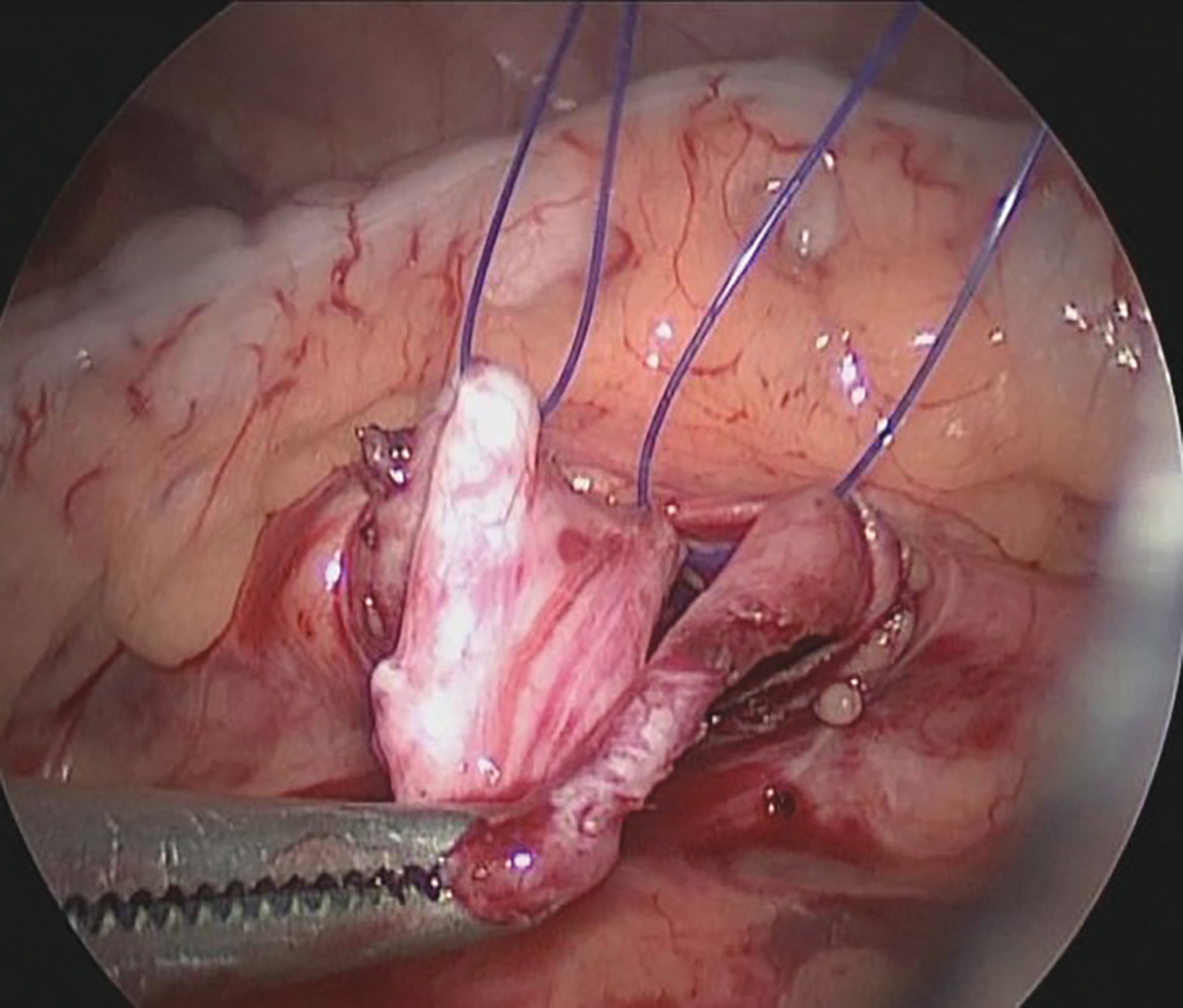
Subsequently, the renal pelvis was dissociated at 1 m from the suspending sutures to leave a space for suturing. The ureter was split longitudinally to 0.5 cm below the suspension sutures (Fig. 3), and tissues between the UPJ and the ureter were partially incised for the following tissue traction. The posterior wall of the anastomosis was first sutured using 5-0 absorbable sutures. After the placement of a double-J stent to splint the anastomosis with one side in the bladder and the other side in the renal pelvis via a Veress needle, the anterior wall of the ureter was continuously sutured using 5-0 absorbable sutures. The UPJ was then completely dissociated before the last sutures. The abdominal cavity was closed layer by layer.

The ureter was split.
About 1- and 0.5-mm suture bite depths were made in group A and B during the suture of renal pelvis to ureter, respectively. The suture thickness and tightness of the suture were made as the same as possible. The suture bite depth was measured referring to the diameter of the 2-0 suspended Prolene suture (Φ = 0.3 mm) (Fig. 4). Both groups were operated by the same surgeon. The abdominal drainage tube was removed if less than 20 mL of fluid was drained within 24 hours after surgery.

The bite depth referring to the Prolene suture.
Surgical outcomes
Surgical outcomes included operation time, postoperative drainage volume, time of ureteral stent removal, incidence of postoperative complications, and time to hydronephrosis resolution.
Statistical analysis
Statistical analysis was performed using SPSS 25.0. Measurement data that were normally distributed were expressed as mean ± standard deviation and compared between groups using the independent sample t-test. Enumeration data between groups were compared by the chi-square test. P < .05 was considered as statistically significant.
Results
Surgical indexes
There was no significant difference in the operation time between groups A and B (P > .05). Compared with that in group B, time of ureteral stent removal was significantly shorter in group A (P < .05). Four cases in group B received replacement of a double-J stent. Except for one reoperated patient with anastomotic stenosis caused by the massive extravasation of urine, the replaced double-J stent in the remaining 3 patients was successfully removed at 3 months, and the symptoms of anastomotic stenosis disappeared. None in group A required a replacement of double-J stent (Table 2).
Surgical Indexes of Recruited Children with Ureteropelvic Junction Obstruction-Induced Hydronephrosis (n = 90)
Postoperative drainage volume
We measured 24 hours drainage volume on at day 1, 2, and 3 postoperatively. Compared with those in group A, the 24 hours drainage volume at each time point was significantly larger in group B (all P < .05). It is suggested that a greater suture bite depth may be correlated with a less postoperative drainage volume (Table 2).
Postoperative ADP
All patients were followed up through measuring ADP at 3, 6, and 9 months postoperatively. Compared with those in group A, the ADP at each time point was larger in group B, although significant differences were only detected in those at 6 and 9 months (P < .05) (Table 3).
Postoperative Anterior-Posterior Diameter of Recruited Children with Ureteropelvic Junction Obstruction-Induced Hydronephrosis (n = 90)
Discussion
Surgical outcomes of different suturing techniques for anastomosis have been previously compared to determine the optimal sutures. Gao et al. 3 have demonstrated that surgical outcomes and postoperative complications do not differ between the open or laparoscopic dismembered pediatric pyeloplasty. A meta-analysis has also described similar surgical outcomes of continuous and interrupted sutures. 2 Andolfi et al. 4 have demonstrated that the success rate of robot-assisted laparoscopic pyeloplasty is comparable to that of conventional laparoscopy. However, there are currently no clear guidelines for the suture bite depth in suturing the anastomosis during pyeloplasty.
A deeper suture bite depth has been considered to cause the anastomotic stenosis in the ureters that are narrow. Interestingly, our data provided an opposite finding that a greater suture bite depth during the modified Anderson-Hynes pyeloplasty did not cause the anastomotic stenosis. Not only that, the patients in group A with a greater suture bite depth presented less postoperative drainage volume, shorter time of ureteral stent removal and hydronephrosis resolution, and lower incidence of postoperative complications than those in group B. The drainage function of ureters need to be maintained continuously after surgery.
During the healing process of anastomosis, urine continuously flows through the constantly peristaltic ureters. A loose suturing of anastomosis would cause extravasation of urine, which may further cause poor healing, scar hyperplasia, and a long-term ureteral obstruction. Therefore, extravasation of urine has become the most common cause of anastomotic stenosis. 5 A relatively great suture bite depth ensures the tightness of the ureters and favors the healing of anastomosis.
The necessity of postoperative drainage after pyeloplasty remains controversial. Ahmed and Crankson 6 have reported that an extrarenal wound drain is favorable to patients after pyeloplasty. However, Ruhle et al. 7 have proposed that an intubation using ureteral stents is sufficient for drainage after pyeloplasty. We believed that an extrarenal wound drainage after pyeloplasty is more preferred than an intubation, especially for inexperienced surgeons. An extrarenal drainage timely drains the extravasated urine out of the body, thereby favoring the healing of anastomosis and reducing the negative influences of extravasation of urine into the abdominal cavity and intestinal tract. The volume of extrarenal wound drainage usually represents the amount of urine leaked from the anastomosis.
In the present study, the 24 hours drainage volumes at the first, second, and third day postoperatively were all significantly larger in group B than in group A, suggesting that a greater suture bite depth is conductive to prevent extravasation of urine and lower the short-term and long-term incidence of postoperative complications.
It is reported that the cure rate of postoperative relapsed UPJO managed by reoperation, endopyelotomy, placement of a double-J stent, and balloon dilatation is 83.3%, 50.0%, 45.5%, and 30.8%, respectively, which is far from the success rate of the initial surgery (98.0%).8–10 In our study, 3 of the 4 children in group B were postoperatively managed by the replacement of a double-J stent due to anastomotic stenosis and were all cured 3 months later. One child was reoperated due to the aggravation of hydronephrosis after the removal of the double-J stent. For children with the relapse of UPJO-induced hydronephrosis after pyeloplasty, replacement of a double-J stent is considered as a simple and low-risk intervention.
As the key to a successful Anderson-Hynes pyeloplasty, accurate excision and anastomosis of the renal pelvis and ureter can decrease the incidence of postoperative complications, like urinary leakage at the anastomosis. 2 An auxiliary suspension technology contributes to shortening the operation time by lowering the surgical difficulty. Here, the renal pelvis and ureter were both suspended before anastomotic suturing. The fixations by suspending sutures and clear exposure of the incision provide conveniences for the accurate anastomosis of the renal pelvis and ureter with a proper suture bite depth.9,11
In the present study, we did not recruit children younger than 3 years because of the adverse surgical outcomes associated with thinner ureters.
Conclusions
Collectively, our data suggested that an appropriate deeper suture bite depth in laparoscopic pyeloplasty of children with UPJO-induced hydronephrosis can increase the success rate of the surgery, lower the incidence of postoperative complications, and reduce the pain and medical cost. A leak-free anastomosis of thin ureters in children requires a thorough research.
Footnotes
Acknowledgments
The authors gratefully acknowledge the trust and support given by staff of our hospital.
Authors' Contributions
G.S.D. and L.H. designed the study; G.S.D. collected the data. G.S.D. wrote and revised the article; all the authors read and approved the final article.
Ethics Approval and Consent to Participate
The research has been performed in accordance with the declaration of Helsinki. Our study was approved by the Ethics Committee of The First People's Hospital of Lianyungang. The number of Institution approval is KY-20160713002, and the date is 06/04/2019.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received grant from Health Science and Technology Project of Lianyungang city (Grant Number: 202111).