
Abstract
Purpose:
Retroperitoneal robotic-assisted pyeloplasty (ret-RAP) for ureteropelvic junction obstruction (UPJO) requires a larger retroperitoneal space (RS) to maintain specified distances between robotic (da Vinci) trocars and between trocars and the region of interest. A modified closed technique (MOT) and conventional closed technique (COT) were compared for creating an adequate RS with optical trocars.
Methods:
RS access in children with UPJO who underwent ret-RAP (n = 30) was MOT (n = 15) and COT (n = 15). All patients were positioned laterally. For MOT, a 5 mm optical trocar was inserted at the angle formed between the 12th rib and the erector spinae muscles. As the trocar was advanced under direct vision, it pierced the superficial subcutaneous layer, Scarpa's fascia, lumbar fascia, internal/external oblique and transversus abdominalis muscles, and the posterior renal fascia. Once in the RS, the tip of the scope was used for blunt dissection of perirenal fat, the tip was withdrawn until it was outside the perirenal fascia, and used to dissect toward the anterior abdomen in the pararenal fat layer.
Results:
Ages and weights at ret-RAP were similar (MOT: 5.6 ± 1.8 years versus COT: 7.8 ± 4.6 years; MOT: 20.6 ± 10.1 kg versus COT: 27.6 ± 13.9 kg). Times for RS access were similar (MOT: 1.6 ± 0.5 minutes versus COT: 1.9 ± 0.7 minutes), but RS expansion was significantly quicker in MOT (32.3 ± 8.7 minutes versus 52.0 ± 15.1 minutes; P < .001). Peritoneal injury caused carbon dioxide leakage in 4 of 15 COT cases and 0 of 15 MOT cases.
Conclusion:
RS expansion with MOT was safer because there were no peritoneal injuries and MOT was quicker than COT.
Introduction
Robotic-assisted pyeloplasty (RAP) for ureteropelvic junction obstruction (UPJO) has gained increasingly wider acceptance and is currently one of the most commonly performed robotic procedures in pediatric surgery. In fact, recent trends in UPJO treatment modalities in children suggest there is evidence emphasizing that RAP is overtaking laparoscopic or open pyeloplasty 1 mainly because robotic technology has technical advantages such as 3D visualization, increased degrees of freedom of movement, and enhanced reconstructive capabilities. RAP can be performed transperitoneally or retroperitoneally and there is still some controversy concerning which approach is least invasive.
The feasibility and efficiency of retroperitoneal RAP (ret-RAP) have been reported for pediatric UPJO2–5 and there are several advantages. Ret-RAP allows direct access to the ureteropelvic junction and hilar vessels, without the need for retraction of abdominal contents or intra-abdominal maneuvers before reaching a kidney, essentially eliminating risks for bowel or intraperitoneal organ injury and preventing the development of intraperitoneal adhesions.
However, it is technically difficult to create a working space in the retroperitoneum consistently, because essentially it is a potential space occupied by areolar connective tissue and fat, which may explain why many pediatric surgeons prefer the transperitoneal approach because of advantages such as a larger operative field and more familiar working environment that are more convenient for intracorporeal suturing.
Several techniques for accessing the retroperitoneum have been described 6 with the most common approach being an open technique using blunt finger dissection and a balloon to create an adequate working space. Although this technique has proven to be safe and associated with little risk for injury, there is risk for CO2 leakage that can reduce the volume of the retroperitoneal space (RS), disrupting visibility, and prolonging operative time. In a previous report, the conventional blunt finger/balloon open technique and a conventional closed technique (COT) using an optical trocar were compared for creating an adequate RS for pediatric renal surgery. 7
This report supported published evidence 3 that COT with an optical trocar allowed retroperitoneal access to be established, but the RS created was inadequate for robotic surgical system (RSS) use because a larger RS is required because of specified distances between RSS trocars and between RSS trocars and the region of interest that must be maintained. Here, a modified closed technique (MOT) and conventional closed technique (COT) were compared for creating a larger RS for ret-RAP with an optical trocar.
Materials and Methods
All pediatric UPJO patients treated by ret-RAP between November 2018 and May 2023 at a single institute were reviewed. Diagnosis of UPJO was made using computerized tomography, ultrasonography, magnetic resonance imaging, diuretic renography, and diethylene-triamine-penta-acid renography. Inclusion criteria for this study were significant flank pain, infection, or decreased renal function. Only patients with unilateral single system hydronephrosis were included in this study. Patients with previous renal surgery were excluded. All ret-RAPs were performed by a team of 2 board-certified pediatric surgeons (H.K. and A.Y.) with extensive technical experience.
Perioperative and postoperative data including age and weight at surgery, body mass index (BMI) at surgery, incidence of preoperative pyelonephritis, time taken to access the retroperitoneum (retroperitoneum access time [RAT]), time taken to create an adequate RS (RS creation time [RSCT]), incidence of intraoperative peritoneal tears, leakage of CO2, and duration of postoperative narcotic use were analyzed.
Surgical technique
Common preoperative management
After induction of general endotracheal anesthesia, the patient was placed in the lateral decubitus position with the affected side up, slightly flexed with a small gel positioner under the contralateral iliac crest. All retroperitoneal procedures were performed in the lateral decubitus position. The operating surgeon, assistant, and nurse were positioned along the patient's back with the monitor on the opposite side of the operating table. A Foley catheter was inserted to decompress the bladder.
COT using an optical trocar
The initial access point was below the costovertebral angle at the lateral border of the sacrospinalis muscle (i.e., the angle between the 12th rib and the erector spinae muscles). A 5 mm incision was made and a bladeless optical trocar (Xcel™; Ethicon Endo-Surgery, Cincinnati, OH, USA) was inserted and advanced under direct vision. The optical trocar allowed the operator to confirm orientation visually, that is, view external/internal/oblique and transversus abdominalis muscles clearly and identify the posterior renal fascia. After passing through the posterior renal fascia, the RS is indicated by the presence of fat. Insufflation with CO2 at 6–12 mmHg was commenced.
Blunt camera dissection was then used to dilate the RS under direct vision by swinging the laparoscope from posterior to anterior, taking great care not to injure the retroperitoneum. Additional second and third trocars were placed under scope guidance. Note the assistant's trocar must be positioned more posteriorly in ret-RAP cases to reduce the risk of conflicts with RSS arms.
MOT with an optical trocar
A 5 mm optical trocar was inserted at the same position as for COT (Fig. 1) and advanced. Once in the RS, the tip of the scope was used for blunt dissection of perirenal fat (Fig. 2a). The tip of the scope was withdrawn until it was outside the perirenal fascia and used to dissect toward the anterior abdomen in the pararenal fat layer (Fig. 2b). The lateroconal fascia can readily be identified blending with the peritoneal reflection (Fig. 2c). A second trocar was placed under scope guidance after the reflection was dissected and a third trocar placed after confirming anatomic relations and preventing inadvertent peritoneal injury (Fig. 2d).
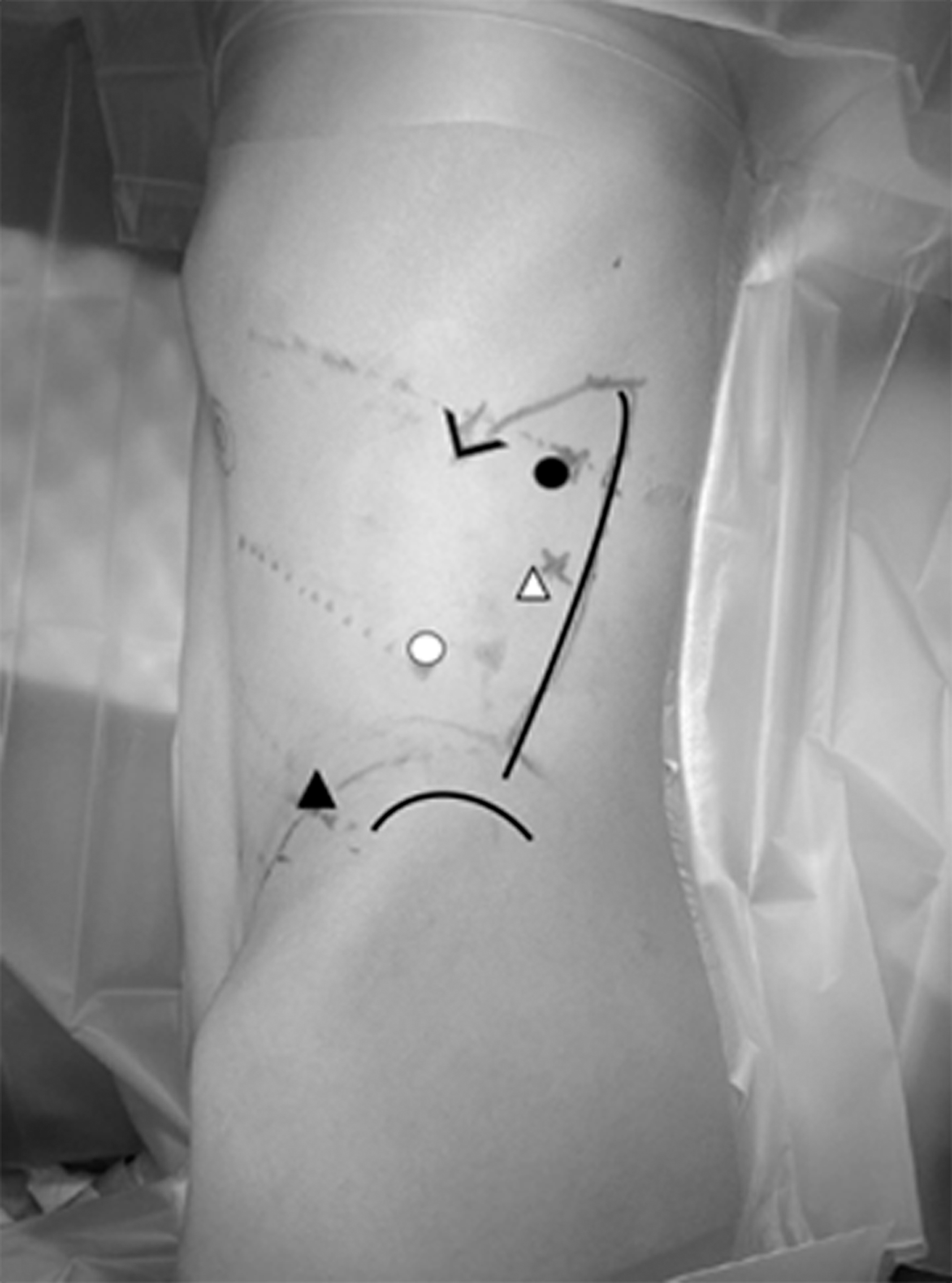
Trocar positions for retroperitoneal RAP. The initial access point is below the costovertebral angle at the lateral border of the sacrospinalis muscle (i.e., the angle between the 12th rib and the erector spinae muscles) for the surgeon's right hand (black circle). After creating a working space in the retroperitoneum, an additional second trocar for the scope (white circle) and third trocar for the surgeon's left hand (black triangle) are placed under scope guidance. Another trocar for the assistant is also placed (white triangle). RAP, robotic-assisted pyeloplasty.

Modified closed technique with an optical trocar. A 5 mm optical trocar (blue) was inserted at the point below the costovertebral angle at the lateral border of the sacrospinalis muscle.
RAP anastomosis
The da Vinci Xi Surgical system (Intuitive Surgical, Sunnyvale, CA, USA) was used for RAP in this study. Although the da Vinci system has four robotic arms, only three were used. Three 5 mm laparoscopic trocars were replaced with three 8 mm da Vinci trocars. The robotic platform was prepared and docked from the anterior aspect of the patient using a 0° telescope camera. Microbipolar forceps and Maryland forceps or needle driver were inserted on the left and right sides, respectively. RAP was performed with interrupted 5/0 or 6/0 absorbable sutures with all knots tied intracorporeally. 3 Once the posterior wall anastomosis was completed, a Double-J stent (4.7F) was placed using an antegrade approach transcutaneously with a guide wire or a retrograde approach with a cystoscope.
Common postoperative management
A retroperitoneal closed suction drain was placed through the trocar site to monitor and manage any anastomotic leakage. The Foley catheter was removed 2–3 days postoperatively. The drain was removed once output decreased to <10 mL per day. The stent was removed 4–6 weeks postoperatively.
Statistics/ethics
Data are expressed as mean ± standard deviation. The Student's t test and chi-squared test were used for statistical analysis. A P-value of <.05 was considered to be statistically significant. This study was approved by the Juntendo University School of Medicine Institutional Review Board (IRB number: J18-024) and complies with the Helsinki Declaration of 1975 (revised 1983).
Results
Ret-RAP access was MOT (n = 15) and COT (n = 15). All cases were treated successfully by RALP without conversion to open repair. There were no significant differences between the two groups for age at the time of surgery: 5.6 ± 1.8 years for MOT versus 7.8 ± 4.6 years for COT; P = .09; weight at the time of surgery: 20.6 ± 10.1 kg for MOT versus 27.6 ± 13.9 kg for COT; P = .12; BMI: 16.5 ± 1.2 kg/m2 for MOT versus 17.2 ± 2.3 kg/m2 for COT; P = .28; and incidence of preoperative pyelonephritis was 3 of 15 (20%) for MOT versus 1 of 15(6.6%) for COT; P = .59 (Table 1).
Subjects
BMI, body mass index; COT, conventional closed technique using an optical trocar; MOT, modified closed technique using an optical trocar; NS, not significant.
RAT was similar for MOT and COT with no subsequent bleeding from any port site (1.6 ± 0.5 minutes for MOT versus 1.9 ± 0.7 minutes for COT; P = .11). RSCT was significantly quicker for MOT (32.3 ± 8.7 minutes versus 52.0 ± 15.1 minutes; P < .001). There was no CO2 leakage at initial port sites in both MOT and COT cases; however, incidence of intraoperative peritoneal tears causing CO2 leakage in COT was significantly higher than that in MOT; 4 of 15 (26.7%) for COT versus 0 of 15 (0%) for MOT; P = .03.
Retroperitoneal tears were repaired with Endo-loops (Ethicon Endo-Surgery, Blue Ash, OH, USA) under retroperitoneoscopic guidance. Mean time taken to ambulate and duration of postoperative narcotic use were not significantly different (1.8 ± 0.7 days for MOT versus 1.5 ± 0.6 days for COT; P = .21, 1.4 ± 0.7 days for MOT versus 1.3 ± 0.5 days for COT, respectively; P = .65) (Table 2).
Modified Technique Versus Conventional Technique
COT, conventional closed technique using an optical trocar; MOT, modified closed technique using an optical trocar; NS, not significant.
Discussion
The most crucial aspect of successful retroperitoneal surgery is creating an adequate RS that does not leak CO2 from either the initial trocar access site or a peritoneal tear. Because insertion is by stabbing and advancement can be viewed clearly, there is good tissue tension around the trocar that prevents CO2 leakage consistently. The lateral decubitus position also helps because abdominal contents are displaced downward because of gravity effectively increasing the potential space in the retroperitoneum. Pediatric patients also have less fat than adults. Thus, creating a good RS should be easier and simpler in children because the initial trocar insertion is more stable.
In fact, there was no leakage of CO2 at the original trocar access site noted in any case in this series because of the tight seal achieved around the trocar as a consequence of advancing through multiple layers of tissue, allowing insufflation pressures of 6–12 mmHg to be established and maintained during scope dissection and during insertion of additional trocars into a nicely expanded RS. Of note is that there was also no CO2 leakage while 5 mm trocars were replaced with 8 mm da Vinci trocars; in other words, MOT provided a stable RS for ret-RAP.
Peritoneal tear is a common complication of retroperitoneal laparoscopic procedures and occurs most often during the clearance of perirenal fat and incision of the lateroconal fascia. Although incidence of peritoneal tear can be correlated with the operating surgeon's skill and experience, an important preventive measure is to confirm continuity of the lateroconal fascia to the peritoneal reflection under direct vision. However, if a peritoneal tear occurs, CO2 leakage causes the RS to collapse resulting in progressive loss of working space and clear vision that increases difficulty and risk for technical complications.
In this study, there were four peritoneal tears in COT cases that occurred when ret-RAP was first introduced for treating UPJO related to dissecting perirenal fat concealing the peritoneal reflection. MOT allows dissection to progress gently with confidence because the peritoneal reflection can be identified under direct vision. Indeed, no MOT case was complicated by peritoneal tear during creation of an RS in this series. In this study, the most crucial complication was peritoneal tear, limited to COT cases and provided MOT is performed cautiously and precisely, peritoneal tear is not expected to occur.
However, repairing a compromised peritoneum is somewhat complicated in retroperitoneal cases. Most surgeons would consider repairing a peritoneal defect with a surgical clip. In practice, this can be difficult because of positive peritoneal pressure. The peritoneum around the clipped defect must not be under tension, otherwise a defect may become larger. In particular, the peritoneum in children is thin and closing a defect may cause attenuation or tension with potential for further tearing or rupture. The pediatric thin peritoneum after closing the defect would get tensioned and attenuated, which is more likely to get ruptured again during the following dissection procedure.
Other options would include inserting a Veress needle into the abdomen. CO2 in the peritoneal space will be vented through the needle, thus the collapsed RS could be decompressed and enlarged. In addition, theoretically, the peritoneal tear could be extended to equalize the pressure between the peritoneal space and RS, 8 but it is difficult to determine to what extent the defect needs to be extended. In this series, all 4 cases of peritoneal tears were closed with Endo-loops after the insufflation pressure was reduced to 4 mmHg to eliminate tension on the peritoneum. Endo-loops would also be expected to prevent secondary peritoneal injury from surgical clips.
This study has limitations because of its retrospective nature, small number of cases, and possible learning curve issues. The success of ret-RAP relies clearly on establishing a good RS as a larger RS improves instrument movement, meaning less risk for collisions between instruments and parts of the RSS. Although the da Vinci Xi system has less bulky arms that improve its application to pediatric surgical procedures, an RS that includes the anterior axillary line for the third trocar placement is mandatory for RAP because the peritoneal reflection is consistently anterior to the posterior axillary line. 9
In this study, there was no bleeding or tissue injury at the initial trocar site associated with a bladeless optical trocar. In fact, there are no reports in the literature about complications subsequent to using the type of bladeless optical trocar used in this study. As with any procedural/technical modifications, there is a learning curve and because MOT cases were performed after COT cases, outcome of COT could be attributed to experience. However, as both operating surgeons have performed numerous retroperitoneal procedures successfully, learning curve bias was considered negligible.
RAP, whether transperitoneal or retroperitoneal, would appear to be better than laparoscopic or open pyeloplasty because RSS overcomes many of the limitations encountered during surgery, especially during laparoscopic surgery.2,10,11 RSS allows complicated and delicate reconstructive procedures in challenging circumstances to be more manageable, and complicated suturing with RSS is likely to be preferred because of easier than for endoscopic suturing, especially retroperitoneal.2,3
As a result, MOT would appear to be the superior technique for establishing a stable RS for ret-RAP, and according to Blanc et al., ret-RAP had a shorter operative time, shorter hospital stay, and earlier recovery of bowel activity with earlier resumption of oral intake than transperitoneal RAP. 2 Options for establishing an adequate RS for ret-RAP have not previously been compared and would interest pediatric surgeons treating children with UPJO.
Footnotes
Authors' Contributions
H.K. and A.Y. designed the study. H.K., S.Y., M.T., T.O., S. Seo, S. Shibuya, Y.Y., R.A., and A.Y. were involved in clinical treatment. H.K., T.O., and N.F. collected and analyzed data. H.K. and G.J.L. prepared the article. G.J.L. revised the article as a native English speaker. All authors have read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.