
Abstract
Background:
The incidence of complications in gastric cancer (GC) patients after surgery was increasing, and it was not clear whether postoperative complications would have an impact on prognosis. The current study attempted to investigate the role of postoperative complication for prognosis on GC patients undergoing radical resection.
Materials and Methods:
Eligible studies were searched in three databases, including PubMed, Embase, and the Cochrane Library, in accordance with the searching strategy on September 4th, 2022. The survival values were most concerned; then, hazard ratios (HRs) and 95% confidence intervals (CIs) were pooled up. All prognostic values, including overall survival (OS), disease-free survival (DFS), disease-specific survival (DSS), and recurrence-free survival (RFS), were allowed. Subgroup analysis based on complication types was used for further in-depth research.
Results:
A total of 29 studies involving 33,858 patients were included in this study. Intra-abdominal abscess (19.4%) was the most common complications in the included studies, followed by anastomotic leakage (17.0%) and pneumonia (16.4%). There were 23, 4, 6, and 10 studies that reported OS, DFS, DSS, and RFS, respectively. After analysis, postoperative complication was found to be an independent prognostic factor for OS (HR = 1.52, I2 = 1.14%, 95% CI = 1.42–1.61, P = .00), DFS (HR = 1.71, I2 = 0.00%,95% CI = 1.44–1.98, P < .05), DSS (HR = 1.60, I2 = 54.58%, 95% CI = 1.26–1.93, P < .1), and RFS (HR = 1.26, I2 = 0.00%, 95% CI = 1.11–1.41, P < .05). Subgroup analysis found that noninfectious complication was not significantly associated with OS (HR = 1.39, I2 = 0.00%, 95% CI = 0.96–1.82, P > .05).
Conclusion:
Surgeons needed to pay more attention to GC patients who developed postoperative complications, especially infectious complications, and take proactive management to improve the prognosis.
Introduction
According to the International Agency for Research on Cancer, gastric cancer (GC) was the fifth most common cancer with 10.81 million new cases and the fourth leading cause of cancer death with 0.77 million deaths in 2020. 1 Although the medical level and technology improved greatly, radical surgery with lymph node dissection was still the most effective and preferred curative treatment option for GC.2–5 The recurrence of cancer and survival time after surgery was a huge challenge, with ∼8.3% of patients experiencing recurrence and a 5-year relative survival rate of ∼30% nowadays.6,7 However, there was also many patients suffering from postoperative complications, which might be related to the malnutrition in GC patients.8–10 The short-term outcomes also needed to be of concern.
Postoperative complication was usually defined as any morbidity that developed within 30 days after surgery.11,12 It could be categorized as local complications and systematic complications. 13 Local complications included surgical-site infection, bleeding, anastomosis leakage, obstruction, etc. Systematic complications included pulmonary infection, diarrhea, liver dysfunction, heart failure, etc. Although perioperative mortality of GC patients declined over the past decades, the incidence of postoperative complications remained high that ranged from 10.5% to 40.1%.14–16 Therefore, reducing the incidence and severity of postoperative complications might also have a potential role to improve long-term outcomes.
The prognostic value of postoperative complications for GC patients was reported by some previous studies.17–45 Most studies demonstrated that there was a significant association between complications and survival rate.18,20,22–25,27–31,33,34,36–45 However, some other studies held a different view and revealed that the current evidence did not support a negative impact of postoperative complications on GC.17,19,21,26,32,35 Therefore, the purpose of this study was to solve the controversy.
Materials and Methods
This study was produced according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 46
Search strategy
The search strategy included three key words: complications, GC, and prognosis. As for complications, the search terms were: “complications” OR “adverse events” OR “surgical outcomes” OR “harms.” As for GC, the search terms were: “gastric cancer” OR “gastric carcinoma” OR “gastric neoplasms” OR “stomach cancer” OR “stomach carcinoma” OR “stomach neoplasms.” As for prognosis, the search terms were: “survival” OR “mortality” OR “death” OR “prognosis” OR “period analysis” OR “long term” OR “survivors.” The searching scope was limited in titles and abstracts. Language was limited in English.
Inclusion and exclusion criteria
The inclusion criteria of the current study were: (1) patients who were diagnosed as GC and underwent radical surgery; (2) the types and incidence of postoperative complications were reported; (3) at least one prognostic indicator was reported; and (4) only the study type of article was allowed. The exclusion criteria of this study were: (1) insufficient data of postoperative complications and prognostic indicators; (2) the study types were case report, review, meta-analysis, letters to editor, comments, or conferences; and (3) data were repeated or overlapped.
Study selection
Two authors searched the eligible studies separately according to the search strategy in three databases (PubMed, Embase, and the Cochrane Library). First, duplicated studies were removed. Next, the study type, title, and abstract were viewed to remove nonarticle and irrelevant studies. Finally, full-text was read to eliminate studies without sufficient data and low quality. When there was a dispute about whether a study should be included, a third author would make a decision based on the inclusion and exclusion criteria.
Quality assessment
The quality of studies was assessed by Newcastle-Ottawa Scales (NOS) score. 47 A score of 9 meant high quality, 7 to 8 meant medium quality, below 7 meant low quality.
Definition
Each complication was defined based on the Common Terminology Criteria for Adverse Events (CTCAE) V4.0, 48 and the grade was evaluated using the Clavien-Dindo (CD) classification. 11 If multiple postoperative complications occurred, the higher grade was used. Due to the common denominator of cancer related death, disease-specific mortality (DSM), cancer-specific survival (CSS), and disease-specific survival (DSS) were collectively referred to as CSS. Same to the common denominator of relapse, time to recurrence (TTR) and recurrence-free survival (RFS) were collectively referred to as RFS.
Data collection
As for the 29 included studies, the characteristics included the first author, published year, published country, study period, sample size, complication incidence, types of complications, CD grade, prognostic indicators, conclusion, and NOS score.
Complication types of all patients included were requested. In this study, patients were divided into the complication group (C group) and noncomplication group (NC group). The data of patients in each group included personal characteristics, comorbidity, pathological characteristics, and treatment characteristics. Personal characteristics included mean age, gender, American Society of Anesthesiologists (ASA) score, and Eastern Cooperative Oncology Group (ECOG) status. Comorbidity included diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular, and liver cirrhosis. Pathological characteristics included histological type, Lauren type, tumor location, tumor depth, lymph node status, and pathological stage. Treatment characteristics included adjuvant chemotherapy, neoadjuvant chemotherapy, surgical approach, surgical procedure, lymphadenectomy, and multivisceral resection. As for prognostic indicators, whether overall survival (OS), disease-free survival (DFS), TTR, RFS, DSM, CSS, or DSS were allowed.
Statistical analysis
This study focused most on patients' prognosis; therefore, hazard ratios (HRs) and 95% confidence intervals (CIs) were added to assess the impact of postoperative complication on different prognostic indicators. As for other characteristics, dichotomous variables were expressed as odds ratios (ORs) and 95% CIs; continuous variables were expressed as mean difference (MD) and standardized difference. I2 value and the chi-squared test were used to evaluate the statistical heterogeneity.49,50 Random-effect model was used as the default model, and P < .1 meant statistically significant. When I2 < 50%, the fixed-effect model was used, and P < .05 meant statistically significant. Stata V16.0 software was used for all of the data analyses.
Results
Study selection
After conducting the searching strategy, there were 11,220 studies (3861 in PubMed, 6263 in Embase, and 11 in the Cochrane Library). Three thousand nine hundred thirty-two studies were excluded for duplicates removed, 1009 studies were excluded for unqualified study type, and then, 2923 studies were left for record screening. After browsing the titles and abstracts, full-texts of 40 studies with relevant content were read. Finally, 29 studies17–45 with sufficient data were included in this study (Fig. 1).
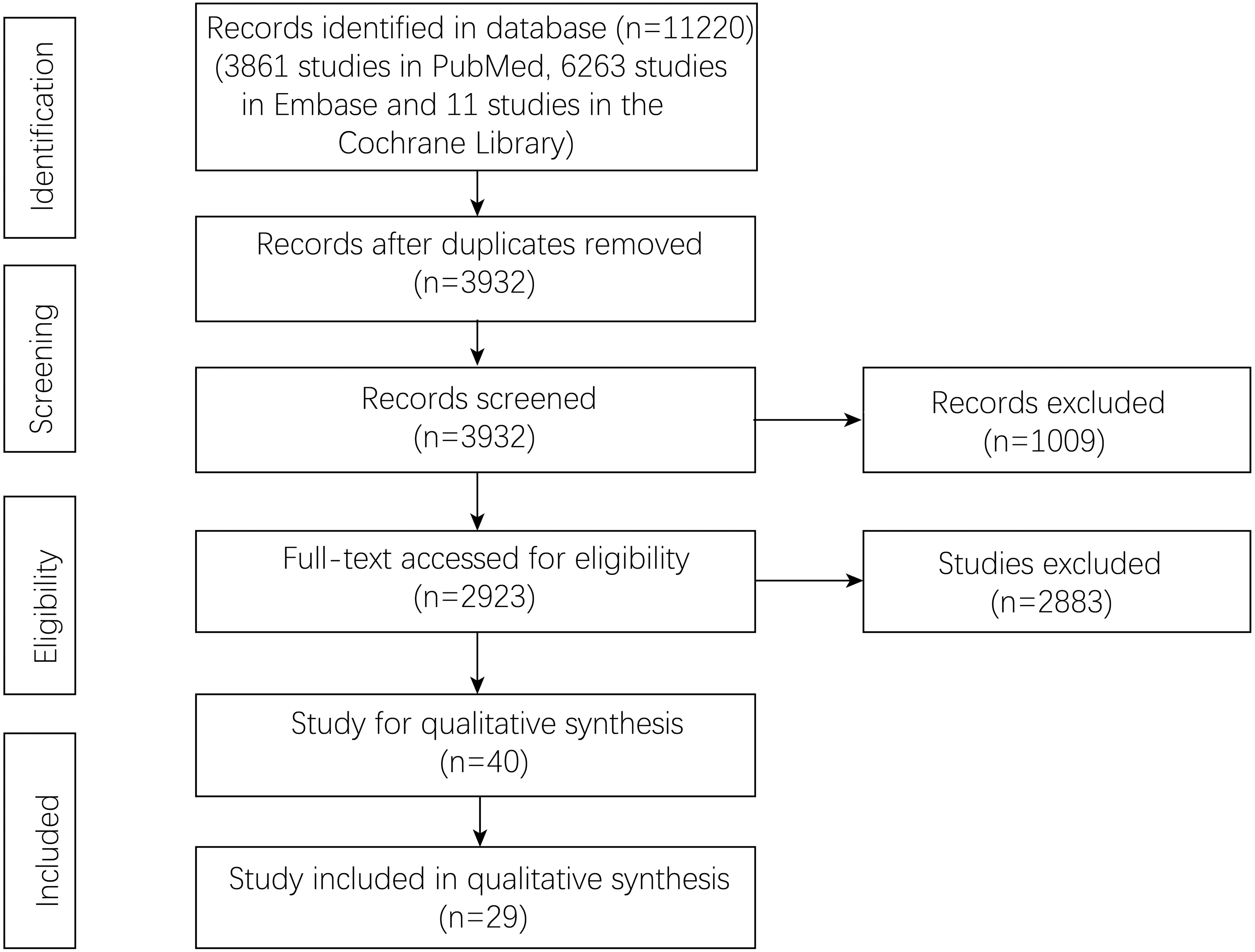
Flowchart of study selection.
Baseline characteristics of studies
This pooling up analysis included a total of 33,858 patients from 29 studies. The published time ranged from 2013 to 2022. Among the 29 studies, 13, 9, and 2 studies were published from Japan, China, and South Korea, respectively. Incidence of complications varied from 5.0% to 59.8%. Prognostic indicators that included OS, DFS, TTR, RFS, DSM, CSS, and DSS were reported from 23, 4, 1, 9, 1, 4, and 2 studies, respectively. More characteristics, including the first author, study period, sample size, complication types, CD grade, conclusion, and NOS score, are shown in Table 1.
Baseline Characteristics of Included Studies
CD, Clavien-Dindo; CSS, cancer-specific survival; DFS, disease-free survival; DSM, disease-specific mortality; DSS, disease-specific survival; GC, gastric cancer; IAC, intra-abdominal complication; IAIC, intra-abdominal infectious complications; IC, infectious complications; NA, not applicable; NOS, Newcastle-Ottawa Scales; OS, overall survival; PC, postoperative complication; RFS, recurrence-free survival; TTR, time to recurrence.
Types of complications
After summarizing complications of all included patients, intra-abdominal abscess was the most common complications for 774 patients (19.4%). Six hundred seventy-nine (17.0%), 655 (16.4%), 356 (8.9%), and 313 (7.9%) patients suffered from anastomotic leakage, pneumonia, complicated fluid collection, and pancreatic fistula, respectively. Other postoperative complications such as pancreatitis, wound infection, cardiac complications, bleeding, and so on are shown in Table 2.
Summary of Complications
Baseline characteristics of patients in the C group and NC group
After pooling up the OR, MD, and 95% CIs, the patients in the C group were older (MD = 2.75, I2 = 80.14%, 95% CI = 0.47–5.04, P = .02) and had more males (OR = 1.61, I2 = 66.01%, 95% CI = 1.36–1.90, P = .00) and more ASA score ≥3 (OR = 2.28, I2 = 78.25%, 95% CI = 1.60–3.24, P = .00) than in the NC group. Tumor location was higher in the C group with less middle third located tumor (OR = 0.44, I2 = 0.00%, 95% CI = 0.37–0.53, P = .00) and lower third located tumor (OR = 0.47, I2 = 0.00%, 95% CI = 0.39–0.56, P = .00). Tumor stage was more advanced in the C group with more T2 (OR = 1.42, I2 = 34.57%, 95% CI = 1.02–1.98, P = .04), T3 (OR = 2.24, I2 = 21.01%, 95% CI = 1.75–2.87, P = .00), and T4 stage (OR = 2.38, I2 = 62.66%, 95% CI = 1.60–3.53, P = .00), more N2 (OR = 1.47, I2 = 57.59%, 95% CI = 1.10–1.97, P = .01) and N3 stage (OR = 1.60, I2 = 52.66%, 95% CI = 1.23–2.08, P = .00), more Tumor Node Metastasis (TNM) II (OR = 1.41, I2 = 76.44%, 95% CI = 1.09–1.83, P = .01) and III stage (OR = 1.76, I2 = 64.86%, 95% CI = 1.46–2.12, P = .00), and more patients received neoadjuvant therapy (OR = 1.47, I2 = 0.00%, 95% CI = 1.06–2.05, P = .02). The C group had less patients who underwent laparoscope surgery (OR = 0.76, I2 = 77.41%, 95% CI = 0.60–0.98, P = .04) and total gastrectomy (OR = 0.54, I2 = 83.46%, 95% CI = 0.44–0.66, P = .00); more patients accepted lymphadenectomy ≥D2 (OR = 1.76, I2 = 83.22%, 95% CI = 1.13–2.74, P = .01) and multivisceral resection (OR = 2.36, I2 = 93.99%, 95% CI = 1.16–4.79, P = .02) than the NC group. There was no significant difference in other characteristics, including ECOG status, comorbidities, histological type, Lauren type, N0 stage, and adjuvant chemotherapy between the two groups (Table 3).
Summary of Characteristics Between C Group and Noncomplication Group
ASA, American Society of Anesthesiologists; C, complication; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ECOG, Eastern Cooperative Oncology Group; MD, mean difference; NC, noncomplication; OR, odds ratio.
OS of complication
After pooling up the HRs and 95% CIs, postoperative complication was found to be an independent prognostic factor for OS (HR = 1.52, I2 = 1.14%, 95% CI = 1.42–1.61, P = .00) for GC patients (Fig. 2).

Overall survival of postoperative complications.
DFS, DSS, and RFS of complication
For other prognostic indicators, postoperative complication still had a prognostic value for DFS (HR = 1.71, I2 = 0.00%, 95% CI = 1.44–1.98, P < .05), DSS (HR = 1.60, I2 = 54.58%, 95% CI = 1.26–1.93, P < .1), and RFS (HR = 1.26, I2 = 0.00%, 95% CI = 1.11–1.41, P < .05) (Fig. 3).
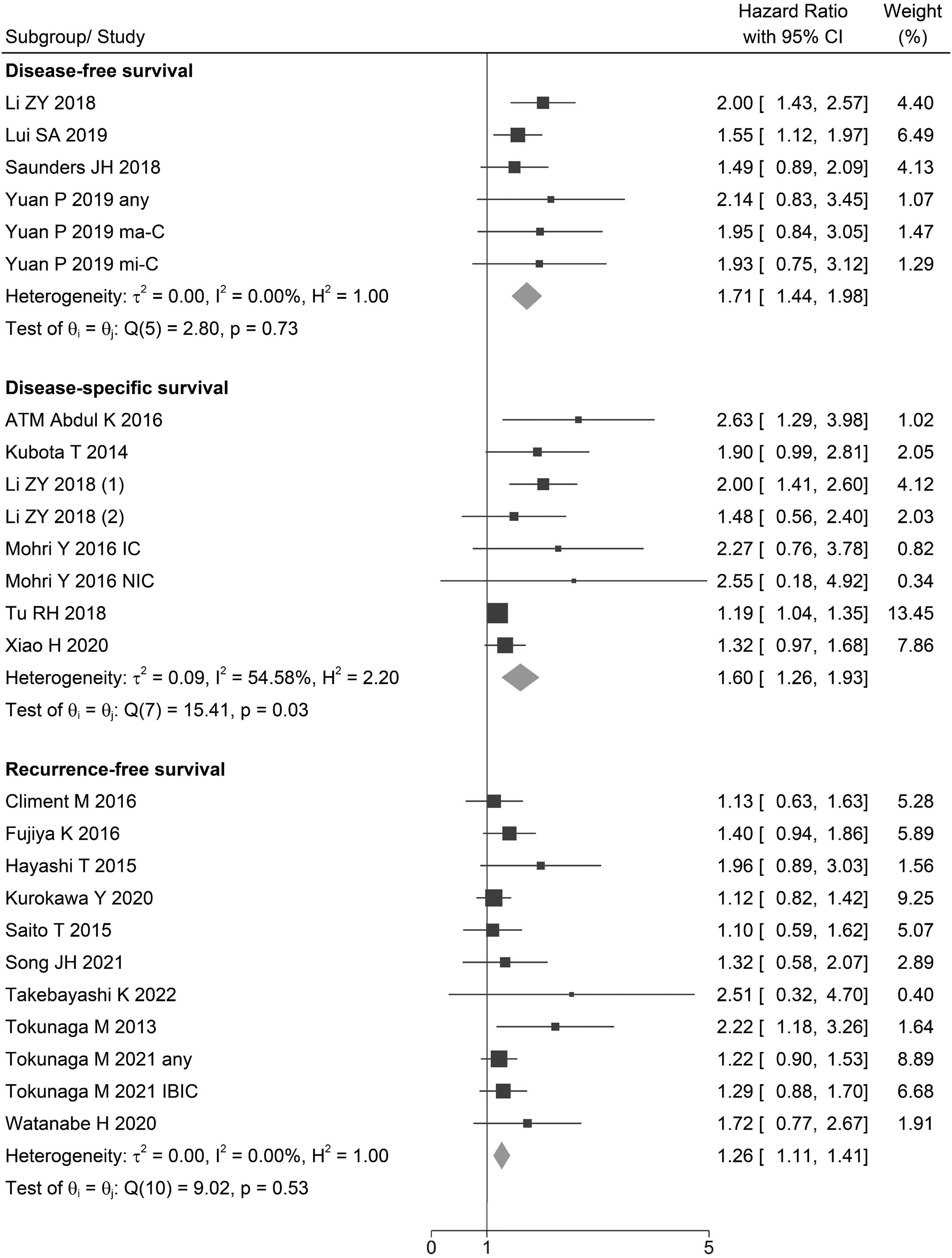
Other survival values, including disease-free survival, disease-specific survival, and recurrence-free survival of postoperative complications.
OS of complication classifications
All included studies were divided into four groups according to the definition of postoperative complications. Of the studies, 16, 9, 2, and 2 reported any complications, infectious complications, noninfectious complications, and other complications, respectively. After subgroup analysis, infectious complications still increased the risk of OS for GC patients (HR = 1.52, I2 = 0.00%, 95% CI = 1.34–1.69, P < .05). However, noninfectious complication was found to have no relationship with OS (HR = 1.39, I2 = 0.00%, 95% CI = 0.96–1.82, P > .05) (Fig. 4).
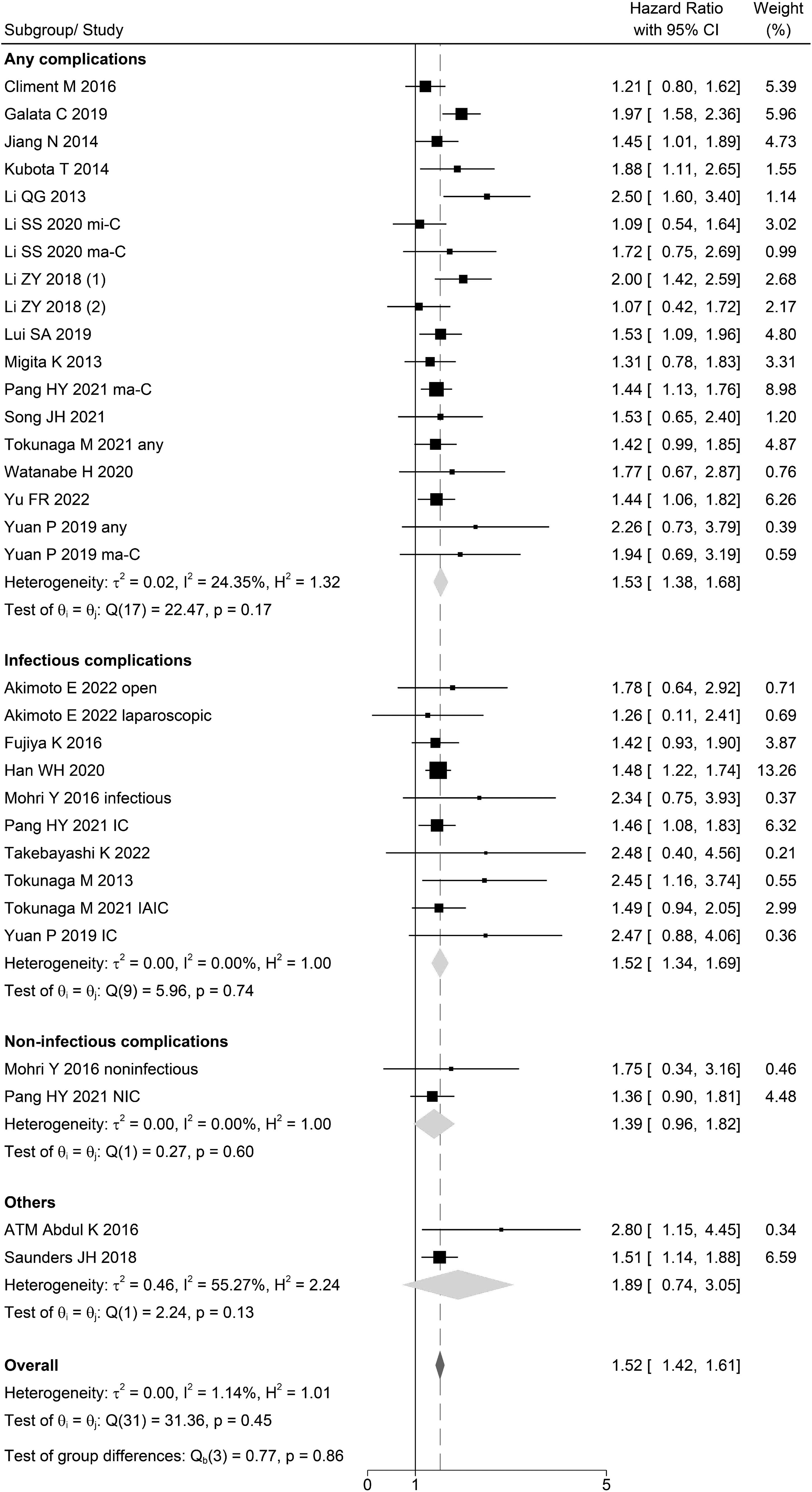
Subgroup analyses based on complication types for overall complications.
Sensitivity analysis
Each study was excluded at a time for sensitivity analysis, and there was no significant difference between every outcome.
Discussion
The present study enrolled a total of 29 studies involving 33,858 patients for analysis17–45 and showed that postoperative complication adversely affected long-term outcomes after radical surgery for GC patients. Complication was an independent prognostic factor for all survival indicators, including OS, DFS, DSS, and RFS. However, further analysis found that noninfectious complications were not significantly associated with OS, while infectious complications still had a prognostic value.
Postoperative complication could decrease the OS and DFS in several cancers, including lung cancer, breast cancer, and colorectal cancer.51–53 In particular, infectious complications such as wound infection and anastomotic leakage was associated with increased recurrence after breast cancer surgery and colon cancer surgery, respectively.54–56 However, infectious complications were reported to decrease recurrence rate and lead to regression in head and neck cancers.57,58
The impact of postoperative complication for GC patients undergoing surgery was also of concern. Some studies reported that infectious complication was a risk factor for recurrence and survival.18,22,23 And more studies showed that overall complication had a negative impact on prognosis after radical resection,24,25,27,28,30,31 even the negative effects increased with higher CD grades. 29 However, some other studies revealed that complication was not a reliable indicator of survival; its impact might be weak.17,19,26,32,35 Galata C analyzed GC patients during a period of 42 years and concluded that postoperative complication influenced OS due to complication-related early postoperative deaths; it was not a risk factor for patients successfully rescued from early postoperative complications. 21 Therefore, the prognostic role and potential mechanisms of postoperative complication in predicting the prognosis of GC patients were unclear.
Based on the current study, we hypothesized that postoperative complications, especially infectious postoperative complications, that resulted in worse prognosis and higher GC recurrence might be due to the following several mechanisms. It was proofed that the excessive surgical stress might increase the levels of inflammatory cytokines such as interleukin-6, and the inflammatory response would cause aggravated postoperative complications.59–62 Otherwise, the inflammation after surgery could suppress cell-mediated immunity responses, particularly by impairing natural killer cells and cytotoxic T lymphocytes, that promoted the cancer cells' growth and metastasis.63,64 Meanwhile, the occurrence of inflammatory complication, especially intra-abdominal infections, produced excessive catecholamine and prostaglandin, which also adversely affected the immune system and contributed to metastatic and worse outcomes. 65 Furthermore, infectious postoperative complication could activate the processes of bacterial antigen mediated; the inflammatory cytokines would lead to the adhesion of circulating cancer cells to vascular endothelium of distant organs, then directly affect the metastasis of cancer cells.66,67
Based on the above mechanisms, we recommended that surgeons developed a multimodality approach for patients preoperatively, 68 made efforts to minimize intraoperative blood loss and transfusions intraoperatively,69,70 and actively provided nutritional support70,71 and correcting hypoproteinemia 72 perioperatively. These measures might help to reduce the incidence of postoperative complications, further improved patient prognosis, and reduced postoperative recurrence.
To our knowledge, this was the first study that pooled up all the previous studies on the relationship between postoperative complication and GC patients' survival. The results were reliable with a large sample size and little heterogeneity. Furthermore, subgroup analysis identified infectious complication as a major prognostic risk factor. Meanwhile, there were some limitations in this study. First, subgroup analysis of more refined types of complications was lacking due to the insufficient data. Second, complications of different CD classifications might have different impact. Third, a majority of the included studies were published in Asian countries, which might lead to a bias. Therefore, more western countries studies on the influence of different CD grades and different types of complications for GC patients were needed.
In conclusion, GC patients with postoperative complication had a worse prognosis than those without postoperative complication, and the survival disadvantage seemed to be mainly driven by infectious complications rather than noninfectious complications. Thus, it was important to prevent postoperative complications, especially infectious complications.
Footnotes
Acknowledgments
We acknowledge all the authors in this article.
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by L-F.R. and Y-H.X. The first draft of the article was written by L-F.R., the final draft of the article was written by J-G.L., and all authors commented on previous versions of the article. All authors read and approved the final article.
Ethics Approval
The current study was conducted in accordance with the PRISMA statement.
Data Availability Statement
The data were accessed from the database.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.