
Abstract
Introduction:
Percutaneous endoscopic biliary lithectomy (PEBL) can be performed through preexisting drain tracts, offering ductal clearance and definitive management for patients with complicated gallstone disease unable to undergo conventional therapy. The technique has not been widely adopted by general surgeons. Herein, we describe our technique with surgeon-performed PEBL and present initial results.
Materials and Methods:
A single institutional retrospective review of the electronic medical record was performed for patients who underwent percutaneous choledochoscopy between February 2019 and November 2020. All operations were performed by 1 of 2 board-certified general surgeons with fellowship training in surgical endoscopy. Preoperative, operative, and postoperative variables were analyzed using descriptive statistics.
Results:
Thirteen patients underwent PEBL. Seventeen total procedures were performed; 4 patients underwent repeat intervention. The diagnoses leading to PEBL were: cholelithiasis (8), choledocholithiasis (4), and recurrent pancreatitis (1). Complete ductal clearance was achieved in 9 patients (69.2%) during the initial procedure. The remaining 4 patients (30.8%) underwent repeat PEBL, at which point complete ductal clearance was then achieved. The percutaneous drain was removed at the time of final procedure in 5 patients (38.5%) or within 5 weeks in the remaining 8 (61.5%). No intraoperative complications occurred, and no pancreatic or biliary postoperative complications or recurrences were noted with a mean follow-up of 279 ± 240 days.
Conclusion:
Surgeon-performed PEBL is a safe and effective method of achieving biliary ductal clearance. The technique is readily achieved following basic endoscopic and fluoroscopic principles and should be understood by all physicians managing gallstone disease.
Introduction
Significant provider-dependent variations exist in the management of obstructive biliary processes, including gallstone disease. Endoscopic retrograde cholangiopancreatography (ERCP) followed by cholecystectomy has shown reliable success in the management of choledocholithiasis and represents the common final pathway for the majority of complicated gallstone disease. Although less commonly performed, laparoscopic common bile duct exploration (LCBDE) represents an alternative to ERCP. Numerous contraindications for these procedures exist, including medical conditions precluding anesthetic use and altered/difficult surgical anatomy. For patients with complicated gallstone disease and contraindications to conventional management, their management often involves percutaneous biliary drainage.
Despite extensive comparisons of the efficacy, safety, and cost between conventional therapeutic options (ERCP and LCBDE), the management of patients undergoing alternative therapy for complicated gallstone disease such as percutaneous biliary drainage is far less studied and, consequently, less standardized. For some patients, biliary drainage represents a bridging therapy until they can tolerate a conventional therapeutic option. For others, however, the intervention represents destination therapy which can require lifelong drainage and multiple tube exchanges over time. Percutaneous biliary interventions can be performed through these preexisting drain tracts, offering reliable ductal stone clearance and definitive management to some patients. These procedures, often performed by interventional radiologists (IR), include cholangiography, internal and external drainage, stent placement, and biliary stone retrieval. 1
Biliary endoscopy, or choledochoscopy, can also be performed percutaneously and offers a minimally-invasive approach to bile duct clearance. Percutaneous endoscopic biliary lithectomy (PEBL) was originally demonstrated in the 1980s,2–4 and since that time, small case series demonstrating success of the intervention have periodically appeared in the literature.5–10 In 2021, Stirrat et al. reported on 75 patients who underwent the technique, with a complete gallstone removal rate of 90.7% and only 3.9% of patients requiring cholecystectomy in the follow-up period. 11 Despite these documented successes, the technique has not been widely adopted by general surgeons, and many patients are left to endure the morbidity of a percutaneous biliary drain for prolonged periods of time. It is, therefore, the goal of this article to present our initial results with the technique, demonstrate the technical principles of performing PEBL, and define how this intervention can be incorporated into the algorithm of any modern minimally-invasive surgeon.
Materials and Methods
Data collection
A single institutional retrospective review of the electronic medical record was performed for patients who underwent percutaneous choledochoscopy between February 2019 and November 2020. All operations were performed by 1 of 2 board-certified general surgeons with fellowship training in surgical endoscopy at an academically-affiliated tertiary referral center. Institutional review board approval was approved before data collection. Preoperative, operative, and postoperative variables were collected and analyzed using descriptive statistics. Our patient selection and procedural details are detailed below.
Patient selection
Percutaneous choledochoscopy can be considered in any patient with a biliary drainage catheter in place. In our practice, we have successfully used the intervention on patients with numerous types of biliary drains, including percutaneous cholecystostomy catheters (PCCs), percutaneous transhepatic biliary catheters (PTCs), and even intra-abdominal drains placed near a remnant gallbladder stump. Regardless of catheter type, the diameter of the catheter must be at least 12F or larger to accommodate the choledochoscope or ureteroscope. Patients with smaller drains in place generally require intervention for tube upsizing before choledochoscopy. Alternatively, a dilating sheath can be utilized to upsize the tract during the procedure. We generally wait to perform the initial PEBL until after the first drain exchange or upsizing has occurred, typically 6–8 weeks after initial placement.
At our institution, the most common use of PEBL is to scope the biliary tract through a PCC. Certainly, not every patient with a PCC in place should undergo choledochoscopy. Many patients successfully undergo cholecystectomy after resolution of their critical illness, obviating the need for prolonged biliary drainage. However, in patients with medical or surgical contraindications to cholecystectomy, direct scoping of the gallbladder can provide complete stone clearance and allow for drain removal. In these cases, the entire biliary system can be accessed through the cystic duct, which can be dilated if needed.
Recently, other methods of minimally invasive gallstone management—including endoscopic ultrasound-guided gallbladder drainage (EUSGBD) and endoscopic transpapillary gallbladder drainage (ETGBD)—have been introduced as alternatives to percutaneous gallbladder drainage in patients with cholecystitis whose surgical risk precludes cholecystectomy. 12 While both procedures offer the promise of internal biliary drainage, it should be noted that these procedures are complex and rarely performed outside of tertiary care centers. Therefore, PCC followed by choledochoscopy and drain removal remains a viable option for the majority of these patients.
Although performed less commonly, scoping the biliary tract through a PTC (generally placed into a right posterior duct as per the preference of interventional radiology) can also have a therapeutic role. Most of these patients have transhepatic biliary catheters in place because they were not candidates for, or had failed, ERCP attempts and required management of a complication of gallstone disease, including cholangitis, choledocholithiasis, or recurrent pancreatitis. With a PTC in place, these patients were then referred to a surgeon for consideration of cholecystectomy. In these cases, percutaneous choledochoscopy is then used for patients who are unfit for cholecystectomy or who require ductal clearance before cholecystectomy.
Overall, it should be noted that there is not one common pathway or indication that leads patients to undergo PEBL. As noted above, there are a great number of acceptable therapeutic options for the management of gallstone disease, and clinical algorithms are varied accordingly among providers. However, it is abundantly clear that a subset of patients with medical and surgical contraindications to more conventional interventions can benefit from PEBL.
Even more noteworthy is the paucity of contraindications to the procedure. Although the procedure is usually performed using conscious/moderate sedation, we have performed the procedure without any anesthetics in a patient with an absolute anesthetic contraindication while maintaining patient comfort. In addition, the procedure can be performed safely without disruption in patients' anticoagulation or antiplatelet regimens. Finally, with slight variations in technique, PEBL can be utilized in cases without limitation on size or number of gallstones. Given its applicability to high-risk patients who lack therapeutic alternatives and its minimal contraindications, the ability to incorporate and perform PEBL in a modern general surgeon's practice is advantageous.
Operative details
PEBL should be performed in an operative suite equipped with endoscopic and fluoroscopic equipment, and enough monitors to allow comfortable viewing of both screens at once (Fig. 1). The patient should be placed in a supine position. After induction of anesthesia, the first essential step is a tube cholangiogram. In this study, the surgeon evaluates the anatomy of the biliary tract and surveys the tract for filling defects (Fig. 2). Following initial cholangiogram, a wire is placed through the drain, down the drain tract under fluoroscopic guidance until it loops within the gallbladder or duodenum, depending on where the original drain was terminated. A Cope loop, if present, must be released to facilitate wire passage. With the wire in place, the drain is then removed from the tract (Fig. 3A).

Room setup for percutaneous biliary lithectomy requires easy visualization of monitors for fluoroscopic and endoscopic views.
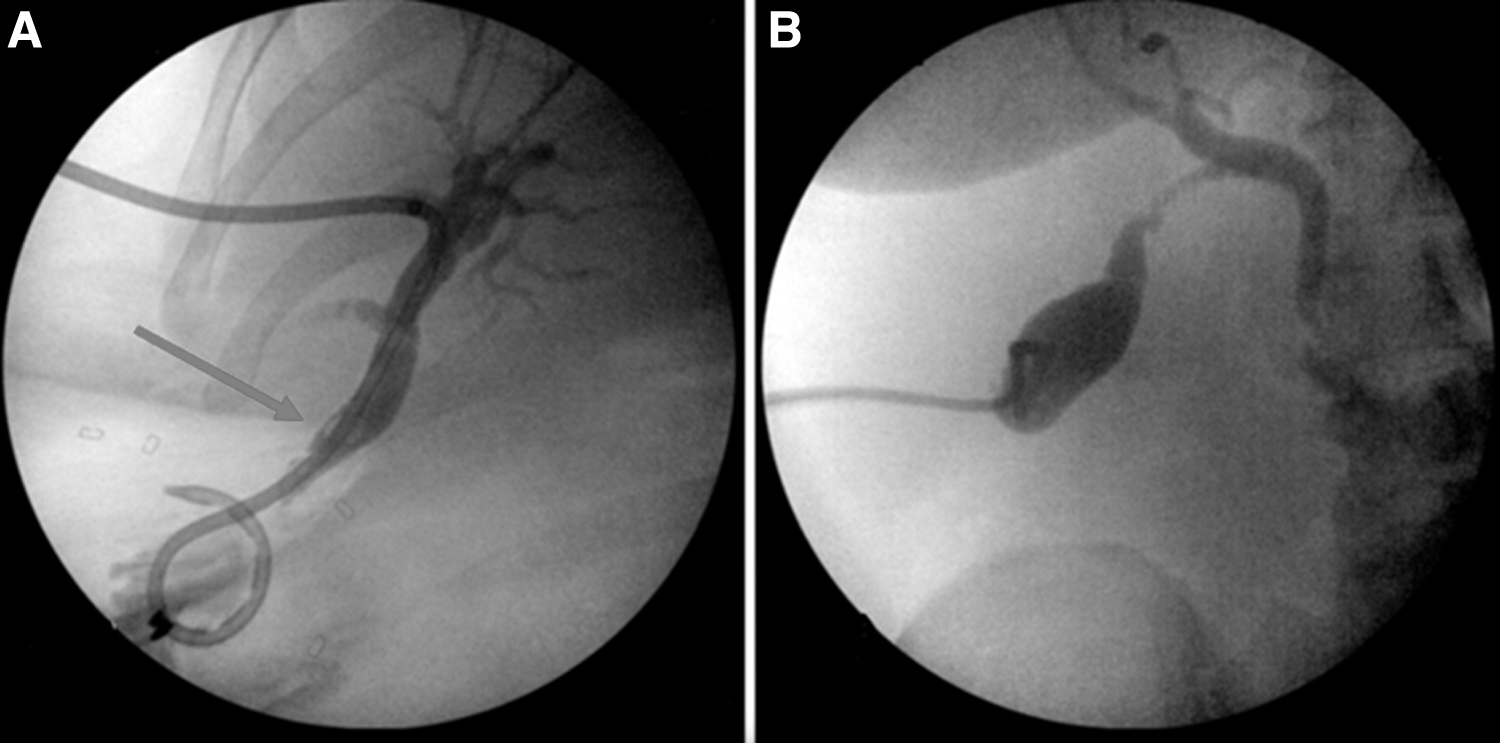
Cholangiogram through a percutaneous transhepatic biliary drain, demonstrating a dilated common bile duct and distal filling defect (arrow)
A percutaneous transhepatic biliary tube is removed over a wire, which is coiled in the duodenum
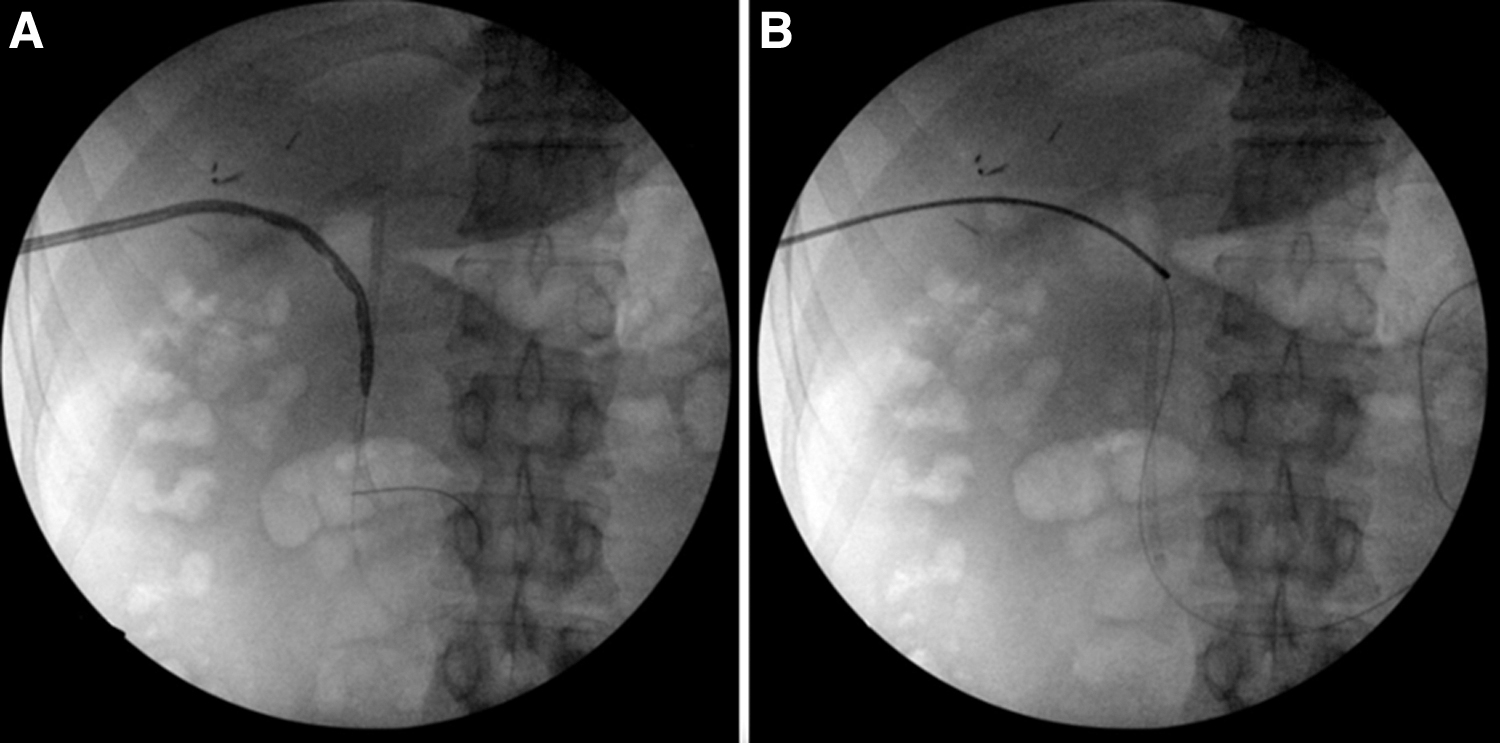
Next, a digital ultraslim ureteroscope or choledochoscope is passed over the wire (Fig. 3B). Recently, we have utilized disposable choledochoscopes (SpyGlass DM; Boston Scientific, Natick, MA) with good success. Gentle saline irrigation is used to navigate the scope through the biliary tree (Fig. 4). The scope can be directed to evaluate both the right and left ductal systems and can be navigated down the common hepatic duct (Fig. 5A, B). Fluoroscopy is essential for maintaining orientation during these maneuvers. The junction of the cystic duct can be visualized and assessed for bile outflow. Finally, the scope can be passed down the common bile duct, through the ampulla of Vater, and into the duodenum. Caution must be used at this stage to avoid disrupting any internalized stents, if present, and passage into the duodenum is not mandatory (Fig. 5C).

The ureteroscope or choledochoscope is passed through the percutaneous drain tract. Saline is gently irrigated through the working channel of the scope to allow for visualization.
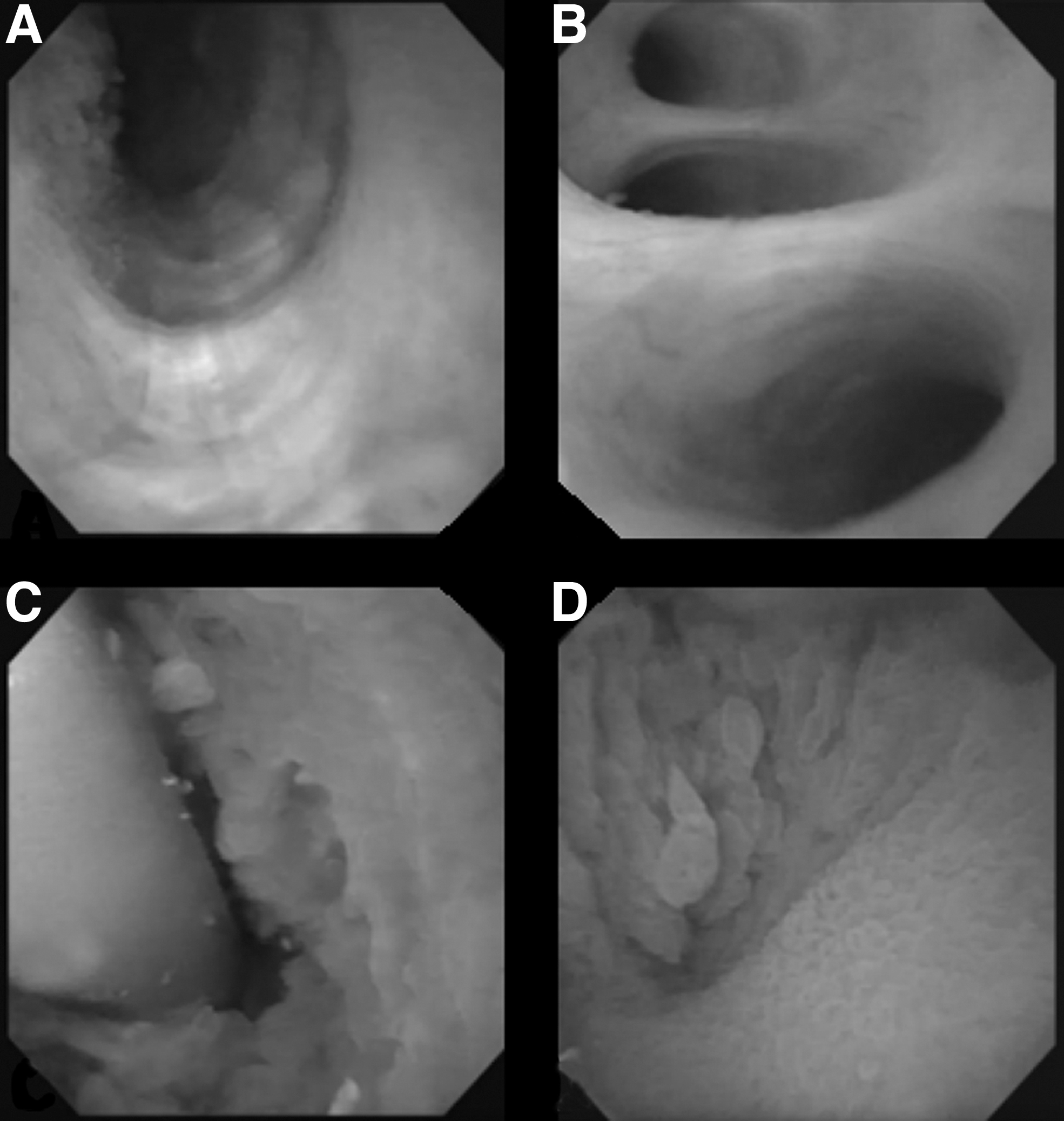
Endoscopic view of the common bile duct
When scoping through a percutaneous cholecystostomy tube, the initial steps are the same as previous. Starting with a cholecystogram, the cope loop (if present) is released and a wire is placed through the drain and coiled in the gallbladder. The drain is removed, and the scope is then advanced down over the wire into the gallbladder. At this point, if the tract is well established, you can either remove the wire or scope alongside the wire through the tract. Access into the biliary tree is achieved by careful passage through the cystic duct and past the valves of Heister. This is facilitated by directing the scope into the cystic duct, and then under endoscopic and fluoroscopic guidance, advancing a wire down the scope, through the cystic duct and through the common bile duct, terminating in the duodenum.
With the wire in place the scope can then be advanced over the wire, or if the duct is too small or tortuous, the cystic duct can be dilated by removing the scope and passing a balloon over the wire and dilating fluoroscopically until the duct can accommodate the scope. The biliary tract should be carefully inspected for gallstones, debris, or sludge. In addition, careful inspection of the mucosa for irregularities is important to rule out a mass lesion as a source of biliary obstruction (Fig. 5D).
If identified, the next step of the procedure should be directed at removing gallstones from the biliary system (Fig. 6). If feasible, the easiest method is to push small stones in an antegrade manner into the duodenum. Cycles of irrigation and aspiration of saline can also be used for smaller debris. For larger stones, basket removal is attempted next with a tipless Nitinol basket or biliary basket (Fig. 7). Given difficult approach angles and minimal working room within a duct, you can also pass the basket parallel to, rather than through, the scope in certain circumstances. The basket is advanced using fluoroscopic guidance in these cases. Mechanical lithotripter baskets, designed to crush gallstones, can also be used.
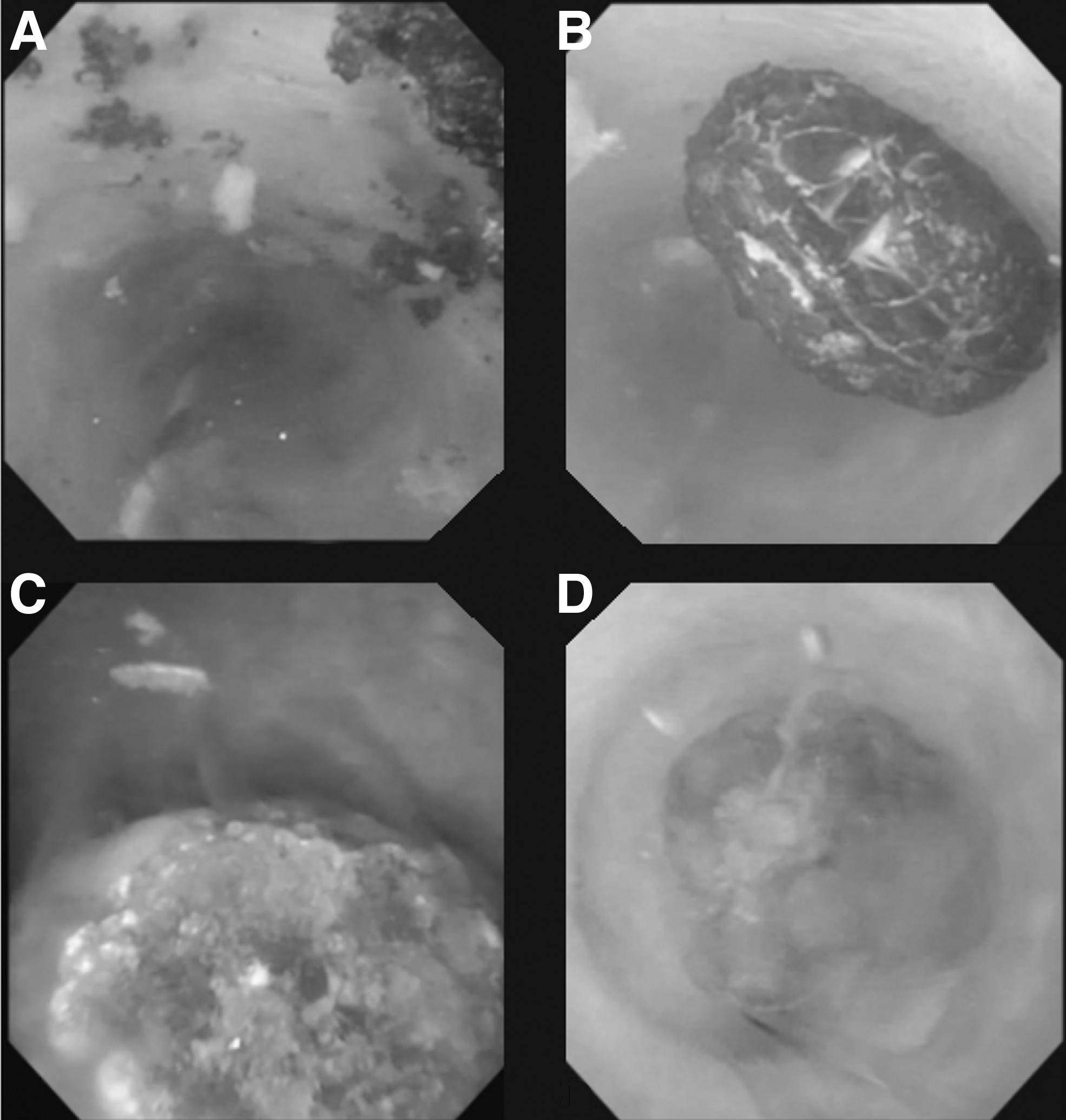
Small gallstone debris within the CBD
A biliary basket is placed around a gallstone
For stones that are too large for basket removal or positioned such that basket retrieval is impossible, laser lithotripsy or electrohydraulic lithotripsy is used. For laser lithotripsy, we use a Holmium laser and 275 μm fiber to fragment the stone into pieces amenable to basket retrieval (Fig. 8). For electrohydraulic lithotripsy, we utilize a single-use bipolar electrohydraulic lithotripsy device (Autolith Touch; Boston Scientific), starting on the lowest pulse and power settings and gradually increasing the settings until adequate stone fragmentation is achieved.
Laser lithotripsy is applied to a large gallstone.
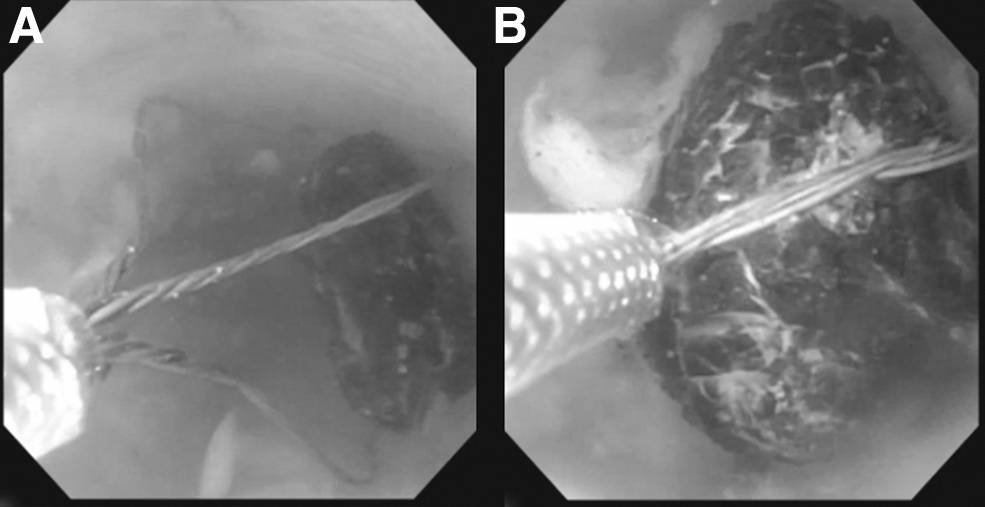
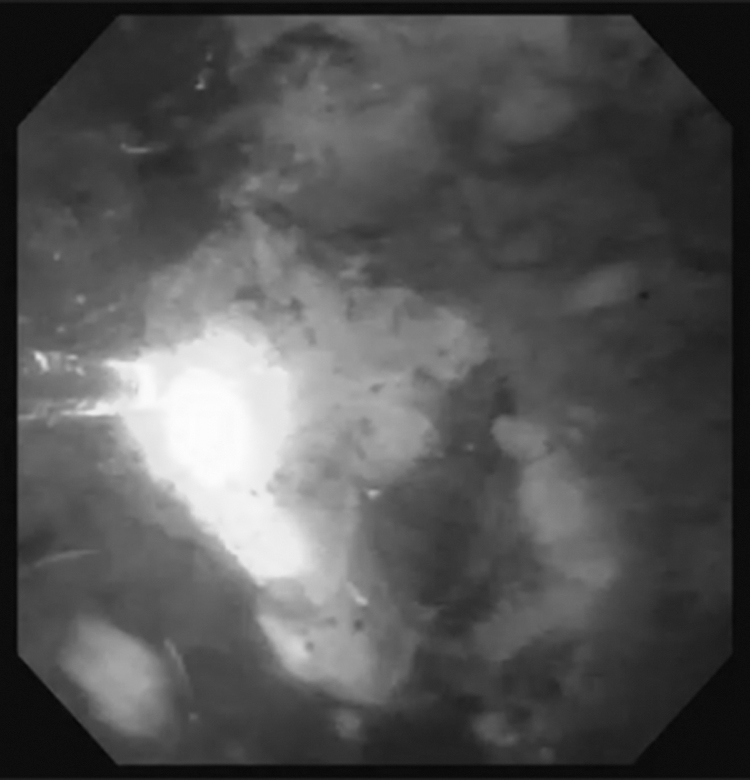
In our experience, we have found stone removal to be the most challenging aspect of this procedure but have identified several technical maneuvers which can aid in completion of this step. First, when the entire gallbladder has been filled with saline it can be difficult to capture the stones in a basket because the stones freely move about the gallbladder and evade even the most skilled endoscopist (Fig. 9A, B). Therefore, a helpful maneuver is to slowly suction out some of the saline within the gallbladder to create an air fluid level (Fig. 9C, D). Cholesterol stones will then float on this fluid level and can be more easily captured with a basket. Some larger stones may sink down into the gallbladder neck or fundus, depending on the positioning of the patient. If this occurs, the endoscopist can further suction down the fluid level which creates a funneling action that coalesces the stones in the dependent portion of the gallbladder (Fig. 10A–D). Patient positioning can be altered to orient the gallbladder neck in an inferior position; here, it is helpful to recall that the gallbladder is in its normal anatomical position with the fundus oriented inferiorly during this procedure, unlike the cranially-retracted surgical position in which most surgeons are accustomed to viewing the organ.

Small, free-floating gallstones can be difficult to grasp with an endoscopic grasper

Numerous, free-floating stones are seen in the neck of the gallbladder
For stones which are impacted within the infundibulum or cystic duct, we have utilized several techniques. First, a suction catheter can be placed over a wire and can be utilized to suction the stone from its location. Alternatively, if a wire can be placed distal to the stone, an ERCP balloon can be passed to perform a balloon sweep. Finally, after the stone or stone fragment has been captured in an endoscopic basket the task of removing a larger stone through the drain tract can represent another challenge. To assist in this process, we have found that while using a tipless Nitinol basket (Zero Tip Nitinol Stone Retrieval Basket; Boston Scientific) the basket can be loosely opened during removal such that the stone can freely settle into a configuration which allows removal.
Following stone removal, the entire biliary system should be copiously irrigated to flush any remaining debris or sludge. We then scope the entire biliary tree in a proximal to distal manner to confirm complete clearance. A completion cholangiogram is then performed through the ureteroscope (Fig. 11). Finally, the decision is made whether or not to replace an external drain through the tract. This decision is made by considering the adequacy of ductal clearance and risk for recurrence. The scope is then removed and either a drain is replaced through the tract over the wire using fluoroscopic guidance or the wire is removed, and the tract opening is dressed with dry gauze. Patients can be discharged the same day of the procedure without specific postoperative limitations. If a drain has been replaced, we generally schedule a tube cholangiogram in 4 weeks at which time the drain is removed if no further filling defects are visualized.

Postprocedural cholangiogram performed through the choledochoscope, showing no filling defects and contrast flow into duodenum.
Results
Thirteen patients underwent PEBL at our tertiary care institution between February 2019 and November 2020 (Table 1). Institutional review board exemption status was approved before data collection. Seventeen total procedures were performed; 4 patients underwent repeat intervention. All procedures were performed by a single board-certified surgeon trained in advanced endoscopy. A urologist with expertise in laser lithotripsy assisted on cases requiring laser use. Nine males (69.2%) and 4 females (30.8%) were included, with age range of 47–83 years (mean 61.2 ± 9). The primary diagnoses leading to PEBL were: cholelithiasis (8), choledocholithiasis (4), and recurrent pancreatitis (1). Seven patients (53.8%) had altered abdominal wall or gastrointestinal anatomy, and 6 (46.1%) patients had strict medical contraindications which limited conventional interventions (i.e., cholecystectomy, ERCP). Five patients had undergone ERCP attempts before PEBL, while only 3 (60%) had successful cannulation of the ampulla of Vater, and none achieved complete gallstone clearance.
Patients Undergoing Percutaneous Endoscopic Biliary Lithectomy
Represents total number of days after the initial PEBL, if more than one procedure was performed.
Drain was removed at the time of initial PEBL procedure.
CKD, Chronic Kidney Disease; HTN, hypertension; PEBL, percutaneous endoscopic biliary lithectomy; PTC, percutaneous transhepatic biliary catheter.
The mean number of days from initial presentation at our institution until PEBL was 161 ± 132, during which patients underwent a mean of 2.5 ± 0.7 (range 2–4) interventional radiology procedures for biliary drain placement, exchange, and upsizing. Access was achieved through percutaneous cholecystostomy tubes in 8 (61.5%) and percutaneous transhepatic biliary tubes in 5 (38.5%) patients. The mean operative time was 61 ± 40 minutes. Stone extraction was performed with baskets and graspers in all cases, and laser lithotripsy was used in 3 (21.1%) cases. Complete ductal clearance was achieved in 9 patients (69.2%) during the initial procedure. The remaining 4 patients (30.8%) underwent repeat PEBL at a mean of 28.5 ± 13 days after the initial PEBL, at which point complete ductal clearance was then achieved. The percutaneous drain was removed at the time of final procedure in 5 patients (38.5%) or within 5 weeks in the remaining 8 (61.5%). No intraoperative complications occurred, and no pancreatic or biliary postoperative complications or recurrences have been noted with a mean follow-up of 279 ± 240 days.
Discussion
Surgeon-performed PEBL can be used with reliable technical success. The application of standard endoscopic and surgical principles to the percutaneous endoscopic management of gallstone disease has led to safe, minimally-invasive interventions as demonstrated in our series and others.7,8,11 Larger data series are necessary to evaluate long-term outcomes of surgeon-performed PEBL. At least one multi-institutional study is currently collecting these data. In our series, each patient facing the daunting prospect of lifelong external biliary drainage due to a wide range of contraindications to conventional therapy achieved ductal clearance and percutaneous drain removal—much to their enthusiastic appreciation.
All surgeons who treat gallstone disease in their practice should have knowledge of PEBL; the intervention can be safely learned by any surgeon with proper endoscopic and fluoroscopic skills and applied to a specific population of patients without proven alternative therapies. The procedure can be learned with a short learning curve which focuses on the proper utilization of equipment and performed with fairly limited resources which are available in most standard operating rooms. Surgeons without the necessary training or resources to perform PEBL should refer to a center capable of completing the intervention.
As the therapeutic modalities for gallstone disease continue to evolve, surgeon-performed PEBL will require continued study. EUSGBD and ETGBD have been suggested as alternatives to percutaneous biliary drainage, particularly in cases of cholecystitis, for long-term minimally-invasive biliary decompression. Comparisons of cost, safety, and efficacy between these techniques versus percutaneous drainage followed by PEBL are important and will require larger series of patients than have previously been published. Because, in part, the technique has not had widespread adoption by general surgeons, current understanding of the technique comes from smaller series.
Percutaneous biliary interventions have been adopted and published more widely by IR; however, percutaneous endoscopic techniques, in particular, fall well within the realm of general surgery. Incorporation of the technique by more surgeons may lead to more comprehensive streamlined care. Notably, patients in our series underwent multiple IR procedures over a prolonged time course before definitive therapy with PEBL was achieved. Wider understanding of—and earlier referral for—PEBL may allow for more efficient definitive management of gallstone disease in these patients.
Conclusion
Surgeon-performed PEBL is a safe and effective method of achieving biliary ductal clearance in patients suffering from complicated gallstone disease who are unable to undergo conventional management. The technique is readily achieved following basic endoscopic and fluoroscopic principles and should be understood by all physicians managing gallstone disease.
Footnotes
Disclosure Statement
C.G.D.: nothing to disclose. J.S.W.: consultant: Boston Scientific Corp. E.M.P.: speaking/teaching: Cook Biotech, Inc., C.R. Bard, Inc., Boston Scientific Corp. Ovesco; research support: C.R. Bard, Inc.; consultant: Boston Scientific Corp., Actuated Medical, Inc., Medtronic, Baxter, Surgimatrix, CMR Surgical; royalties: UpToDate, Inc., Springer.
Funding Information
No funding was received for this article.