
Abstract
Background:
Esophageal submucosal tumors (SMTs) are rare, occurring in less than 1% of esophageal neoplasms. For surgical treatment of esophageal SMTs, enucleation is usually the procedure of choice for benign tumors. This study aimed at evaluating the surgical technique and outcomes of thoracoscopic enucleation with esophagoscopy for esophageal SMTs.
Methods:
Patients with esophageal SMTs who underwent thoracoscopic enucleation between 2015 and 2022 were retrospectively investigated. Surgery was performed with the patient in the prone position. First, an esophagoscope was inserted, and a sodium hyaluronate solution with indigo carmine dye was injected into the submucosal layer just below the tumor. Next, under thoracoscopy, the tumor was exposed through a thoracoscopic incision and dissection of the muscularis propria and adventitia was performed at the tumor site. The colored layer resulting from the previously injected dye was identified, and tumor enucleation was performed under guidance of the dye so as not to damage the mucosa or pseudocapsule.
Results:
In total, 5 surgeries were performed. The mean operative time was 122.6 minutes (range 84–168 minutes), mean blood loss was 21.1 mL (range 0–80 mL), and mean postoperative hospital stay was 8 days (range 7–10 days). There were no postoperative complications. Pathological diagnosis revealed 2 cases of gastrointestinal stromal tumors, 2 cases of schwannoma, and 1 case of leiomyoma.
Conclusions:
We believe that this technique is a useful and safe method of performing thoracoscopic enucleation of esophageal SMTs because the injected dye provides an indicator of the resection line during enucleation.
Introduction
Esophageal submucosal tumors (SMTs) are rare, occurring in less than 1% of esophageal neoplasms. 1 Although there are a variety of esophageal SMTs, including schwannomas and gastrointestinal stromal tumors (GISTs) with malignant potential, leiomyomas account for about 70% of all of these tumors. 2 Esophageal GISTs are extremely rare and account for less than 2% of all gastrointestinal GISTs. 3 The preoperative diagnosis of esophageal SMTs greatly influences the choice of surgical technique, so the histological diagnosis, including immunostaining following preoperative endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB), is important. The surgical indications for esophageal SMTs depend on the grade of malignancy and the presence of symptoms. 4
Surgical treatment for esophageal SMTs includes enucleation and esophagectomy, but for benign tumors such as leiomyomas, enucleation with preservation of the esophagus is the procedure of choice, and in recent years there have been increasing reports of minimally invasive surgery performed via a thoracoscopic approach. 5
In contrast, esophageal GISTs with malignant potential may require more invasive esophagectomy. However, recent reports suggest that enucleation of primary esophageal GISTs may be recommended in patients with small tumors or in low-risk groups. 5
We have performed thoracoscopic enucleation of esophageal SMTs with esophagoscopy with the patient in the prone position and report on the surgical technique and surgical outcomes.
Methods
In our hospital, we retrospectively investigated 5 patients with esophageal SMTs who underwent thoracoscopic enucleation with esophagoscopy in the prone position between 2015 and 2022. The clinical characteristics of patients are shown in Table 1. Their mean age was 60.6 (range, 54–67) years. Tumor localization was the middle thoracic esophagus in 4 patients and lower thoracic esophagus in 1 patient. The mean tumor diameter was 27.8 mm (range, 16–40 mm).
Clinical Characteristics of Patients with Esophageal Submucosal Tumors
EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy; GIST, gastrointestinal stromal tumor.
All patients underwent preoperative EUS-FNAB to obtain a preoperative diagnosis. Two patients had GIST (1 low risk, 1 very low risk), 2 had schwannoma, and 1 had leiomyoma. This study was approved by the institutional review board of St. Marianna University School of Medicine bioethics committee (approval number: 6117), and the need for informed consent was waived as it was a retrospective study with data analyzed anonymously. All procedures were performed in accordance with relevant guidelines and regulations.
Surgical technique
Surgical position
Single-lung ventilation with bronchial blockers was used for general anesthesia, with the patient positioned prone and the right upper arm elevated. The surgeon and scopist performed the procedure standing on the patient's right side.
Thoracoscopic enucleation with esophagoscopy
Three ports (5, 12, and 12 mm) were inserted on the middle axillary line between the right fourth intercostal space, right sixth intercostal space, and right eighth intercostal space, respectively. The three thoracoscopic ports were placed under artificial CO2 pneumothorax (CO2 pressure 8 mmHg).
First, an esophagoscope was inserted to identify the tumor. Under esophagoscopy, a sodium hyaluronate solution (MucoUp®; Boston Scientific, Tokyo, Japan) with indigo carmine dye was injected into the submucosal layer just below the tumor (Fig. 1). Next, after confirming the esophageal SMT under thoracoscopy (Fig. 2a), the mediastinal pleura of the tumor area was incised longitudinally along the esophagus to expose the esophagus, and the esophagus around the tumor area was detached from the posterior mediastinum (Fig. 2b).

Esophagoscopic findings. Endoscopic injection of sodium hyaluronate solution (MucoUp®) with indigo carmine dye added in the submucosal layer just below the tumor.
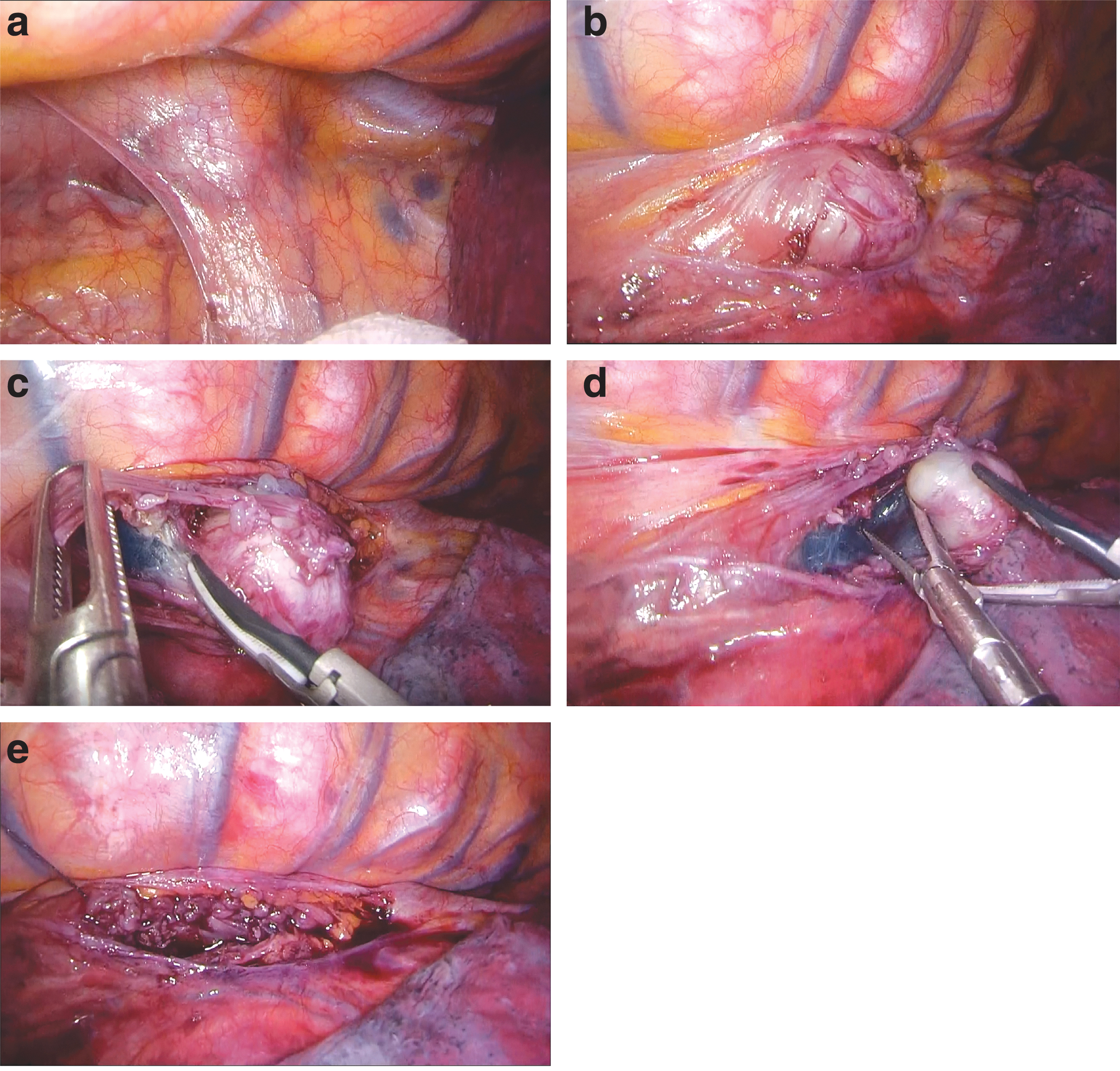
Thoracoscopic findings.
The muscularis propria layer and adventitia of the tumor area were then incised and dissected to expose the tumor and the previously injected indigo carmine dye. The gap between the mucosal layer and the tumor was clearly visible (Fig. 2c), and under the guidance of the injected dye, the tumor was enucleated without damaging the pseudocapsule (Fig. 2d).
After enucleation, the muscularis propria layer and adventitia were closed with continuous sutures using a 3-0 absorbed barbed suture (V-Loc®; Medtronic, Tokyo, Japan) (Fig. 2e). The tumor was removed from the body through a 12-mm port wound, but if the tumor was larger than the port wound, the wound incision was widened. Finally, the patient was observed endoscopically to ensure that there were no insufficiencies in the suturing and no stenosis. A 20-Fr chest tube was placed in the thoracic cavity through the eighth intercostal port, and the wound was closed.
Postoperative management
The day after surgery, the patient was gotten out of bed and started drinking water. On the third postoperative day, esophagography was performed to confirm that there was no leakage of contrast medium before oral intake was started. The chest tube was removed after oral intake began.
Results
Surgical outcomes
The surgical outcomes of the patients are shown in Table 2. The mean operative time was 122.6 minutes (range 84–168 minutes), mean blood loss was 21.1 mL (range 0–80 mL), and the mean postoperative hospital stay was 8 days (7–10 days). No intraoperative or postoperative complications were observed.
Surgical Outcomes of Patients with Esophageal Submucosal Tumors
GIST, gastrointestinal stromal tumor.
Pathological diagnosis
Pathology revealed 2 GISTs (1 low risk, 1 very low risk), 2 schwannomas, and 1 leiomyoma, similar to the preoperative diagnosis by FNAB.
Postoperative observation period
The mean postoperative observation period was 56.6 months (27–98 months). No recurrence of the SMT was observed during follow-up.
Discussion
Esophageal SMTs account for less than 1% of all esophageal neoplasms. 1 Among them, leiomyomas account for about 70%, GISTs 25%, leiomyosarcomas 5%, and the remainder are lipomas and schwannomas. 2 Considering all gastrointestinal SMTs, primary esophageal GISTs are extremely rare, occurring in less than 2% of all gastrointestinal SMTs. 3
EUS-FNAB is useful for the definitive diagnosis of esophageal SMTs, 6 and its rate of positive diagnosis is reported to be 89%. 7 Preoperative diagnosis of esophageal SMTs greatly influences the choice of surgical technique, and therefore it is recommended that histological diagnosis, including immunostaining by preoperative EUS-FNAB, should be performed whenever possible. All of our patients underwent preoperative EUS-FNAB to obtain a definitive diagnosis before surgery.
The indications of surgery for esophageal SMTs (from enucleation to subtotal esophagectomy) depend on the grade of malignancy and the presence of symptoms. 4 For benign esophageal tumors, tumor enucleation is acceptable for prognosis and preservation of function, and most SMTs such as leiomyomas and schwannomas are enucleated.8,9 The choice of surgical procedure, enucleation or esophagectomy, depends on the location, size, and suspected malignant behavior of the tumor. 10
For GISTs, tumor size and the mitotic rate of the tumor are associated with poor survival. 5 Moreover, the capsule of GISTs is not a true capsule, and tumor enucleation is not recommended because of the risk of dissemination. 11 Gastric and intestinal GISTs can be treated with segmental or wedge resections. 10 Hence, esophageal GISTs may require more invasive esophagectomy. However, there have been scattered reports of enucleation being selected for tumors of smaller diameters. 5
Which surgical procedure should be performed for esophageal GISTs remains controversial.4,5 Recent reports suggest that enucleation of primary esophageal GISTs may be recommended in patients with small tumors (2–5 cm) or in low-risk groups, 10 and these tumors showed low mitosis histopathologically and a low Ki-67 labeling index. 12 In contrast, esophagectomy may be recommended for larger GISTs above 5 cm in size and for very high-risk lesions with a high mitotic rate.5,13
Two of our patients had GISTs, but both tumors were in the low-risk group based on the preoperative pathological diagnosis and measured less than 5 cm (1.9 and 3.5 cm). So, we chose enucleation for these cases.
In recent years, advances in thoracoscopic surgery have led to many reports of thoracoscopic approaches to esophageal disease.10,14,15 The first thoracoscopic enucleation for esophageal leiomyoma was reported by Everitt et al., 14 and since then, the feasibility and safety of this approach in the treatment of leiomyomas and GISTs has been increasingly selected by several authors.15–17
The usefulness of thoracoscopic esophageal surgery with the patient in the prone position for esophageal cancer was also reported by Cuschieri. 18 Thoracoscopic surgery in the prone position is superior in terms of developing a better visual field due to the effect of gravity, less blood loss due to pneumothorax pressure, and thereby, fewer postoperative pulmonary complications.17,18
Claus et al. reported the successful thoracoscopic enucleation in the prone position for esophageal leiomyoma. 19 Moreover, Jeon et al. reported that esophagoscopy during thoracoscopic enucleation for benign esophageal SMT is useful in identifying tumor location and determining the appropriate direction of esophageal access incision. 20
During endoscopic submucosal dissection, local injection of sodium hyaluronate solution with indigo carmine dye into the submucosal layer can dissociate the dissected layer and clarify the boundaries, aiding in manipulation of the dissection. Therefore, we initiated this procedure by applying the technique of endoscopic submucosal dissection.
Daiko et al. reported a technique similar to ours and described a hybrid procedure combining esophagoscopy and thoracoscopy as a useful minimally invasive procedure. 17 We believe that this technique is a useful method allowing safe thoracoscopic enucleation as it avoids inadvertent damage to the tumor or mucosa and improves visibility by providing an indicator of the resection line when enucleating the tumor and by clarifying and coloring the gap due to swelling caused by the local injection of sodium hyaluronate solution plus indigo carmine dye.
Recently, the usefulness of endoscopic treatments for esophageal SMTs, such as per-oral endoscopic tumor resection 21 and submucosal tunnel endoscopic resection, 22 has been reported. However, these treatments may not be indicated depending on the tumor size and localization. Therefore, thoracoscopic surgery may be useful, particularly for large esophageal SMTs, and the choice of treatment should be based on the tumor size, tumor localization, and the skill of the surgeon.
Conclusions
We report the surgical technique of thoracoscopic enucleation with esophagoscopy in patients in the prone position for esophageal SMTs. Our technique of local injection of sodium hyaluronate solution with indigo carmine dye into the submucosal layer is a useful and safe method for esophageal SMTs because it provides an indicator of the resection line during enucleation.
Footnotes
Acknowledgments
Authors' Contributions
S.M. conceived the idea of the study, and wrote the manuscript. S.M., Y.H., S.O., M.H., Y.T., S.K., J.S., T.E., and O.S. are the surgeons who performed the operation and evaluated the patient. T.O. supervised the conduct of this study. All authors read and approved the final manuscript.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.