
Abstract
Background:
Life expectancy of patients with rectal cancer is increasing day by day with innovative treatments. Low anterior resection syndrome (LARS), which disrupts the comfort of life in these patients, has become a serious problem. We aimed to evaluate the effect of high ligation (HL) and low ligation (LL) techniques on LARS in rectal cancer surgery performed with the robotic method.
Materials and Methods:
The data of patients diagnosed with mid-distal rectal cancer between 2016 and 2021 who underwent robotic low anterior resection by the same team in the same center with neoadjuvant chemoradiotherapy were retrospectively evaluated. Patients were divided into two groups as those who underwent HL and LL procedures. Preoperative, 8 weeks after neoadjuvant treatment, 3 and 12 months after ileostomy closure were evaluated.
Results:
A total of 84 patients (41 HL, 43 LL) were included in the study. There was no statistically significant difference between the demographic characteristics and pathology data of the patients. Although there was a decrease in LARS scores after neoadjuvant treatment, there was a statistically significant difference between the two groups at 3 and 12 months after ileostomy closure (P: .001, P: .015).
Conclusions:
In patients who underwent robotic low anterior resection, there is a statistically significant difference in the LARS score in the first 1 year with the LL technique compared with that of the HL technique, and the LL technique has superiority in reducing the development of LARS between the two oncologically indistinguishable methods.
Introduction
Colorectal cancers are the third most common type of cancer worldwide. It accounts for ∼10% of all cancer cases and is the second leading cause of cancer-related deaths worldwide. 1 In the history of the treatment of this disease, the treatment approach is updated every day with surgical and medical innovations such as the preoperative application of oncological treatment and the definition of total mesorectal excision (TME).2–4 In addition, laparoscopic and robotic surgical procedures have gained a significant place in the treatment of rectal cancer with the adaptation of technological developments to rectal surgery.5,6
With the advances in medical, technological, and surgical techniques, the life expectancy in rectal cancer has increased 7 and the treatment of postoperative comorbidities has become a serious problem for patients and surgeons in the following period. 8 Low anterior resection syndrome (LARS), which occurs between 17.8% and 56% after TME, causes serious life discomfort in the early and late periods and prevents social life continuity. 9
With the postoperative superiority of laparoscopic or robotic TME over open TME in the surgical treatment of rectal cancer, these minimally invasive methods are increasingly used in rectal surgery. Especially with the advantages of robotic surgery in the narrow pelvis, nerve injuries that may cause LARS are less common. 10
The oncologic outcomes of HL or LL surgical techniques of the inferior mesenteric artery (IMA) in rectal cancer have been shown to be similar in studies, and this result has paved the way for the comparison of LARS, which is frequently seen after low anterior resection in rectal cancer, in these methods.11,12 There are reviews suggesting that with high ligation (HL) of the IMA, blood supply problems in colorectal anastomosis may be less and anastomotic complications may be less common. 13 In our study, we aimed to evaluate the superiority of robotic low ligation (LL) and HL techniques in patients with distal–intermediate rectal cancer who received neoadjuvant treatment for LARS, which causes serious disturbances in the comfort of life of patients after rectal surgery.
Materials and Methods
Our study was conducted with the decision of Antalya Training and Research Hospital Clinical Research Ethics Committee numbered 2023-019.
Patient selection and study design
This study was performed to investigate the effect of HL or LL of IMA on LARS in patients undergoing robotic TME. All patients who underwent robotic TME after neoadjuvant chemoradiotherapy for locally advanced (T3–T4 node negative/positive) mid or distally located rectal cancer at the Gastroenterology Surgery Clinic of Antalya Training and Research Hospital between 2016 and 2021 were included.
Neoadjuvant treatment was given as standard long course chemoradio therapy (CRT) (50.4 Gy radiotherapy and fluoropyrimidine-based induction chemotherapy to sensitize radiotherapy). At 8–10 weeks after CRT, patients underwent surgery after restaging.
TME surgery was performed by 2 surgeons experienced in colorectal surgery and certified in robotic surgery using the Da Vinci Xi system. During TME, the IMA was closed and cut either proximal to the left colic artery exit (HL) or distal to the left colic artery (LL). Which method was used was determined using the closed envelope technique and patients were divided into two groups as HL group and LL group. In all patients, the anastomosis was performed end to end using a 31 mm circular stapler.
At the end of adjuvant therapy, the ileostomy was closed using a 75 mm linear stapler (EthiconTM, NTLC 75) side by side with the peristomal incision. The data of patients who did not develop complications after ileostomy closure were prepared for analysis.
LARS scores were calculated for all patients preoperatively, 8 weeks after neoadjuvant, 3 months after ileostomy closure, and 1 year after ileostomy closure using the LARS scoring questionnaire defined by Emmertsen et al. in 201214 and the data were compared between the two groups.
Exclusion criteria
Only patients who underwent robotic TME were included in this study. Patients who underwent open or laparoscopic surgery were excluded. Upper rectal tumors were not included in this study. Patients who underwent ileostomy or colloanal anastomosis during surgery were also excluded. Patients who developed anastomotic leakage or other anastomosis-related complications (rectovaginal fistula, etc.) and patients in whom ileostomy could not be closed for any reason were also excluded.
Formation of the working group
During this period, 456 patients underwent TME for rectal tumors. In total, 305 patients were excluded because they underwent open or laparoscopic surgery. Of 151 patients, 32 were excluded because they had tumors located in the upper rectum. Of the remaining 119 patients, 14 were excluded due to colloanal anastomosis, 15 due to anastomosis-related complications, 3 due to failure to close the ileostomy, and 3 due to incomplete records, making a total of 84 patients (HL group/LL group, n = 41/43) (Fig. 1).
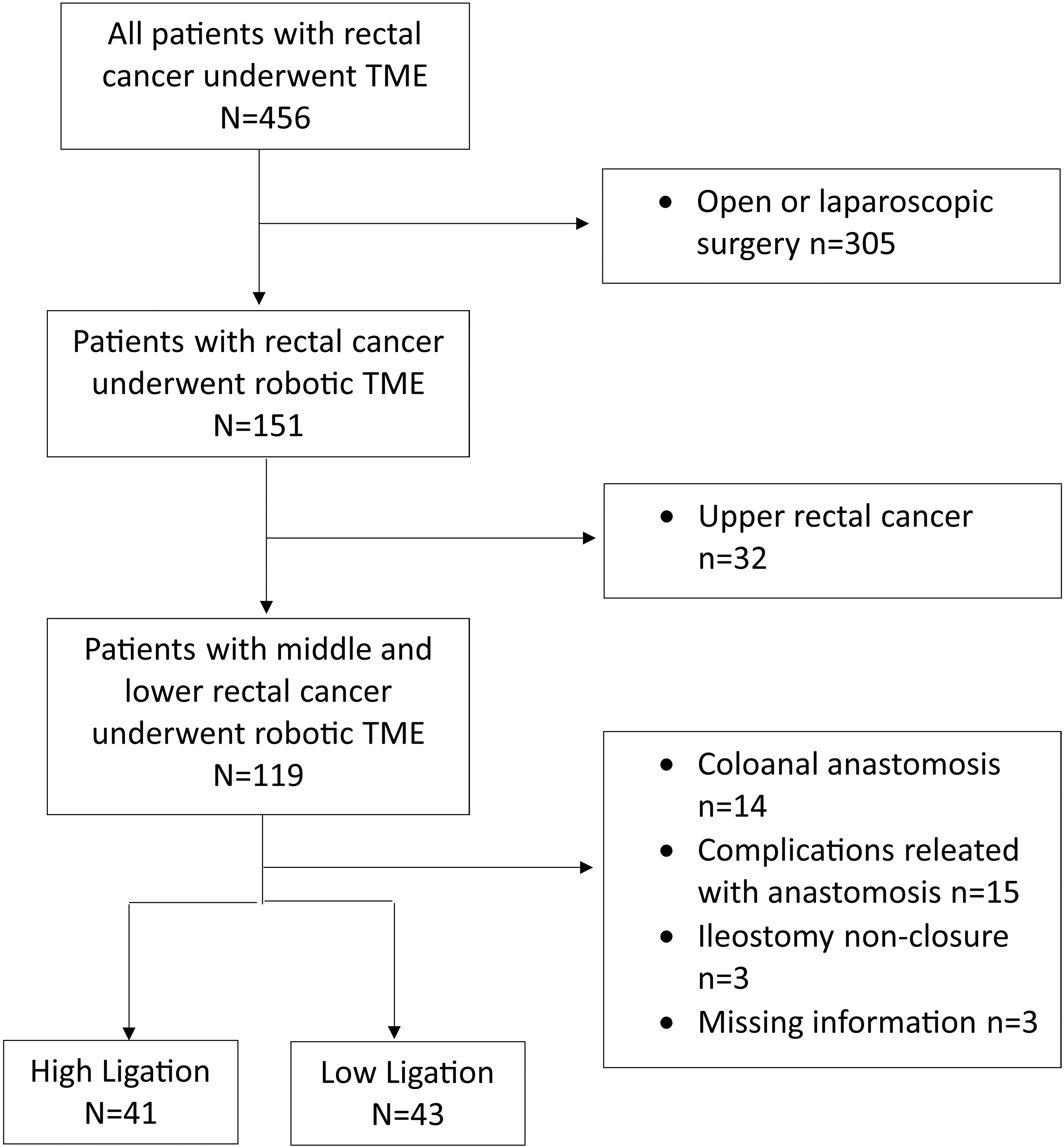
Election of the study groups.
Endpoint of the study
The primary endpoint of this study was to show that the LARS score at 3 months and 1 year after mid and distal rectal tumor surgery would be more favorable in the LL group than in the HL group.
Statistical analysis
Statistical analysis was performed using IBM's SPSS Statistics for Windows, Version (IBM Corp., Armonk, New York, NY, USA). Data are presented as n (%), mean ± standard deviation or median, depending on the condition. Normality assumptions were checked with the Shapiro–Wilk test. Pearson chi-square test was performed for categorical data. If >20% of the expected values were <5, they were analyzed with Fisher's exact test. Differences between two groups were evaluated with Student's t-test for normally distributed data or Mann–Whitney U test for non-normally distributed data. The difference between two different time measurements of a variable in the sample was evaluated using the paired t-test. A P < .05 was considered statistically significant.
Results
Data of a total of 84 patients with a median age of 61.7 years, 41 in the HL group and 43 in the LL group, were analyzed. In total, 63% of the patients were men and 37% were women and there was no difference in gender distribution between the two groups. In terms of comorbid diseases, 34 (40.5%) patients had comorbid hypertension, 5 (6%) patients had diabetes mellitus, 2 (2.4%) patients had previous coronary artery disease, and 5 (6%) patients had chronic obstructive pulmonary disease.
The median distance from the tumor site to the anal verge before neoadjuvant treatment was 7.6 cm and was similar in the two groups. According to TNM staging according to AJCC 8th edition, 4.8% of the patients had complete response, 34.5% had Stage 1, 21.4% had Stage 2A, 10.7% had Stage 3A, 20.2% had Stage 3B, and 8.3% had Stage 3C. Pathological stages were similar in both groups (Table 1).
Characteristics of Patients with Middle or Lower Rectal Cancer Who Underwent Robotic Total Mesorectal Excision
ASA, American Society of Anesthesiologists; AJCC, American Joint Committee on Cancer; CAD, Coronary artery disease; COPD, Chronic obstructive pulmonary disease.
The LARS scores of the patients in the HL group at diagnosis, after neoadjuvant CRT, 3 months after ileostomy closure, and 1 year later were 3.9, 1.9, 27.7, and 17.2, respectively. In the LL group, the same scores were 3.5, 2.1, 19.4, and 13.5, respectively. The scores at 8 weeks after preoperative and neoadjuvant CRT were similar in both groups, but the scores at 3 months and 1 year after ileostomy closure were higher in the HL group. According to LARS scores at 3 months after ileostomy closure, 34% of the patients in the HL group had no LARS, 26.8% had minor LARS, and 39% had major LARS.
In the LL group, 55.8% of the patients had no LARS, 32.6% had minor LARS, and 11.6% had major LARS. In the postoperative 1st year evaluation, 65.9% of the patients in the HL group had no LARS, 29.3% had minor LARS, and 4.9% had major LARS. In the LL group, minor LARS was observed in 7% patients and major LARS was observed in 4.7% patients in the same period. (Table 2).
Comparision of Low Anterior Resection Syndrome Scores in High ligation and Low Ligation Groups
CRT, chemoradio therapy; LARS, low anterior resection syndrome.
In both groups, LARS scores, which were higher at the time of diagnosis, significantly decreased after nCRT but significantly increased again at 3 months after ileostomy closure. At 1 year after ileostomy closure, there was a significant decline in scores in both groups (Table 2).
Discussion
LARS is observed in 22% of patients undergoing TME in rectal cancer treatment. 15 Considering the advantages of laparoscopic surgery in rectal surgery,16–19 open and laparoscopic results for LARS scores are similar in the literature. There are studies in favor of LARS in robotic surgery. Again, there are studies advocating LL in studies indicating advantages in terms of LARS development between HL and LL techniques of IMA, but there are no studies in the literature comparing robotic surgery with HL and LL. In our study, we compared the occurrence of LARS after robotic TMJ after HL and LL techniques and found that it was in favor of LL.
Preoperative CRT treatment, comorbidities of the patients, proximity of the tumor to the anal canal, and postoperative complications are generally blamed as the factors of LARS syndrome. However, there is no study in the literature that detected a change in LARS values with the shrinkage of the mass with neoadjuvant CRT in the preoperative period. In our study, although there was a proportional decrease in LARS after neoadjuvant CRT, it was not statistically significant (P: .735). Perhaps the effects of neoadjuvant therapies on LARS will become clearer in the coming years with the increase in the number of patients with complete response in rectal cancer who are enrolled in the follow-up program.
When the pathophysiology of LARS is evaluated, the physiology of defecation completely changes with the disappearance of the rectum or volume change with the neorectum created and the neural conductivity is affected by the resection.20–22 Irritability increases in the neorectum created by anastomotic complications or nerve damage and the incidence of LARS increases accordingly. 23
Since the most important complication in TME is anastomotic leakage, surgeons have defined different techniques to minimize this complication. It is thought that with the application of LL instead of HL of IMA, the risk of impairment in the blood supply of the anastomosis will be further reduced and anastomotic complications will be less common. Studies evaluating postoperative complications between the two methods with similar oncological results and emphasizing the advantages of LL are available in the literature. 12 In the current limited study, no significant difference was found between HL and LL in laparoscopic TME. 24
With the development of oncological treatments and surgical procedures, life expectancy in rectal cancer is increasing day by day. 25 With the advantages of minimally invasive surgery in the treatment of rectal cancer, there are significant advantages in recovery and return to normal life.26–28 With the advantages of robotic surgery in rectal surgery, its place in treatment is increasing day by day.10,29–30 The three-dimensional vision and the mobility of the arms in robotic surgery provide both the patient with the postoperative advantage of minimally invasive singles and the surgeon with the advantage of serious dissection during surgery.31,32
Injury as a result of hypogastric nerve dissection, which is one of the causes of LARS, can be minimized with the visual angle provided by robotic surgery.33–36 Although laparoscopic HL and LL are compared in the literature, the applicability of LL in robotic surgery has been determined in studies, although there are limited number of studies on this subject. 37 In our study, this issue was evaluated and LARS was evaluated in groups of robotic HL and LL patients. It was found that the LL group was statistically significantly more advantageous in terms of the occurrence of LARS in the 3rd and 12th months after ileostomy closure (HL and LL LARS ratio at third month—HL and LL LARS ratio at 12th month).
Limitations of the study
Although there are no studies in the literature under the title of LARS evaluation in robotic HL and LL procedures, the studies are compared with laparoscopic surgery, which is the closest procedure to robotic surgery. Another important limitation is the lack of long-term LARS results data in our study.
Conclusion
Innovations in the surgical treatment of rectal cancer are prolonging the life expectancy of patients with each passing day. With this situation, the long-term problems of patients who have undergone surgery are becoming more on the agenda of patients and surgeons. The frequency of application of minimally invasive surgical methods in rectal surgery is increasing due to its postoperative advantages.
We found that LARS, which seriously disrupts the social life and comfort of patients after rectal surgery, is the procedure in which both anastomotic complications and nerve damage are minimized and the incidence of LARS is the lowest with the combination of the robotic procedure offered by technology and the LL procedure in which anastomotic nutrition is maximized. However, studies with a larger number of patients evaluating long-term results are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.