
Abstract
Background:
Esophageal diverticula were traditionally treated with open surgery, which is associated with significant morbidity and mortality rates. Management has shifted to minimally invasive approaches with several advantages. We examine outcomes in patients with esophageal diverticula treated with minimally invasive techniques by a multidisciplinary surgical team at a single center.
Materials and Methods:
A retrospective review of a prospectively maintained database was performed for patients who underwent minimally invasive surgery for esophageal diverticula at our institution from June 2010 to December 2022. Primary outcomes were 30-day morbidity and mortality rates. Secondary outcomes were symptom resolution, length of stay (LOS), readmission, and need for reintervention.
Results:
A total of 28 patients were identified. Twelve patients had pharyngeal diverticula, 7 patients had midesophageal diverticula, and 9 patients had epiphrenic diverticula. Thirty-day morbidity and readmission rates were 10.7% (3 patients), 1 pharyngeal (sepsis), 1 midesophageal (refractory nausea), and 1 epiphrenic (poor oral intake). There were no esophageal leaks. Average LOS was 2.3 days, with the pharyngeal group experiencing a significantly shorter LOS (1.3 days versus 3.4 days for midesophageal, P < .01 versus 2.8 days for epiphrenic, P < .05). Symptom resolution after initial operation was 78.6%. Reintervention rate was 17.9%, and symptom resolution after reintervention was 100%. There were no mortalities.
Conclusion:
This study demonstrates that esophageal diverticula can be repaired safely and efficiently when performed by a multidisciplinary team utilizing advanced minimally invasive endoscopic and robotic surgical techniques. We advocate for the management of this rare condition at a high-volume center with extensive experience in foregut surgery.
Introduction
Esophageal diverticula are rare disorders caused by an outpouching of the esophageal mucosa that primarily affects the elderly, with a prevalence ranging from 0.06% to 4%. 1 An esophageal diverticulum can be categorized based on location as pharyngeal (Zenker), midesophageal (Rokitansky), or epiphrenic, each with a unique pathophysiology. Although most patients remain asymptomatic, esophageal diverticula can cause a range of symptoms as they progress, including chest pain, dysphagia, and regurgitation. If left untreated, patients can develop serious complications, such as aspiration pneumonia, severe malnutrition, medication malabsorption, and lung abscesses.2,3
Pharyngeal diverticula are the most common with a prevalence ranging from 0.01% to 0.11%. 2 Midesophageal diverticula account for ∼15% of esophageal diverticula and are usually located near the tracheal bifurcation, whereas epiphrenic diverticula are most commonly located at the distal 10 cm of the esophagus. 4 Midesophageal diverticula can occasionally precipitate gastrointestinal hemorrhage, hemoptysis, or fistula formation between the diverticulum and the trachea or major vascular structures. 5 Epiphrenic diverticula are often associated with motility disorders, with prevalence reports ranging from 35% to 100%, though a causative relationship between the two processes is unclear. 6
Treatment for esophageal diverticula should be considered for symptomatic cases. Traditionally, treatment for pharyngeal diverticula was an open cricopharyngeal myotomy, and treatment for midesophageal and epiphrenic diverticula was diverticulectomy with esophageal myotomy through thoracotomy.5,7–9 However, due to the significant postoperative morbidity associated with open surgery, minimally invasive techniques have emerged and demonstrated several advantages, including faster recovery and decreased postoperative complications.2,8,10,11
These techniques are accomplished by several specialties, including minimally invasive general surgery, thoracic surgery, otolaryngology, and gastroenterology. Data on the safety and efficacy of minimally invasive surgery for esophageal diverticula are lacking due to the rarity of this condition. In this study, we examine the outcomes in patients with esophageal diverticula managed with minimally invasive endoscopic and robotic approaches by a multidisciplinary surgical team at a single academic center.
Materials and Methods
A retrospective review of a prospectively maintained institutional review board-approved database was performed for all patients undergoing minimally invasive surgery for esophageal diverticula at a single academic institution between June 2010 and December 2022. Patient demographics included age at time of surgery, gender, American Society of Anesthesiologists classification, presenting symptoms, preoperative manometry, diverticulum size, and diverticulum location. Intraoperative data included total operative time, operative approach, and fundoplication type. Postoperative outcomes data included 30-day morbidity, 30-day mortality, hospital length of stay (LOS), readmission, need for reintervention, and symptom resolution.
Patients underwent a comprehensive preoperative workup, including barium esophagram and upper endoscopy. Patients with midesophageal and epiphrenic diverticula additionally underwent high resolution manometry and pH testing if reflux symptoms were present. Our primary outcome measures were 30-day morbidity and 30-day mortality rates. Secondary outcomes were symptom resolution, LOS, readmission, and need for reintervention. All statistical analyses were performed in R (version 4.1.2, Vienna, Austria). One-way analysis of variance was used for continuous variables and Fisher's exact test was used for categorical variables with P < .05 considered to be statistically significant.
Surgical technique
Pharyngeal diverticula
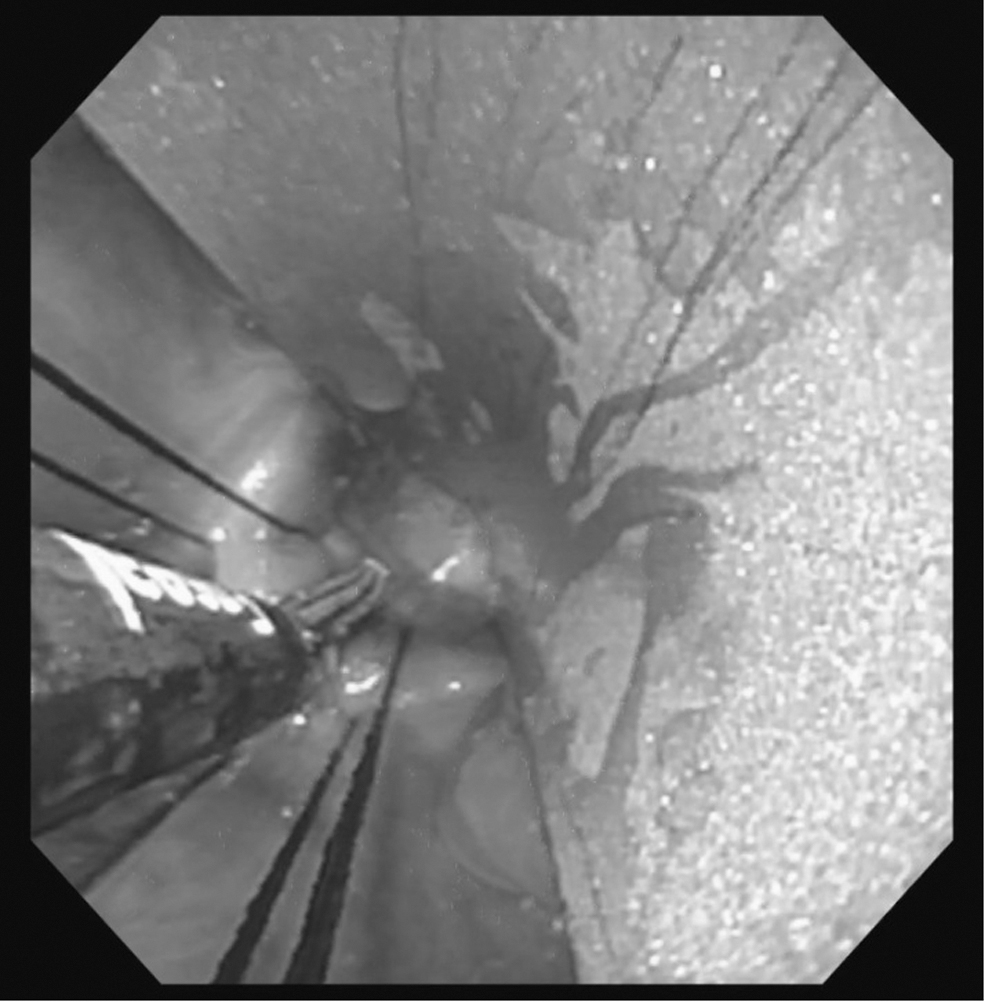
An endoscopic approach was used for management of all pharyngeal diverticula. All patients undergo general anesthesia and orotracheal intubation. A diverticuloscope is introduced into the hypopharynx down to the diverticulum pouch to confirm the correct level, and the common wall between the esophagus and the diverticulum is identified (Fig. 1). The diverticulum is then decompressed of any retained debris or fluid. If needed, one or two traction sutures are placed. A flexible pediatric endoscope is then introduced to visualize the esophagus.

Endoscopic view of the esophageal lumen (superiorly) and pharyngeal diverticulum (inferiorly) separated by a common wall.
Under direct visualization, a bipolar tissue sealer device is used to divide the diverticulum septum, creating a cricopharyngeal myotomy and diverticulotomy (Fig. 2). Depending on the diverticulum size, multiple device activations are performed to ensure complete division of the common wall. Upon completion of the myotomy (Fig. 3), the traction sutures and endoscope are carefully removed.
Endoscopic view of diverticulotomy using a bipolar tissue sealer device. Note the two traction sutures.

Endoscopic view postdiverticulotomy with complete division of the cricopharyngeal muscle and common wall.
Midesophageal diverticula
A right robotic-assisted thoracoscopic approach was utilized for management of midesophageal diverticula. Patients are placed in the left lateral decubitus position. A 1 cm incision is then made in the eighth intercostal space along the posterior axillary line. Blunt dissection is then performed through this incision using the camera and optical trocar into the chest cavity. Three additional robotic trocars, two 8 mm and one 12 mm, are then placed (Fig. 4). The Da Vinci Xi robotic surgical system (Intuitive Surgical, Sunnyvale, CA, USA) is then docked. The parietal pleura is first entered, and the lung is carefully dissected away from the esophagus.
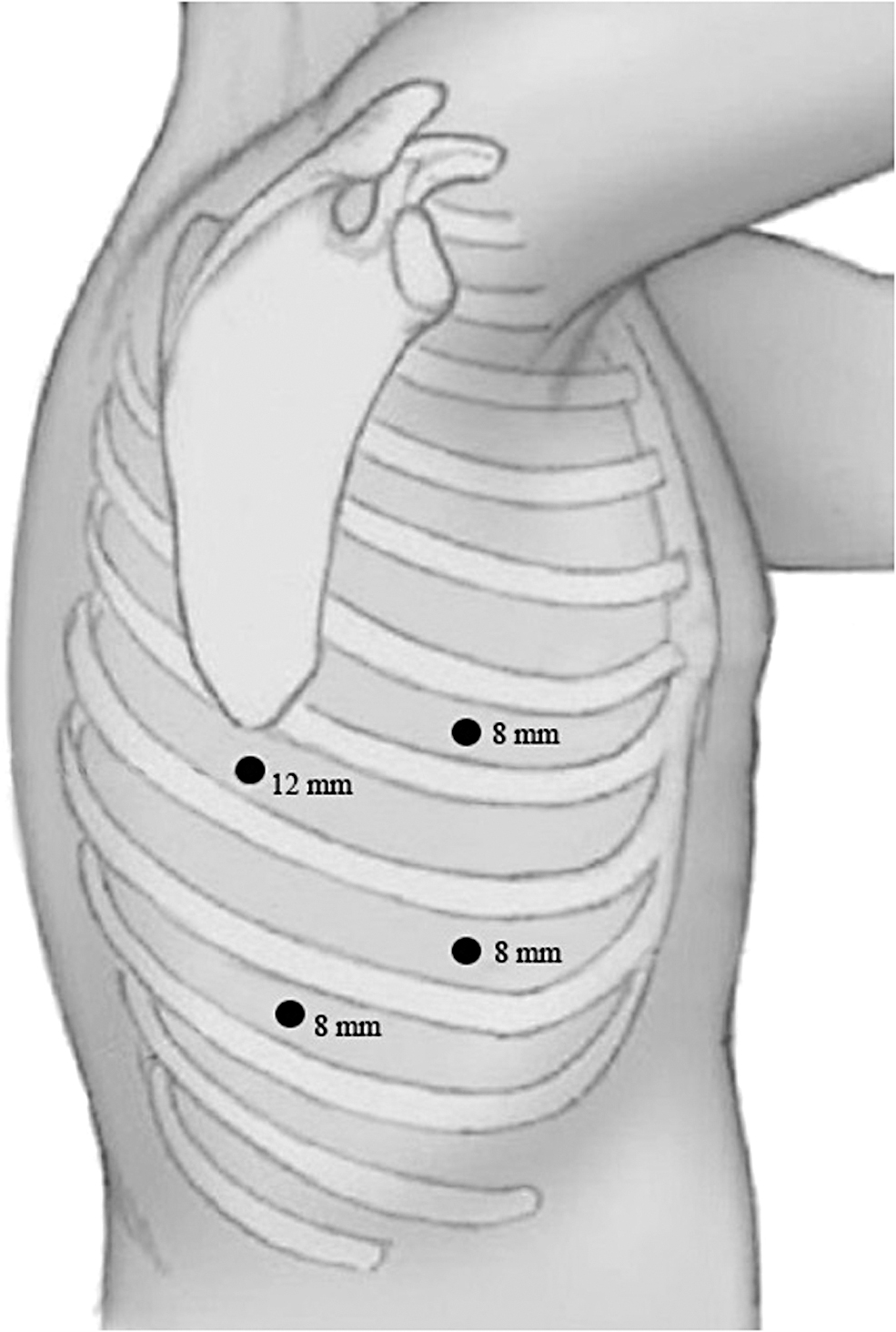
Port placement for right robotic-assisted thoracoscopic midesophageal diverticulum repair with patient in the left lateral decubitus position.
The inferior pulmonary ligament is then taken down and the dissection is carried along the esophagus. During this dissection, care is taken to identify and avoid injury to the vagus and phenic nerves. The diverticulum is then identified, and an upper endoscopy is performed concurrently to better visualize and isolate the diverticulum. The diverticulum sac and neck are dissected free from surrounding structures, and the neck is divided using a 60 mm endoGIA stapler. A 5 cm myotomy is performed using hook electrocautery, extending from the upper portion of the diverticulum resection site distally. A conclusion upper endoscopy is then performed to evaluate the resection site and a right chest tube is placed through the original camera incision.
Epiphrenic diverticula
In all cases of epiphrenic diverticula, a robotic-assisted transhiatal approach is first attempted. The patient is placed on the operating table in a supine position with arms out and legs split. Before prepping, the patient is placed in steep reverse Trendelenburg position to ensure the patient is appropriately secured to the operating room table. Port sites are placed as depicted in Figure 5.
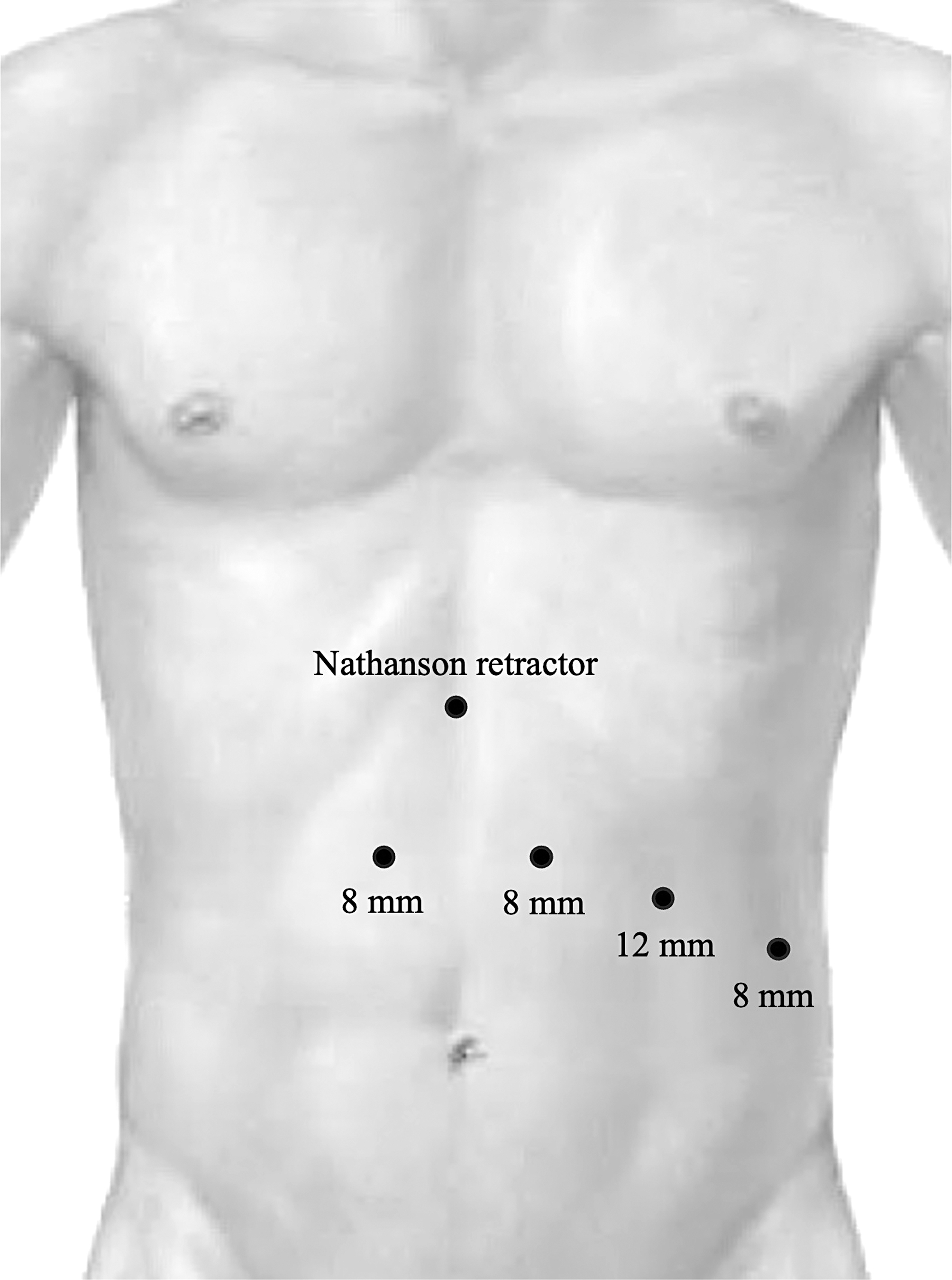
Port placement for robotic-assisted laparoscopic transhiatal epiphrenic diverticulum repair.
First, the peritoneum overlying the left crus of the diaphragm is divided, followed by division of the short gastric vessels. The peritoneum overlying the right crus is then divided, exposing the esophagus. Anterior and lateral dissection are then performed in the lower third of the esophagus up to the level of the diverticulum. If we are unable to satisfactorily reach the diverticulum from a transhiatal approach, a transthoracic approach is performed as previously described.
After this dissection, the robotic system is then docked. Hook electrocautery is placed in the right arm and a fenestrated bipolar grasper in the left. After placement of a 52-French Bougie, the fat pad of the stomach is mobilized with hook electrocautery. The anterior vagus nerve is identified and dissected upward ∼10 cm, separating it from the esophageal wall and moving it to the right side.
The esophagogastric junction is then exposed, and hook electrocautery used to mark out the myotomy site. The diverticulum sac and neck are dissected free, and the neck is divided using a 60 mm endoGIA stapler (Fig. 6). The myotomy is extended proximally until the neck of the diverticulum is passed, and then extended distally onto the stomach for 2 cm. A partial fundoplication is then performed. A conclusion upper endoscopy is performed to evaluate the resection site and fundoplication.

Robotic-assisted laparoscopic view of transhiatal epiphrenic diverticulectomy using a laparoscopic stapler.
Results
Patient demographics
A total of 28 patients were identified. Average patient age was 66.5 years and 39.3% were women. Twelve patients had pharyngeal diverticula, 7 midesophageal, and 9 epiphrenic. The pharyngeal group had a significantly smaller average diverticulum size at 2.4 cm compared with midesophageal (4.0 cm, P < .05) and epiphrenic (5.0 cm, P < .05). Most patients presented with dysphagia (85.7%), with the second most common symptom being regurgitation/reflux (50%). Preoperative manometry was obtained in 16 patients: 10 were found to have achalasia, 3 jackhammer, and 3 normal peristalsis. Patient demographic information is detailed in Table 1.
Patient Demographics
Diverticulum size obtained in 11 pharyngeal, 6 midesophageal, and 7 epiphrenic patients.
Diverticulum location only obtained in 5 midesophageal patients and 4 epiphrenic patients.
ASA, American Society of Anesthesiologists; E, epiphrenic; M, midesophageal; P, pharyngeal; SD, standard deviation.
Intraoperative data
Overall average operative time was 121.1 (±66.6) minutes. The pharyngeal diverticula group had a significantly shorter average operative time (62.7 minutes) than midesophageal (145.8 minutes, P < .05) and epiphrenic (176.0 minutes, P = .001) groups. All pharyngeal diverticula were managed endoscopically, whereas a robotic-assisted approach was used for all midesophageal and epiphrenic diverticula. A total of 12 fundoplications were performed. Intraoperative data are detailed in Table 2.
Intraoperative Data
E, epiphrenic; M, midesophageal; P, pharyngeal; SD, standard deviation.
Postoperative outcomes
There were no esophageal leaks. Thirty-day morbidity and readmission rates were 10.7% (3 patients), 1 in the pharyngeal group (sepsis), 1 in the midesophageal group (refractory nausea), and 1 in the epiphrenic group (poor oral intake). Average LOS was 2.3 days, with the pharyngeal group experiencing a significantly shorter LOS (1.3 days versus 3.4 days for midesophageal, P < .01 versus 2.8 days for epiphrenic, P < .05).
Symptom resolution after initial operation was 78.6% (66.7% for pharyngeal, 71.4% for midesophageal, and 100% for epiphrenic, P = .15). Reintervention rate was 17.9%, 3 in the pharyngeal group (all redo endoscopic diverticulotomies), and 2 in the midesophageal group (endoscopic botox administration, endoscopic dilation, and endoscopic myotomy). Symptom resolution after reintervention was 100%. There were no mortalities. Postoperative outcomes are detailed in Table 3.
Postoperative Outcomes
E, epiphrenic; M, midesophageal; P, pharyngeal; SD, standard deviation.
Discussion
Esophageal diverticulum surgery is generally challenging and has traditionally been associated with high morbidity and mortality rates. Open surgery is particularly morbid, and its complications can be devastating. Although the surgical treatment for esophageal diverticula has evolved from open to minimally invasive approaches, there is a paucity of long-term large-scale data and the best surgical approach remains uncertain. Minimally invasive techniques have gained popularity due to their reported lower morbidity and mortality rates in several case series. In our experience with a cohort of 28 patients, we have found minimally invasive approaches to provide good symptom resolution with a favorable safety profile.
Open pharyngeal diverticula repair was previously the standard of care, but carries a morbidity rate of up to 11% and mortality rate of 0.6%. 12 Serious complications can occur with open repair, such as cervical infection (e.g., mediastinitis), leak, perforation, and nerve damage. Rigid and flexible endoscopic management of pharyngeal diverticula has gained popularity in recent years, with the added benefit of transoral removal options and the possibility to forego general anesthesia and limit neck extension. 13 Endoscopy is an especially desirable approach for elderly patients or those patients with medical comorbidities that may preclude more invasive surgical options.
Endoscopy has been shown to have several other advantages when compared with open pharyngeal diverticula repair, including shorter operative time, decreased hospital LOS, quicker resumption of oral intake, and lower complication rates at 7%–8% on average.2,10 For rigid endoscopy, the electrocautery technique was previously used for diverticulectomy, but this has largely been replaced by other options, including the endostapler, carbon dioxide laser, and other advanced energy devices that use bipolar, monopolar, or ultrasonic energy. 14
Flexible options include diverticulectomy using a stag beetle or clutch cutter knife.15,16 Peroral endoscopic myotomy for the treatment of Zenker's diverticulum (Z-POEM) is a novel technique that has been described in several reports.17–19 This technique creates a third space through submucosal endoscopic tunneling that enables complete exposure and division of the septum, with technical and clinical success in >90% of cases in multiple reports.19,20 Although there is no consensus on the optimal endoscopic technique for minimally invasive treatment of pharyngeal diverticula, the array of available options represents a promising long-term alternative to standard open surgery.
Endoscopic pharyngeal diverticula repair has seen variable recurrence rates between 0% and 35%. 21 Among our 12 endoscopically treated pharyngeal diverticulum patients, 4 (33.3%) experienced recurrence: 3 of these patients had successful endoscopic revisions and 1 was lost to follow-up. Although symptom recurrence rates are often reported to be higher for endoscopic surgery, endoscopic revision is efficient and easily performed with low morbidity and high success rates.21,22 It is also a viable option for patients who received prior open repair. 23 We report a relatively low morbidity rate for these patients than those undergoing open surgery at 8.3% with no mortalities.
Among the three types of esophageal diverticula, midesophageal diverticula is the least common with very little published on treatment experience and outcomes. Thoracotomy was previously the standard of care with a high associated mortality rate of up to 9% and leak rates of up to 18%.24,25 A limited number of studies have been published on minimally invasive repair. One small case series of 3 patients who underwent thoracoscopic repair reported zero leaks, but there was 1 mortality. 26 One case report described successful endoscopic treatment using a needle-knife through a flexible endoscope. 27
Another case series describes treatment in 2 patients using POEM. 28 Similar to the management of midesophageal diverticula, the previous standard of care for epiphrenic diverticula was open repair through a thoracotomy. Open epiphrenic diverticulum repair carries high morbidity, with an esophageal leak rate as high as 21%, and a mortality rate as high as 11%.1,29,30 There has been increasing evidence for the feasibility of laparoscopic repair, which has become the preferred approach for many institutions.4,31,32 Although studies have shown that laparoscopic repair reduces mortality, decreases LOS, and is similarly efficacious, morbidity remains high in some studies. A recent review of laparoscopic epiphrenic diverticular repair reports leak rates ranging from 8% to 23% and mortality rate between 0% and 7%.33,34
We were able to successfully perform robotic-assisted repair in all 7 midesophageal and 9 epiphrenic diverticula patients. Given that these types of esophageal diverticula are highly associated with esophageal dysmotility, diverticulectomy alone is not sufficient and we routinely perform concurrent myotomies to ensure optimal symptom resolution. In our patient cohort, we were able to achieve a relatively low morbidity rate with no esophageal leaks and no mortalities. Two out of 7 midesophageal patients had symptom recurrence and required reintervention, but were successfully treated endoscopically. All epiphrenic patients had symptom resolution after initial surgery.
The utilization of robotic techniques for esophageal diverticula repair has been gaining popularity as well. Robotic surgery provides increased degrees of freedom with articulation and improvements in tissue manipulation and visibility, which is especially advantageous for technically demanding midesophageal and epiphrenic esophageal diverticula repairs. The improved resolution through a three-dimensional view also allows for visualization and precise division of each individual muscular fiber during the myotomy, ensuring that it is adequate, but not too extensive. 33
There are few other published cases in the literature describing robotic-assisted esophageal diverticulum repair. One case series describes the successful treatment of 3 epiphrenic esophageal diverticula using a robotic-assisted transthoracic approach. 34 Two other case reports describe a robotic-assisted transhiatal approach for repair of large epiphrenic diverticula.35,36 Here we report a larger cohort of 16 successful robotic esophageal diverticula repairs with low morbidity and no esophageal leaks. We recommend a robotic-assisted approach for midesophageal and epiphrenic esophageal diverticula repair when feasible given its safety, efficacy, and associated technical advantages.
Our results are encouraging and demonstrate the favorable outcomes of minimally invasive esophageal diverticula repair compared with open surgery. Endoscopic and robotic techniques have become the preferred modalities at our institution. The implementation and mastery of minimally invasive esophageal diverticula repair are necessary for the contemporary management of this rare condition.
Given the need for endoscopic and robotic-assisted thoracoscopic and laparoscopic expertise, we have employed a multidisciplinary team approach to the management of esophageal diverticula with frequent involvement of multiple specialties during surgery to achieve optimal outcomes. Ongoing collaboration between disciplines will be necessary for esophageal diverticula management as treatment techniques become more advanced with time.
Although our results and the other cases presented here are promising, larger and long-term prospective studies are needed to evaluate the specific morbidity risks, efficacy, and outcomes associated with these minimally invasive approaches. Limitations of this study include its retrospective nature, as well as our small heterogeneous study population given that esophageal diverticula are relatively rare.
Conclusion
This study demonstrates that esophageal diverticula can be repaired safely and efficiently when performed by a multidisciplinary team utilizing advanced minimally invasive endoscopic and robotic surgical techniques. We advocate for the management of this rare condition at a high-volume center with extensive experience in foregut surgery.
Footnotes
Authors' Contributions
R.C.B. contributed to conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—review and editing, and project administration; G.J.S. was involved in formal analysis, data curation, software, and writing—review and editing; E.Y.H. carried out formal analysis, data curation, software, and writing—review and editing; B.J.S. and G.R.J. were in charge of conceptualization and supervision; R.A.W., M.W.O., and P.A.W. took charge of conceptualization, investigation, and supervision; and S.H. was in charge of conceptualization, investigation, supervision, writing—original draft, and writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.