
Abstract
Objective:
The aim of this study is to compare the precision and applicability of the Zhongshan (ZS) score against the radius, exophytic/endophytic, nearness, anterior/posterior, and location (RENAL) score in forecasting perioperative outcomes during laparoscopic partial nephrectomy (LPN).
Materials and Methods:
We retrospectively analyzed data from 99 renal cancer patients who underwent LPN between January 2017 and August 2023. Patients were scored and categorized based on both the ZS and RENAL scores. The study then compared perioperative outcomes across these groups and further investigated the correlation between ZS and RENAL scores and overall complication rates.
Results:
LPN was successfully accomplished in 94 patients, whereas 5 patients necessitated conversion to open or radical surgery. The high-risk group, according to the ZS score, manifested more warm ischemic time (WIT) than the low-risk group (P = .007). Furthermore, the incidence of overall complications escalated with increase in the ZS score grade (P = .045). A higher RENAL score corresponded to a greater risk of conversion to open or radical treatment (P = .012). Correlation analyses revealed associations between both ZS and RENAL scores and overall complications. The RENAL score also correlated with changes in blood creatinine values, while the ZS score was associated with WIT (all P < .05). In the univariate analysis, both ZS and RENAL scores were substantial factors for the occurrence of total complications (P = .029 and P = .027, respectively), but they were not statistically significant in the multivariate analysis. The receiver operating characteristic curves suggested that both individual and combined ZS and RENAL scores held predictive potential for the onset of overall complications (area under the curve = 0.652, 0.660, and 0.676, respectively).
Conclusions:
Compared with the RENAL score, the ZS score provides a more comprehensive assessment of tumor complexity in patients undergoing LPN. Integrating these two scores could potentially improve the accuracy of predicting surgical risks.
Introduction
The continuous advancements in imaging technology coupled with the widespread adoption of physical examinations have led to a year-on-year increase in the detection rate of renal tumors. Approximately 85% of these tumors are identified as renal cell carcinoma (RCC). 1 Current research suggests that laparoscopic partial nephrectomy (LPN) for early-stage RCC (T1a) offers efficacy equivalent to that of radical nephrectomy (RN). Additionally, LPN reduces the long-term risk of chronic kidney disease and cardiovascular disease. 2 Given its minimal invasiveness and faster recovery time, LPN is endorsed as a clinical option by the European Society of Urology and the Urological Association, serving as the standard treatment procedure for clinically limited RCC. 3
To better quantify the risks and challenges associated with partial nephrectomy (PN), various renal tumor scoring systems have been developed and studied extensively. Notably, the radius, exophytic/endophytic, nearness, anterior/posterior, and location (RENAL), preoperative aspects and dimensions used for an anatomical (PADUA), and C-index scores are the most commonly used and investigated.4–6 However, each possesses certain limitations, including the inability to describe the relationship between a renal tumor and renal vascularity and the observation that the precision of the PADUA score does not significantly alter upon removal of certain elements. 7
Therefore, Zhou et al. proposed the Zhongshan (ZS) scoring system, an integration of key features from the RENAL and PADUA scores. This system, based on just three measurement parameters, captures crucial anatomical aspects of renal tumors. Studies have demonstrated its superior predictive ability for PN surgery complexity compared with the RENAL and PADUA scores. 8 Despite this, studies focusing on the ZS score's application in LPN are sparse, with no comparative studies reported between the ZS and RENAL scores in the context of LPN.
In our study, we evaluated the predictive efficacy of the ZS score in LPN, through a retrospective analysis of renal tumor patients who underwent the procedure, and compared the clinical utility of the ZS and RENAL scores.
Materials and Methods
Patient selection
This study conducted a retrospective analysis of data from 99 patients who underwent LPN between January 2017 and August 2023 at our institution. Preoperative abdominal computed tomography or magnetic resonance imaging was performed on all patients. We excluded patients with a history of renal surgery, other simultaneous renal surgeries, bilateral or multiple lesions, or impaired renal function.
The study collected data on the following variables as indicators for ZS and RENAL scores: gender, age, age-adjusted Charlson comorbidity index (aCCI), maximum tumor diameter, warm ischemic time (WIT), operative time (OT), preoperative and postoperative creatinine levels, and complications.
Overall complications were categorized as intraoperative (including conversion to open or radical treatment and blood transfusions) and/or postoperative complications, which were further classified and recorded according to the Clavien–Dindo grading system. 9
Nephrometry scores
A senior resident, not directly involved in the procedure and unaware of the outcomes, received comprehensive training from experienced radiologists. This resident then independently evaluated each renal tumor using the ZS and RENAL scores, as detailed by Zhou et al. 8 and Kutikov and Uzzo. 4 An associate surgeon reviewed these evaluations, with disagreements resolved through joint discussions.
The ZS score considers three parameters: Ri (maximum tumor diameter), L (tumor location), and D (depth of tumor invasion). Ri represented the maximum diameter of contact between the tumor and renal parenchyma, with the diameter value rounded to contribute directly to the total score. The L parameters were assigned scores of 1–3, contingent upon the location of the tumor in relation to the central region of the renal hilum. Similarly, the D parameters were scored from 1 to 3 based on the depth of tumor invasion.
The total ZS score categorizes tumors into low- (3–4), intermediate- (5–7), or high- (≥8) risk groups. The RENAL score incorporates the tumor diameter, exophytic rate, proximity to the collecting system, pole–line relationship, and anteroposterior position. Scores of 4–6, 7–9, and ≥10 correspond to low, intermediate, and high risk, respectively. Finally, the study analyzed the correlation of ZS and RENAL scores with various perioperative indices of LPN.
Statistical analyses
Statistical analyses were conducted using the SPSS 26.0 statistical software. Quantitative data are presented as median (interquartile range), denoted as M (Q), and compared between groups using either the one-way analysis of variance or Kruskal–Wallis rank sum test. Categorical variables are described as frequency and percentage and compared between groups using either Pearson's chi-square test or Fisher's exact test.
The Spearman correlation analysis was used to determine the relationship between RENAL and ZS scores and perioperative indices. Univariate and multivariate logistic regression analyses were performed to identify factors affecting the occurrence of total complications.
Furthermore, receiver operating characteristic (ROC) curves were plotted using GraphPad Prism software, and the area under the curve (AUC) was compared to evaluate the predictive ability of ZS and RENAL scores, and their combination, for overall complications. P = .05 was used as the significance level.
This study was approved by the Ethics Committee of the Guizhou Provincial People's Hospital, ensuring adherence to the Declaration of Helsinki guidelines. Informed consent was obtained from all participants.
Results
Table 1 presents the demographic and tumor characteristics of the 99 patients. Among these patients, 59 had an aCCI score of 0–1; 34 had a score of 2–3; and 6 had a score of 4 or higher. The median preoperative serum creatinine level was 74 μmol/L (interquartile range [IQR] 65–84). The median maximum tumor size measured 3.1 cm (IQR 2.4–4.0). Median RENAL and ZS scores were both 7 (IQR 6–8). The tumor TNM stage distribution was cT1a in 76 patients, cT1b in 22 patients, and cT2a in only 1 patient.
Baseline Characteristics of the 99 Patients Included in the Analysis
aCCI, age-adjusted Charlson comorbidity index; RENAL, radius, exophytic/endophytic, nearness, anterior/posterior, and location; Scr, serum creatinine; ZS, Zhongshan.
Table 2 shows the surgical outcomes among distinct risk groups based on the ZS score. A notable difference in WIT was statistically significant in the intergroup comparison. Further pairwise comparisons revealed prolonged WIT in the high-risk group compared with the low-risk group (25.0 minutes versus 15.0 minutes, P = .006). However, the difference between the intermediate-risk and low-risk groups as well as between the intermediate-risk and high-risk groups was not statistically significant.
Comparison of Perioperative Outcomes in Patients Among Risk Groups Based on Zhongshan Score
Values are expressed as median (IQR) or n (%).
Kruskal–Wallis test for changes in blood creatinine and indwelling drainage tube; Fisher exact test for overall complications and three types of complications; and one-way ANOVA for other selected variables between the three groups.
Five patients who underwent open and radical treatment were excluded from the above metrics, except for the complications.
P < .05.
ANOVA, analysis of variance; Hb, hemoglobin; IQR, interquartile range.
Variables such as postoperative hemoglobin drop, changes in serum creatinine levels, OT, postoperative hospital stay, and indwelling drain time did not differ significantly across the three groups. Meanwhile, when the intergroup analysis of RENAL score indicators was conducted (Table 3), no significant correlation was found between the RENAL score and any of the aforementioned indicators.
Comparison of Perioperative Outcomes in Patients Among Risk Groups Based on Radius, Exophytic/Endophytic, Nearness, Anterior/Posterior, and Location Score
Values are expressed as median (IQR) or n (%).
Kruskal–Wallis test for changes in blood creatinine and indwelling drainage tube; Fisher exact test for three types of complications; Pearson's chi-square test for overall complications; and one-way ANOVA for other selected variables between the three groups.
Five patients who underwent open and radical treatment were excluded from the above metrics, except for the complications.
P < .05.
ANOVA, analysis of variance; Hb, hemoglobin; IQR, interquartile range.
With respect to total perioperative complications, 23 patients (23.2%) encountered intraoperative and/or postoperative complications. The top three complications included positive surgical margins (8.08%), conversion to open or radical procedures (5.05%), and intraoperative blood transfusions (3.03%). A significant correlation was observed between the increase in the ZS score risk group and the overall complication rate (P = .045).
Nevertheless, no statistical significance was detected among different ZS score groups regarding rates of positive surgical margins, conversion to open or radical procedures, and intraoperative blood transfusions. Conversely, when patients were grouped according to the RENAL score (Table 3), an increased RENAL score was associated with a higher risk of conversion to open or radical procedures (P = .012).
Table 4 illustrates the correlation between RENAL and ZS scores and primary surgical outcomes. Both RENAL and ZS scores showed significant correlations with overall complications (r: 0.233 and r: 0.252, respectively). Additionally, the RENAL score was linked to changes in blood creatinine levels (r: 0.218), and the ZS score was associated with WIT (r: 0.290).
Spearman correlation between Radius, Exophytic/Endophytic, Nearness, Anterior/Posterior, and Location and Zhongshan Scores and the Major Surgical Outcomes of Laparoscopic Partial Nephrectomy
P < .01.
P < .05.
Hb, hemoglobin; RENAL, radius, exophytic/endophytic, nearness, anterior/posterior, and location; ZS, Zhongshan.
Table 5 indicates that in the univariate analysis, aCCI, ZS, and RENAL scores were significantly related to the incidence of overall complications. In the multivariate analysis, only the aCCI score emerged as an independent predictor of overall complications, with the ZS and RENAL scores showing no statistical significance. The predictive capabilities of ZS and RENAL scores for overall complications were further evaluated using the ROC curve (Fig. 1).
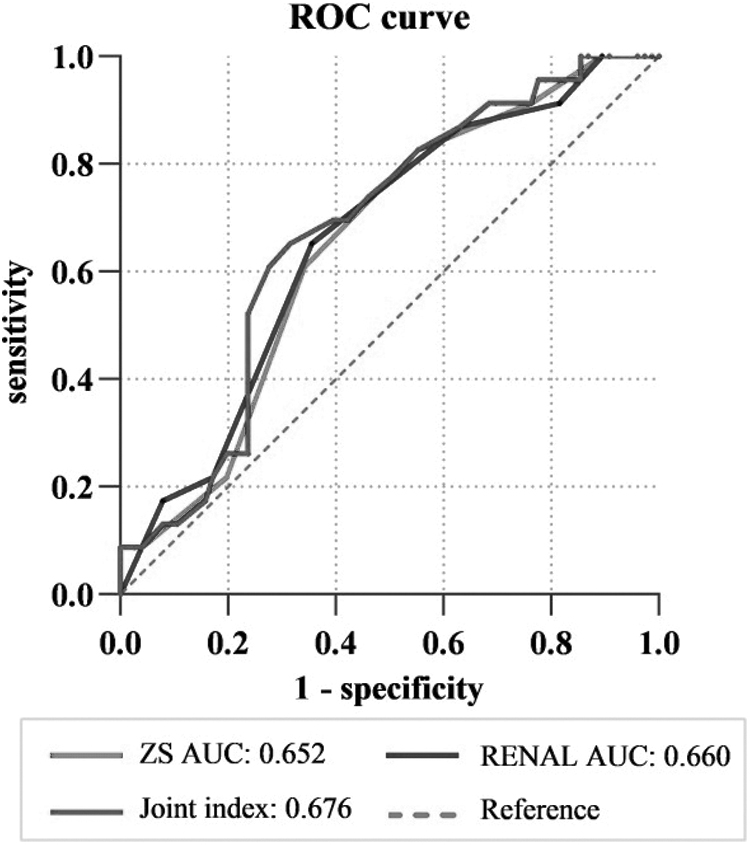
ROC curves of three parameters (ZS, RENAL, and joint index) used to predict overall complications. AUC, area under the curve; joint index, combination of ZS and RENAL scores; RENAL, radius, exophytic/endophytic, nearness, anterior/posterior, and location; ROC, receiver operating characteristic; ZS, Zhongshan.
Univariate and Multivariate Logistic Regression Showing the Accuracy of Potential Influencing Factors to Predict the Risk of Overall Complications
P < .05.
aCCI, age-adjusted Charlson comorbidity index; CI, confidence interval OR, odds ratio; RENAL, radius, exophytic/endophytic, nearness, anterior/posterior, and location; ZS, Zhongshan.
The AUC for the ZS score was 0.652, comparable with that of the RENAL score (AUC = 0.660). Combining ZS and RENAL scores did not significantly enhance the predictive accuracy for overall complications (AUC = 0.676).
Discussion
The 2022 European Society of Urology guidelines strongly advocate PN for localized T1 stage RCC. 3 A crucial aspect of PN surgery's success is the preoperative evaluation of renal tumor complexity. To this end, numerous researchers have proposed various renal tumor scoring systems. The first-generation systems, including RENAL, PADUA, and C-index scoring, are more widely adopted, but have notable limitations, such as complex scoring parameters and inclusion of less relevant items. 10
Consequently, Zhou et al. introduced the ZS score, streamlining the assessment of anatomical features of renal tumors. This score has been shown to surpass the RENAL and PADUA scores in predicting PN surgery's complexity and complications. By combining the branching pattern of the renal arteries and the ZS score, aiding precise segmental arterial blockade during PN surgery. 8
Nevertheless, the study encompassed open, laparoscopic, and robotic surgical approaches, each with differing levels of surgical complexity. Currently, there is no external validation of the ZS score in LPN cases. To our knowledge, this study represents the first external comparison between ZS and RENAL scores in LPN scenarios.
In our study, we observed a lower patient count in the low-risk ZS score category, with a more pronounced concentration in the intermediate- and high-risk groups. In contrast, categorization by the RENAL score revealed a substantial increase in the low-risk group and a notable decrease in the high-risk group. Previous studies, such as those by Zhang et al., have shown a significant association between the RENAL score and WIT. 11
Hayn et al. identified significant differences in WIT, estimated blood loss, and hospital stay duration across RENAL score groups. 12 However, we noted that the RENAL score was linked to overall complications and changes in blood creatinine levels. Additionally, we observed extended WIT and a higher incidence of overall complications in the ZS score's high-risk group, indicating that the ZS score may also reflect the complexity of the procedure to some extent.
In this study, the overall complication rate was 23.2%. The univariate analysis identified both ZS and RENAL scores as significant predictors of overall complications; however, multivariate analysis of the two was not statistically significant. Further evaluation using ROC curves to assess the predictive capacity of both scores for overall complications indicated no significant difference.
Moreover, combining ZS and RENAL scores to enhance prediction did not yield a notable improvement in predictive accuracy. This outcome could be attributed to the similarity in the scoring criteria of both systems, resulting in a degree of redundancy in assessing renal tumors.
The literature indicates a 1.2% (2/164) chance of RN in LPN. 13 Long et al. determined that for renal tumors with a RENAL score of 7 or higher, the risk of conversion to RN is significantly elevated, reaching 11.5%. 14 In our study, 2 patients (2.02%) underwent conversion to RN: 1 with a low RENAL score (5), but an intermediate ZS score (7), and other with high scores in both RENAL and ZS systems (10 and 12). Additionally, 3 patients (3.03%) required conversion to open PN, with intermediate- and high-risk scores in both ZS and RENAL systems, exceeding the reported literature incidence of 1.6%. 15
Furthermore, our findings indicate an increased likelihood of radical or open conversion as the RENAL score risk category escalates. For the ZS score, an intraoperative shift toward radical or open conversion with rising risk levels is anticipated, yet our study reveals this trend to be statistically insignificant. Despite ongoing debates about the criteria for selecting RN or open PN, our results imply that the RENAL score offers a more effective assessment in such cases.
The primary limitations of this study encompass its retrospective nature, being conducted at a single center, and a constrained sample size. Additionally, the focus on small renal lesions may restrict the evaluation of the ZS score's applicability to more anatomically complex renal tumors. Furthermore, the absence of radioisotope scanning—a more precise method than measurement of serum creatinine or estimated glomerular filtration rate for assessing renal function—might constrain the interpretation of certain results. 16
In summary, this study indicates that the ZS score, being simpler and more intuitive, can be as effective as the RENAL score in assessing renal tumor complexity and surgical difficulty. The combined use of both scoring systems could enhance prediction of tumor complexity and surgical outcomes in LPN.
Footnotes
Acknowledgments
The authors thank all their colleagues for the intensive studies in this research.
Authors' Contributions
Y.H. and S.Y. Huang were involved in conceptualization (lead); writing—original draft (lead); formal analysis (lead); and writing—review and editing (equal). C.G. and G.H. were involved in data curation (equal). Y.H. was involved in methodology (lead) and writing—review and editing (equal). Y.W. and S.X. were involved in supervision (equal) and writing—review and editing (equal). All authors have read and approved the content and agree to submit it for publication.
Data Availability Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.