
Abstract
Background:
A primary pull-through for Hirschsprung’s disease (HD) requires confirmation of normal ganglionic bowel by intraoperative biopsies to determine the level of resection. Despite this, aganglionic bowel that is not fully resected (so-called “transition zone pull-throughs”) is reported in 15%–19% of patients. We hypothesize that this may result from insufficient biopsies sent for intraoperative diagnosis.
Methods:
A new biopsy protocol has been developed in our institution for patients undergoing a laparoscopic-assisted endorectal pull-through for HD. Laparoscopic seromuscular biopsies are taken as per standard practice and are reported intraoperatively to identify the most distal site of ganglionic bowel. A 5 mm laparoscopic stapling device is used to divide the bowel at the proposed proximal resection margin and 2 cm distally. If there is any evidence of abnormality in the first doughnut, a second, more proximal doughnut is taken.
Results:
Between 2015 and 2020, 21 patients underwent a primary laparoscopic endorectal pull-through for HD using the doughnut biopsy protocol. Sixteen patients were male. The mean patient age at the time of surgery was 3 months (range 1–6 months), and the mean weight at the time of surgery was 6.5 kg (range 4.1–8.54 kg). In all 21 cases, initial laparoscopic biopsies were reported showing normal ganglionic bowel; in two cases (10%), the laparoscopic doughnut influenced the proximal resection margin. In both cases, aganglionic tissue was identified intraoperatively in the doughnuts, and a second, more proximal doughnut was sent. No patients had transition zone resections on final histology (mean clear margin 45.55 mm, range 11–72 mm).
Conclusions:
In conclusion, intraoperative frozen sections taken from doughnuts of bowel retrieved using 5 mm laparoscopic stapling devices are safe and have resulted in a 0% rate of transition zone pull-throughs while reducing the potential of spillage of enteric contents. We would recommend this protocol for all patients undergoing primary endorectal pull-throughs.
Introduction
Hirschprung’s disease (HD) was first described in 1888. 1 However, reports of the condition before it was formally defined may have been as early as 1691. 2 The condition develops due to a failure of neural crest cells to develop into the myenteric (Auerbach) plexus. The disease tends to develop in a craniocaudal manner, with milder variants only affecting the most distal colon and more severe forms affecting the entire gastrointestinal tract. 3
Hirschprung’s is diagnosed by rectal biopsy demonstrating distal aganglionic bowel. 4 The pathological hallmarks of the disease include the absence of neural ganglions, thickened nerve fibers, diffuse acetylcholinesterase staining, and/or the absence of calretinin staining. 3
Definitive surgery can include an end colostomy formed in ganglionic bowel, but most specialist surgical centers will attempt to perform reconstructive surgery utilizing a pull-through operation with rectal dissection using either the Swenson anal anastomosis, the Duhamel procedure or Yancey-Soave-Boley endo-rectal dissection. 5 During all pull-through surgeries, seromuscular biopsies are taken and are sent for intraoperative frozen section, to determine the extent of the aganglionosis and the amount of bowel to be resected. 6
With the advent of minimally invasive surgery, many centers in the U.K. now perform a primary endo-rectal procedure, either using a purely transanal dissection or with additional laparoscopic assistance. 7 In both cases, intraoperative seromuscular biopsy sampling is essential to determine the level of resection.6,8,9
Despite this, there remains a 10%–15% rate of operative failure defined as aganglionosis or the presence of a transition zone at the anastomosis.10–12 It has been suggested that this may be due to the aganglionosis not affecting the bowel circumferentially, with the mesenteric and anti-mesenteric surfaces not being representative of each other. 13 This may then result in normal ganglionic seromuscular biopsies being obtained from the anti-mesenteric bowel wall, when the mesenteric wall at the same level may be aganglionic.
As surgical technology has developed, there are now 5 mm stapling devices on the market suitable for resecting bowel in patients of <10 kg weight. We, therefore, hypothesized that a stapled, full-thickness final colonic biopsy will reduce the rate of aganglionic pull-through surgery for HD.
Materials and Methods
The data collection period ran between the 28th of July 2015 and 30th November 2019. This study was exempt from application to an institutional review board, as it was deemed to meet the standard for retrospective service evaluation. Patients involved in the study provided informed consent to having tissue and images used for research purposes. All patients undergoing a primary laparoscopic-assisted trans-anal pull-through procedure for HD were operated on using the doughnut biopsy technique. Data were collected retrospectively using a combination of operating theatre management software and electronic patient notes. Patients were excluded from the study if they did not have biopsy-confirmed HD at the time of surgery or were not having a primary laparoscopic operation. The primary outcome measures were the presence of ganglion cells at the resection margin. Secondary outcome measures were device-related intraoperative complications and postoperative complications. Data collected included patient age, sex, weight at surgery, doughnut pathology, and definitive pathology.
Surgical Technique
Patients underwent a laparoscopic-assisted transanal pull-through procedure. Following standard laparoscopic port insertion, seromuscular biopsies were taken and reported intraoperatively to identify ganglionic bowel. Proximal to the most distal ganglionic biopsy, a laparoscopic stapling device (JustRight 5 mm laparoscopic stapler, Boulder Surgery Inc £750/device) was utilized to excise a doughnut of colon (Fig. 1). On occasion, a standard 12 mm surgical stapler (Endo-GIA stapler, Medtronic £65/device), or an 8 mm powered stapler (Signia powered stapler, Medtronic £204/power shell, £147/reload), depending on what device was most appropriate for each patient. This was then sent for intraoperative pathological analysis with further full-thickness biopsies taken from all four quadrants.
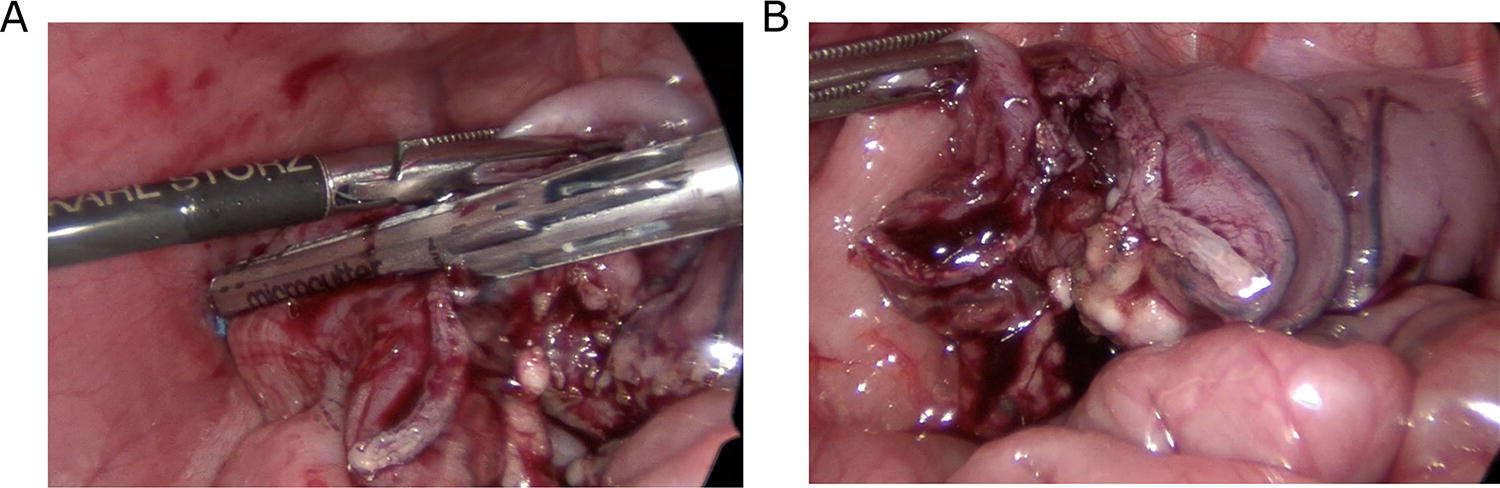
Intraoperative images taken during a laparoscopic-assisted endo-rectal pull-through procedure. Following intraoperative seromuscular biopsies have been taken and reported the colon is mobilised sufficiently to allow ganglionic bowel to reach the anus.
The proximal and distal bowel were then loosely sutured together using a white suture medially and a blue suture laterally to allow for identification of the correct orientation. The proximal colon was then mobilized on its mesentery to allow a tension-free pull-through to take place. The patient was then placed in the Lloyd-Davis position to perform a standard endo-rectal dissection. 14
During the procedure, the doughnut biopsies were sent for frozen section histology, and if found to display features of transition zone or were aganglionic, a further, more proximal doughnut of bowel was excised in the same way and sent for frozen section microscopy, ensuring circumferential ganglionation at the time of anastomosis (Fig. 2).

Diagrammatic Representation of the steps in acquiring a circumferential doughnut biopsy.
Results
During the 5 years of this study, 21 patients underwent a primary laparoscopic endorectal pull-through using the doughnut protocol. The mean age at surgery was 3.14 months (range .75 − 10). Mean patient weight was 6.51 kg (range 4.08–11.3), and mean follow-up was 24 months (range 2–53). The male-to-female ratio was 16:5 (Table 1).
Demographics of the Patients Operated on during the 5 Year Period the Doughnut Biopsy Technique Has Been Used
Initial doughnut histology was normal in 19 patients (90.5%), and transition zone was found in 2 patients (9.5%). Both patients with abnormal pathology had a second, more proximal doughnut found with subsequent normal histology. The mean distance from ganglionic bowel to the transition zone of the final resection specimen (excluding the already excised doughnut) was 54.7 mm (range 1–137 mm). The transition zone was most commonly located in the sigmoid colon (17 patients), followed by the rectum (2 patients), transverse colon (1 patient), and descending colon (1 patient) (Table 2).
The Results from the Excised Doughnuts of Tissue and Final Resection Specimen. In Total 9.5% of Patients Had Doughnuts Showing Abnormal Pathology, Who Would Have Subsequently Had Transition Zone Pull Throughs, Which Were Prevented by This Protocol
No patients suffered from intraoperative bleeding, spillage of enteric contents, or injury to visceral or vascular structures.
One patient (4.8%) with a diagnosis of trisomy 21 underwent a colostomy formation due to ongoing severe chronic constipation and enterocolitis. Repeat suction rectal biopsies and the subsequently resected colon showed the previous pull-through had been ganglionic throughout (Table 3).
Long and Short Term Complications of All Patients Undergoing the Doughnut Biopsy Technique. There Were no Intra Operative Complications Noted and One Patient with Trisomy 21 Required a Subsequent Colostomy Due to Chronic Constipation. Biopsies and Resection Specimen Showed That the Original Pull through Operation Was Ganglionic
Discussion
Previously published articles have identified the rate of aganglionic bowel at the resection margin at between 10%–15% of all pull-through operations performed for HD.10,12 These patients will typically develop clinical features of outlet obstruction post pull-through, with abdominal distension, refractory constipation, and recurrent enterocolitis, and rectal biopsies will confirm aganglionosis.10–12 Treatment is by redo pull-through surgery or end colostomy formation. It has been hypothesized by Jajagnir et al. that aganglionic pull-throughs may occur, in spite of ganglionic intraoperative biopsies, because the ganglionation of the colon may not be uniform, and aganglionosis may persist on the mesenteric aspect, while the ante-mesenteric border is ganglionic. 13 In these patients, a circumferential biopsy protocol, such as we have described, should all but eliminate the occurrence of an aganglionic pull-through at surgery. We have demonstrated a 0% aganglionosis rate, defined by a normal proximal resection margin at surgery and either an absence of outlet obstruction symptoms or normal post pull-through rectal biopsies, suggesting in this small study the potential benefits of obtaining an intraoperative circumferential biopsy.
During this study, 2 patients had doughnut biopsies, which demonstrated features consistent with the transition zone. In these patients a second, more proximal doughnut was sent, which showed normally ganglionic colon. These 2 patients represent 9.5% of the endorectal pull-through procedures performed. If the doughnut biopsies had not been taken, these patients would have presumably undergone transition zone pull-throughs. 9.5% is consistent with the reported rate of transition zone pull-throughs in the literature, and we believe that this finding confirms the advantage of a circumferential biopsy in eliminating the transition zone pull-through. The use of the doughnut biopsy protocol appears to have eliminated the 10% transitional pull-through rate widely reported in the literature and therefore prevented patients from having to undergo revisional surgery with associated morbidity and mortality.
Endorectal pull-through procedures do not require the bowel to be opened within the abdomen, minimizing the risk of enteric spillage and potentially reducing postoperative infection. 9 By using novel 5 mm laparoscopic stapling devices, we have managed to achieve a 0% enteric content spillage rate and a 0% rate of postoperative infection, successfully mitigating any risk that these extra operative steps involve.
This study is limited by its observational nature. To adequately assess the benefits of using a doughnut biopsy protocol over standard operative techniques, a randomized controlled trial would be most beneficial, with adequate power to see an effect. However, at our institution, this pilot study has resulted in such a striking reduction in aganglionic pull-throughs and postoperative complications that we would be unwilling to offer the previous biopsy protocol to our patients. This study has also involved only one center with an experienced laparoscopic colorectal surgery team and paediatric pathology team. Further studies will have to be performed to see if the same benefits are seen in different centers.
In conclusion, we have demonstrated in this study that a laparoscopic endorectal circumferential biopsy protocol is safe, does not lead to any increased complications, and may either reduce or eliminate the incidence of aganglionic pull-throughs in HD.
Footnotes
Acknowledgment
The authors wish to thank the patients and staff of the Royal Hospital for Children, Glasgow.
Authors’ Contributions
J.H.: Methodology, validations, formal analysis, investigations, resources, data curation, writing—original draft, visualization. C.E.: Validation, resources, writing—review and editing. G.W.: Conceptualization, methodology, resources, writing—review and editing. T.B.: Conceptualization, methodology, resources, writing—review and editing.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This project has received no funding.