
Abstract
Objective:
At present, the incidence of synchronous multiple primary lung cancer (SMPLC) is increasing, and the treatment is still a challenge. This study aims to investigate the appropriate surgical procedure for treating bilateral primary lung cancer simultaneously.
Methods:
A retrospective analysis was conducted on clinical data from 32 patients who underwent simultaneous bilateral lung cancer surgery in our team. This data included patient characteristics, pulmonary function indicators, surgical procedures, operation duration, chest tube removal time, postoperative hospital stay, and postoperative complications.
Results:
Out of the 32 patients, 15 were male, and 17 were female, with an average age of 56.4 ± 8.8 years. The average maximum diameter of the main and minor tumors was 1.8 ± 1.0 cm and 1.0 ± .5 cm, respectively. All surgeries were performed thoracoscopically through intercostal approach. The procedure for the minor tumor was performed first, followed by the main tumor operation after turning over. One case was converted to thoracotomy during the main tumor operation because of bleeding. Postoperative complications occurred in one patient. No instances of respiratory insufficiency or failure were observed after the operation, and there were no perioperative deaths or readmissions within 90 days.
Conclusion:
Simultaneous bilateral thoracoscopic surgery is deemed a secure and feasible option for eligible patients with bilateral primary lung cancer, and it is advisable to commence the operation on the minor tumor first.
Introduction
Currently, the worldwide incidence of synchronous multiple primary lung cancer (SMPLC) is on the rise, posing significant challenges in clinical practice. A retrospective study revealed that 7.9% of surgically resected nonsmall cell lung cancers and 8.4% of adenocarcinomas manifest with multiple lesions. 1 The occurrence of SMPLC in the general population spans from .2% to 8%, and autopsy studies have reported rates between 3.5% and 14%. 2 Surgical resection has shown favorable survival rates for patients with SMPLC.3–6 In cases where patients have multiple tumors on the same side, simultaneous surgery is recommended. However, in instances of bilateral tumors, a substantial debate persists regarding whether to proceed with simultaneous or staged surgery. Many surgeons favor staged surgery, expressing concerns over prolonged operative time and elevated risks. Although some studies have highlighted the feasibility of simultaneous bilateral surgery for carefully selected patients,6–10 global clinical guidelines for bilateral surgical management remain absent.
In this study, we conducted a retrospective analysis of the clinical data from 32 patients who underwent simultaneous bilateral lung cancer surgery carried out by our team. Our objective was to investigate the appropriate surgical procedure for treating bilateral primary lung cancer.
Materials and Methods
Data collection
We collected clinical data from 32 patients who underwent simultaneous bilateral lung cancer surgery and were admitted to our team since November 2016. Preoperative assessments included enhanced chest and brain computed tomography (CT), lung function tests, electrocardiograms, echocardiography, abdominal ultrasound, radionuclide bone imaging, bronchoscopy, and hematological examinations to exclude distant metastases and other surgical contraindications. Informed consent has been obtained from all individuals included in this study. The research was conducted in accordance with the tenets of the Helsinki Declaration and has been approved by the authors’ institutional review board.
Criteria for simultaneous bilateral surgery
Patients were considered eligible for simultaneous bilateral surgery if they satisfied the following criteria: 1. Diagnosis of SMPLC: Simultaneous bilateral pulmonary lesions must be confirmed as SMPLC. 2. Surgical indications: Indications for surgery on either side of the tumors must align with current clinical guidelines or expert consensus. 3. Resection strategy: The surgical approach for the main tumor should involve lobectomy or sublobectomy, whereas the minor tumor should undergo right middle lobe resection or sublobectomy. The main tumor is defined as the tumor requiring a more extensive lung resection, and the minor tumor necessitates less resection. In cases where the resection ranges are comparable on both sides, the left side tumor is designated as the main tumor. 4. Pulmonary function: Patients must exhibit pulmonary function adequate for the operation, with the following safety thresholds: percent of the predicted maximal voluntary ventilation (MVV%) ≥ 60%, percent of the predicted forced expiratory volume in 1 second (FEV1) ≥ 1.5L, percent of the predicted FEV1 (FEV1%) ≥ 60%, and percent of the predicted single-breath diffusing capacity of the lung for CO (DLCO SB%) ≥ 60%. 5. Patient preference: The patient must express the desire for simultaneous bilateral surgical treatment. In cases that do not meet these criteria, staged surgery or nonsurgical treatments are recommended. 6. The patient had no prior history of major surgery. 7. The patient had no prior history of other late-stage malignant tumor.
Surgical procedures
The patients underwent general anesthesia with double-lumen endotracheal intubation in the traditional lateral decubitus position. Thoracoscopic surgeries through the intercostal approach were performed. The operations commenced with the minor tumor. Subsequently, the patients were repositioned to the contralateral decubitus position for the main tumor operation.
The surgical procedures included one case of double lobectomy, one case of lobectomy and segmentectomy, 15 cases of lobectomy and wedge resection, four cases of segmentectomy and wedge resection, and 11 cases of double wedge resection. One case was converted to thoracotomy during the main tumor operation because of bleeding. Lymph node dissection was determined by the results of fast frozen pathology during the operation. Invasive adenocarcinoma cases underwent systemic lymph node dissection, microinvasive adenocarcinoma (MIA) cases had lymph node sampling, and lymph nodes were not dissected for adenocarcinoma in situ (AIS). All data were statistically analyzed using SPSS 20.0 software.
Results
Clinical characteristics of the patients
Out of the 32 patients, 15 were male, and 17 were female, with a mean age of 56.4 ± 8.8 years, ranging from 37 to 70 years. Nine patients had a history of smoking, and 19 patients had other concurrent diseases, such as diabetes, cardiovascular disease, cerebrovascular disease, or a history of surgery. All patients have no history of malignant tumors. The means of pulmonary function parameters were as follows: MVV% (91.1 ± 18.2%, ranging from 56.6% to 130.9%), FEV1 (2.7 ± .8L, ranging from 1.57 to 4.39L), FEV1% (104.1 ± 16.7%, ranging from 64.7% to 132.5%), and DLCO SB% (90.3 ± 13.1%, ranging from 70.5% to 117.8%) (Table 1).
Clinical Characteristics of the Patients
DLCO SB%, percent of the predicted single-breath diffusing capacity of the lung for CO; FEV1, forced expiratory volume in 1 second; FEV1%: percent of the predicted FEV1; MVV%, percent of the predicted maximal voluntary ventilation.
Imaging characteristics
Out of the 32 patients, 26 had two tumors, five had three tumors, and one had four tumors. The CT data of some patients are shown in Figure 1. The tumors included 11 solid nodules and 60 ground-glass opacities (GGO) (Table 2). The main tumor was located in the right upper lobe in 14 cases, left upper lobe in 6 cases, right lower lobe in 5 cases, left lower lobe in 4 cases, and right middle lobe in 3 cases. The mean maximum diameter of the main and minor tumors was 1.8 ± 1.0 cm and 1.0 ± .5 cm, respectively.
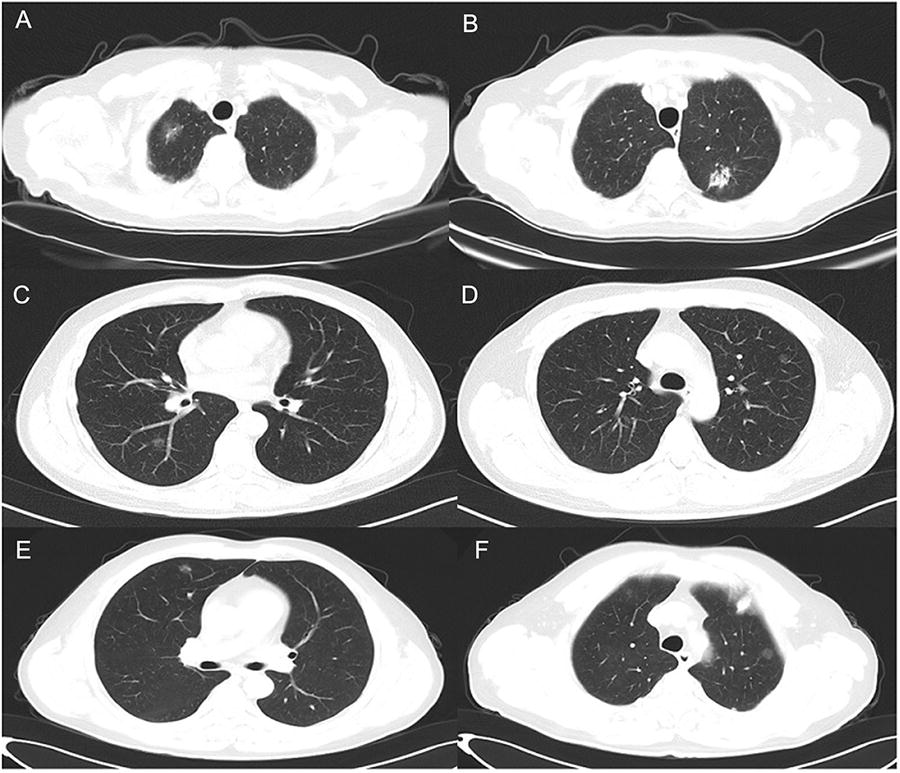
CT images of different patients.
Characteristics of the Tumors
AIS, adenocarcinoma in situ; GGO, ground-glass opacities; MIA, microinvasive adenocarcinoma.
Perioperative period
The mean operation time was 211.1 ± 73.7 minutes, ranging from 70 to 430 minutes. No major intraoperative bleeding occurred. Postoperatively, 31 patients had their tracheal intubations successfully removed and were transferred back to the ward, while one patient failed to have the tracheal intubation removed and was admitted to the intensive care unit (ICU) but returned safely on the second day. This patient was severely overweight and had undergone double wedge resection.
The average time for chest tube removal on the main tumor side was 2.9 ± 1.1 days, and on the minor tumor side, it was 2.3 ± 1.5 days. The mean duration of postoperative hospitalization was 5.7 ± 1.3 days. One patient, with severe pleural adhesions, experienced prolonged chest tube removal and hospital stay because of air leakage after the operation. This patient also developed lower extremity venous thrombosis and pulmonary embolism but was discharged following anticoagulant treatment. All other patients had a smooth recovery with no postoperative complications. There were no cases of respiratory insufficiency or failure, and no perioperative deaths or readmissions within the initial 30 days. Furthermore, there were no deaths or complications requiring readmission within the first 90 days following the operation.
Pathological results
All 71 tumors were diagnosed as adenocarcinoma (Table 2), comprising 31 cases of invasive adenocarcinoma, 26 cases of MIA, 13 cases of AIS, and one case of mucous adenocarcinoma. The TNM stages are shown in Table 2, and most of the tumors were in the early stage.
Discussion
With the rise in health awareness and the widespread availability of physical examinations, the detection of simultaneous bilateral multiple primary lung cancer has increased. Among surgeons, there remains a significant debate regarding whether to opt for simultaneous or staged surgery for patients suitable for surgical intervention. Although some studies have demonstrated the safety and feasibility of simultaneous bilateral surgery for selected patients, a fraction of surgeons still perceive high risks associated with simultaneous bilateral surgery, advocating for staged procedures. In reality, simultaneous bilateral surgery offers advantages, such as shorter hospital stays and lower costs. 11 Currently, there are no global clinical guidelines for simultaneous bilateral surgery. Our preference is to recommend simultaneous bilateral surgery for eligible patients and to explore the most optimal surgical approach for this procedure.
Foremost, the selection of eligible patients is pivotal to ensure the effectiveness and safety of surgical treatment.
First, an accurate preoperative diagnosis of bilateral primary lung cancer is essential. It is widely acknowledged that surgical outcomes for advanced lung cancer are considerably less favorable than for early-stage lung cancer; thus, it is imperative to rule out pulmonary metastasis of lung cancer. The concept and diagnostic criteria for SMPLC were introduced by Martini and Melamed in 1975. 12 In line with this, we have introduced an additional criterion: the presence of lung cancer manifesting as GGO on imaging. With the widespread use of CT screening, a substantial number of GGOs have been detected.13–16 Numerous studies have indicated that GGOs predominantly represent early primary lung cancers with a positive prognosis.17–21 We also maintain the belief that lung cancer presenting as GGO has a minimal likelihood of being a pulmonary metastasis. In our study, out of the 71 tumors, 60 were GGOs, and no metastases were detected in the dissected lymph nodes associated with these GGO tumors. This further underscores that lung cancer presenting as GGO predominantly corresponds to early-stage primary lung cancer.
Second, it is imperative to limit the overall extent of simultaneous bilateral lung resection within specific boundaries to prevent respiratory insufficiency or failure. We have devised a preoperative plan where lobectomy for the main tumor and sublobectomy for the minor tumor are considered safe for patients. Bilateral lobectomy should be avoided, except when the minor tumor is located in the right middle lobe, in which case right middle lobe resection in addition to a left lobectomy is deemed acceptable. Patients whose condition falls outside of this range are advised to undergo staged surgery or nonsurgical treatments. It is essential to emphasize that indications for surgery on either side of the tumors must align with current clinical guidelines. The scope of simultaneous resection should mirror that of staged surgery and should not be reduced because of the increased trauma associated with simultaneous surgery, as it could impact surgical outcomes. Sublobectomy was predominantly performed on tumors presenting as GGO. Previous evidence has shown that lung cancer presenting as GGO can achieve a high cure rate with sublobar resection.22–25 Patients with AIS and MIA who undergo sublobar resection without lymph node dissection can achieve a 5-year recurrence-free survival rate of 100%. 26 Therefore, lung cancer presenting as GGO is highly suitable for simultaneous bilateral surgery because of the limited resection scope and surgical trauma. The surgeries in our study included double lobectomy, lobectomy and segmentectomy, lobectomy and wedge resection, segmentectomy and wedge resection, and double wedge resection. Among these patients, there were no instances of respiratory insufficiency or failure.
Lastly, the patient’s pulmonary function must be able to withstand simultaneous bilateral surgery. Preoperative pulmonary function assessments are a critical measure to ensure the safety of thoracic surgery. However, previous studies have not outlined the criteria for pulmonary function indicators concerning simultaneous bilateral lung resection. We have set criteria, stating that when MVV% is ≥60%, FEV1 is ≥1.5L, FEV1% is ≥60%, and DLCO SB% is ≥60%, simultaneous bilateral surgery can be considered safe. These criteria are slightly more stringent than those for lobectomy. Consequently, our study reported no occurrences of respiratory insufficiency or failure after the operation, affirming the rationale and feasibility of these criteria.
In addition to the intercostal thoracoscopic approach, other techniques for bilateral thoracic surgery include the subxiphoid thoracoscopic approach27–29 and the median sternal approach. 30 However, we firmly believe that the intercostal approach stands as the most suitable option for the majority of surgeons.
In the past, the median sternal approach was commonly used in lung cancer surgery.30–32 However, with the increasing popularity of minimally invasive thoracoscopic surgery, this approach has become seldom used because of its substantial surgical trauma, except in a few specific cases. The advantage of the median sternal approach in bilateral lung surgery is its ability to avoid position changes. Nevertheless, it poses difficulties in exposing the entire pulmonary hilar region and its structures, particularly in dissections involving posterior anatomical areas such as S1 + 2, S6, S9, and S10 segmentectomies. Subcarinal lymph node dissection is even more challenging. In addition, patients subjected to the median sternal approach have a notably higher incidence of postoperative arrhythmia when compared with those undergoing the intercostal approach. 33 Given the extensive surgical trauma and these disadvantages, we do not recommend the use of this approach for simultaneous bilateral lung cancer surgery.
Subxiphoid video-assisted thoracoscopic surgery (SVATS) is a less painful alternative to intercostal thoracoscopic surgery. It is widely used in lung resection and mediastinal surgery in some centers worldwide. The main advantage of the subxiphoid approach is that it allows the resection of bilateral lesions through a single subxiphoid incision, reducing trauma and avoiding the need for intra-operative position changes. The subxiphoid approach has been shown to significantly reduce postoperative pain compared with the intercostal approach by preventing injury to the intercostal nerve.29,34–36 However, the subxiphoid approach is technically more challenging, especially in complex procedures. The limitations of the subxiphoid approach include the following:27,37–39 1. The subxiphoid approach requires long operating distances, demanding specially designed long-curved instruments and precise surgical techniques. 2. Access to posterior anatomical regions can be more challenging, especially in procedures like S1 + 2 and S6 segmentectomies on the left and S9 and S10 bilaterally. Dissecting the subcarinal lymph nodes, in particular, poses a significant challenge and has been a critical aspect in the learning curve of subxiphoid surgery. 40 3. Performing SVATS on the left side can be especially challenging, particularly in cases of cardiomegaly. Studies have indicated that the subxiphoid group experienced higher rates of intraoperative arrhythmias or hypotension because of compression on the heart.27,34,41 Therefore, preoperative patient selection for SVATS should avoid those with a history of cardiac disease or arrhythmia, especially those with left-sided lesions. 38 4. Controlling bleeding, separating dense pleural adhesions, dissecting enlarged or calcified lymph nodes, and performing complex operations through the subxiphoid approach can be more challenging than the intercostal approach. Consequently, SVATS procedures are frequently converted to conventional VATS or thoracotomy. 5. SVATS has been associated with longer operative time and increased blood loss compared with intercostal thoracic surgery.29,42 These limitations emphasize that the pursuit of esthetics and reduced pain should not overshadow technical challenges or major bleeding complications. Notably, even with careful patient selection and some of the most experienced VATS surgeons, conversion was necessary in 8.5% of cases, 41 which raise doubts about its safety in the hands of low-volume thoracic surgeons. So SVATS is not recommended for difficult pulmonary surgery by Chinese experts. Based on these, SVATS should not be the preferred choice for simultaneous bilateral surgery.
Conversely, the intercostal approach presents fewer limitations, rendering it a highly favored technique globally because of its lower technical demands and enhanced safety. This approach can be applied to nearly all types of lung cancer surgeries, particularly intricate and challenging procedures, and effectively addresses unforeseen scenarios like pleural cavity closure and significant vessel bleeding. Systemic lymph node dissection is comparatively straightforward, leading to a more comprehensive dissection. Despite the necessity of adjusting the patient’s position during surgery, we consider the intercostal approach as the optimal choice for simultaneous bilateral surgery.
The sequence of bilateral surgeries remains inconsistent, with some surgeons initiating procedures on the minor tumor,8,10 while others commence with the major tumor. 7 We advocate performing the operation on the minor tumor first. This process allows for the preservation of more normal lung tissue because of the smaller resection area, ensuring successful single lung ventilation during the subsequent operation on the contralateral major tumor. In our study, there were no instances of failed single lung ventilation during surgery.
Among the 32 patients, the oldest was 70 years old, and 19 had comorbidities. With the exception of one patient, the remaining 31 patients successfully had their tracheal intubations removed and were discharged to the ward post-surgery. Initial patients experienced longer postoperative hospital stays, primarily because of concerns regarding the greater trauma associated with simultaneous bilateral surgery and slower postoperative recovery. However, upon observation, it became evident that postoperative recovery after simultaneous bilateral surgery was not significantly impacted, leading to a substantial reduction in later hospital stays. Only one patient encountered complications, which resulted in extended chest tube retention and hospitalization. There were no cases of respiratory insufficiency or failure following the operation, and no perioperative deaths or readmissions within 30 days. Previous studies have also shown that the incidence of severe complications and perioperative mortality during simultaneous bilateral surgery is low. 6 Therefore, simultaneous bilateral surgery is a safe and feasible option for eligible patients.
The main limitations of the present study are the small sample size and retrospective analysis. Prospective large-scale clinical studies are needed in the future. Nevertheless, our study can serve as a valuable reference for thoracic surgeons for these patients.
Conclusion
In conclusion, simultaneous bilateral thoracoscopic surgery is a safe and viable option for patients with bilateral primary lung cancer who meet the eligibility criteria. A suitable surgical approach involves performing lobectomy or sublobectomy on the main tumor along with sublobectomy for the minor tumor. For most surgeons, the intercostal approach is recommended as the preferred method, and initiating the procedure with the minor tumor is advisable.
Footnotes
Authors’ Contributions
H.J. and M.B. designed and performed the study, and Y.Z. and Y.Q. collected and analyzed data. H.J. and M.B. wrote the article. H.J. supervised the clinical research and revised the article. All authors approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Shandong Province Medical and Health Technology Project (No.202304020338).