
Abstract
Purpose:
Surgery for choledochal cysts (CDC) in children younger than 6 months is relatively rare. We report our experience and compare the results between Da Vinci robot-assisted hepaticojejunostomy (RAHJ) and laparoscopic-assisted hepaticojejunostomy (LAHJ) in children younger than 6 months to treat CDC.
Methods:
A retrospective study was conducted on all children under 6 months of age who underwent RAHJ or LAHJ at the Children’s Hospital, Zhejiang University School of Medicine, from July 2018 to November 2023.
Results:
We reviewed 34 patients who underwent RAHJ surgery and 50 patients who underwent LAHJ surgery (P = .243). RAHJ group of the median operation time was 182 minutes (range 161–221), and LAHJ group was 168 minutes (range 143–191) (P = .02). The RAHJ group had a significantly shorter median postoperative hospital stay of 9 days (range 7–10) than the LAHJ group, 11 days (range 10–14), p < .001. The median hospitalization cost in the RAHJ group was significantly higher than that in the LAHJ group (75,474 CNY versus 28,984 CNY, p < .01). The median follow-up time was 18 months in the RAHJ group and 48 months in the LAHJ group (p < .01). All patients in the RAHJ group recovered well and were discharged. One patient in the LAHJ group developed biliary fistula 21 days after surgery and recovered well after reoperation.
Conclusions:
For children under 6 months old, on the basis of no consideration of cost, RAHJ has fast postoperative recovery and fewer postoperative complications, which is more recommended.
Introduction
Since the 1980s, the invention of radical resection of choledochal cysts (CDC) based on cyst resection and biliary tract reconstruction has created a new era of surgical treatment of CDC in modern times. 1 Since the first laparoscopic-assisted hepaticojejunostomy (LAHJ) in children was performed by Farello in 1995, 2 more and more general pediatricians have shown interest in this less invasive alternative to open surgery, which has advantages of less trauma, less bleeding, and faster recovery.3–6
However, as a surgical procedure with higher technical challenge and complexity, its learning curve is longer and difficult.7–9 Advances in robotic technology have facilitated the advent of Da Vinci robot-assisted hepaticojejunostomy (RAHJ), which allows easier and more precise trimming and reconstruction of bilioenteric anastomosis.10–12 At our center, as an alternative to open technology, LAHJ has been implemented since 2011 and RAHJ since 2020 to treat pediatric CDC. We share our experience and compare the results of these two minimally invasive techniques.
Methods
Patient population
Retrospectively, this study collected the medical records of all children under 6 months of age who underwent RAHJ and LAHJ at the Children’s Hospital, Zhejiang University School of Medicine, from July 2018 to November 2023.
Data on the children were collected from the hospital electronic records after obtaining ethics review board approval. The statistics obtained included patient demographics, clinical presentation, intraoperative characteristics, postoperative fasting time, length of hospital stay, hospitalization costs, and complications.
Patients and families were offered biliary reconstruction techniques for RAHJ or LAHJ, and the surgical approach was determined based on shared decision-making.
This study was approved by the Medical Ethics Committee of the Children’s Hospital, Zhejiang University School of Medicine. Transfer number: 2023-IRB-0296-P-01.
RAHJ surgical procedures
The anatomical area of the hepatic hilum was fully exposed by suspending the round hepatic ligament (Fig. 1A) and gallbladder (Fig. 1B) with 3-0 absorbable sutures. The gallbladder was gradually removed using an electrocoagulation hook, and the gallbladder artery was ligated to expose the biliary cyst, shown in Figure 1C. An incision was made in the anterior wall of the cyst to perform intracystic decompression while the aberrant bile duct opening could be explored, as shown in Figure 1D. The distal end of the cyst wall was elevated, and the cyst was gradually freed from proximal to distal end until the thin part close to the pancreatic duct was fully exposed, and the distal end of the common bile duct was dissected with a Hem-o-locking clamp, as shown in Figure 1E.

Procedure diagram of laparoscopic total choledochal cyst resection and Roux-en-Y hepaticojejunostomy.
Then, the stump of the proximal CDC was dissected upward to the common hepatic duct, and the tissue removed included the remaining cyst wall and gallbladder, as shown in Figure 1F. Trim the distal opening of the hepatic duct for anastomosis. The jejunum was fixed with intestinal forceps (15–20 cm from Treitz’s ligament) and pulled out of the abdominal cavity through a transumbilical incision. The proximal jejunal loop was closed; the appropriate length of the loop was assessed (measured as the straight-line distance between the umbilicus and the hepatic hilum), and the distal jejunal loop was anastomosed to the proximal jejunum. After the jejunum is placed in the abdominal cavity, the jejunal loop is elevated to the hepatic hilum through a tunnel created in the right mesocolon avascular zone of the transverse middle colic artery. A longitudinal incision of the intestinal wall was made 1 cm from the blind end of the jejunal loop, and the incision was the same size as the opening of the distal common hepatic duct, and “a biliary branch (this is not a true bile duct, but the jejunum, which is one of the branches of the Y, is used in Roux-Y to replace the original common bile duct and anastomose with the common hepatic duct)” was formed for reserve. As shown in Figure 1G.
The common hepatic duct and jejunal loop (biliary branch) were sutured with a full-thickness continuous suture using a PDS-II (5-0 absorbable suture) round needle, as shown in Figure 1H. After the closure, the anastomosis was checked again to visually evaluate the tightness of CJ reconstruction based on the deformation of the hepatic duct and jejunum. As shown in Figure 1I.
Statistical Analysis
IBM SPSS statistics version22 was used for statistical analysis. We performed Fisher’s exact tests for hypothesis tests for categorical variables and Wilcoxon-Mann–Whitney tests for hypothesis tests for continuous variables. For non-normal distribution data, with the median (IQR) to compare. In all analysis results, P < .05 was considered significant.
Results
During the study period, 84 children with CDC were divided into RAHJ (n = 34) and LAHJ (n = 50). One patient in the LAHJ group underwent reoperation 21 days after surgery due to biliary fistula. Patient and operative statistics are summarized in Table 1. In the RAHJ group, 31 cases were diagnosed prenatally, 1 case with jaundice, and 2 cases with abdominal mass, while in the LAHJ group, 38 cases were diagnosed prenatally, 5 cases with jaundice, and 5 cases with abdominal mass.
Patient Data Statistics Sheet
RAHJ, robot-assisted hepaticojejunostomy; LAHJ, laparoscopic-assisted hepaticojejunostomy.
The median operative time was 182 minutes (160.75–220.5) in RAHJ and 168 minutes (143–191.3) in LAHJ (P = .02). Figure 2. shows the effect of increased surgical experience on operative time in both groups. Compared with RAHJ, LAHJ had a steeper learning curve and shorter operation time with increased experience (r = −0.326, P = .021). In contrast, the RAHJ procedure time did not change significantly with increasing experience (r = −0.17, P = .924). The RAHJ had less intraoperative bleeding in the two groups, and the difference was statistically significant (P = .042). The duration of postoperative fasting was similar between the two groups (P = .795). The RAHJ group had a shorter postoperative hospital stay than the LAHJ group (P < .001). The RAHJ group had significantly higher hospitalization expenses than the LAHJ group (P < .01). All patients adhered to the postoperative follow-up. The median follow-up time in the RAHJ group was 18 months, and that in the LAHJ group was 48 months (P < .01).
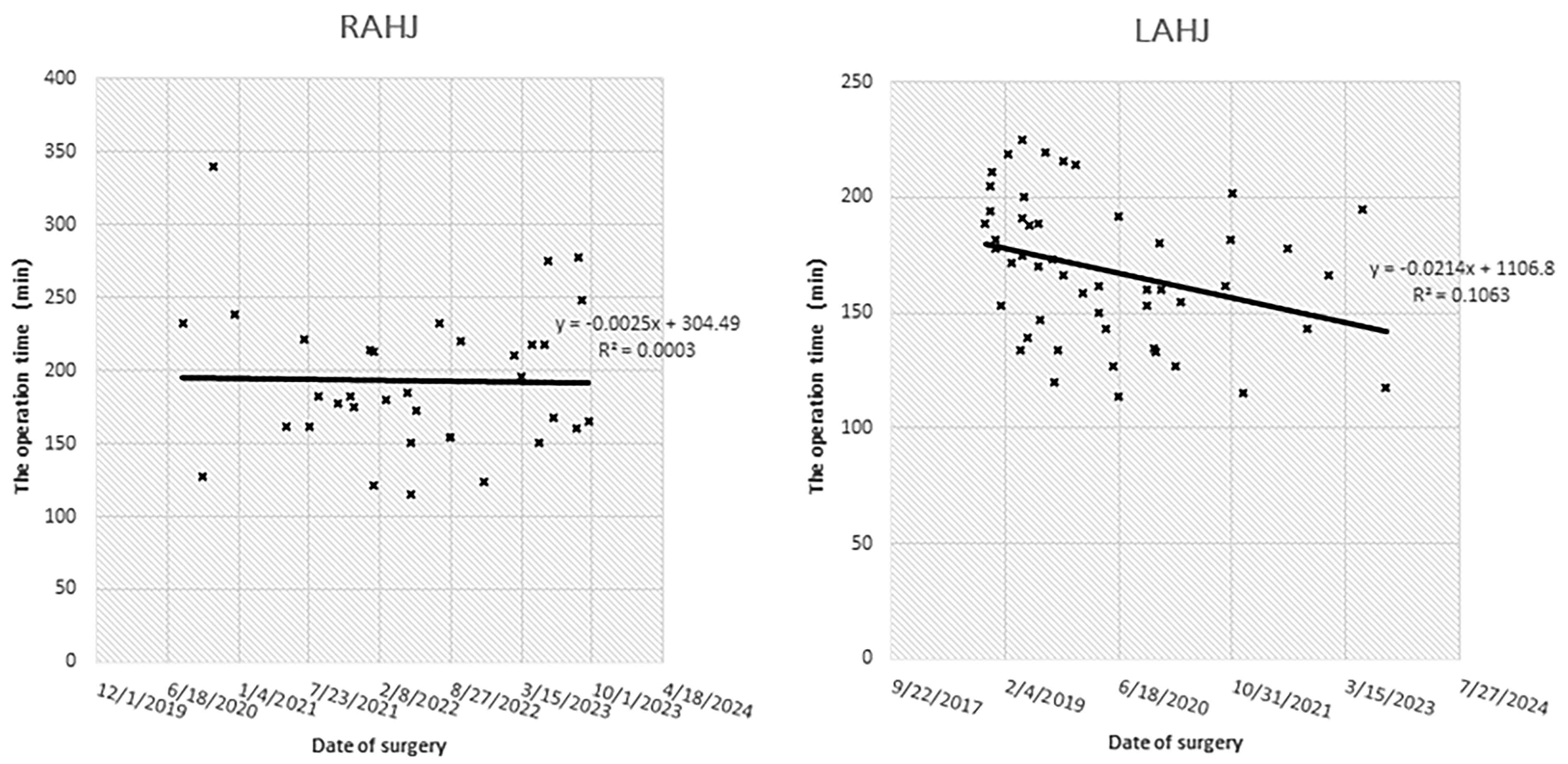
The effect of increased surgical experience on operative time in both groups. The RAHJ operation time did not change with the increase of experience (r = −0.17, P = .924). The LAHJ operation time shortened with the increase of experience (r = −0.326, P = .021).
The complication rate was 2% (1 case) in the LAHJ group and none in the RAHJ group. In the LAHJ group, a child aged 18 days had 30 to 40 mL of bile-like fluid in the abdominal drainage tube after surgery. After 21 days of conservative treatment, a biliary fistula was considered, and the patient recovered well after biliary fistula repair.
Discussion
In 1995, Farello et al. successfully performed the first successful LAHJ procedure on a 6-year-old girl of 14 kg. 2
As a new surgical method instead of open surgery at that time, laparoscopic surgery was recognized for its small trauma, quick recovery, and beautiful incision, but at the same time, it was difficult for some doctors to accept because of its high technical difficulty and long learning curve.7–9
Until 2006, Woo performed the first LAHJ in a child; 13 subsequent studies by Dawrant, Meehan, and Alizai et al., demonstrated greater ease of bile duct dissection, accurate clipping, and reconstruction of biliary branches, and the safety of successful use of robot-assisted surgery in a pediatric population.
In our hospital, we have implemented LAHJ since 2011 and RAHJ since 2020 for the treatment of pediatric CDC as an alternative to open techniques. Prior to the implementation of robotic techniques, there was considerable experience with laparoscopic surgery among our surgeons. Since early 2020, 4 surgeons have been surgically trained to perform the RAHJ. The youngest child in our series underwent LAHJ at 2 days of age, whereas the youngest child underwent RAHJ at 4 days of age. Jin et al. had reported a technically feasible RAHJ method, suitable for patients under 6 kg. 14
Compared with laparoscopic and open surgery, robotic surgery undoubtedly has technical advantages over traditional laparoscopic surgery. 15
First, robotic surgery includes 3D imaging, tremor filters, and articulated instruments, which allows it to overcome some of the limitations of laparoscopy and provide an enlarged 3D view. 15 Moreover, the more flexible and stable joint of the instrument eliminates the physiological tremor of the operator and enables the operation in a delicate space and ergonomic operating position. 16 With this advanced equipment, robotic surgery is superior to conventional laparoscopic surgery due to its significant improvement in visibility and manipulation.15,17,18
Robotic surgery is more advantageous in complex biliary reconstruction. Bustos et al. retrospectively analyzed 152 patients who underwent RAHJ and found a 2.6% incidence of bile leakage and a 3.3% incidence of stricture at a mean follow-up of 22.5 months. 10 Several studies have compared the clinical outcomes of robotic and laparoscopic biliary reconstruction in children. 11 Koga et al. compared 10 RAHJ and 27 LAHJ in children undergoing complete resection of CDC found that RAHJ had a shorter overall anastomosis time and a lower incidence of biliary fistula. Lee et al. compared laparoscopic and robotic choledochal cyst resection in 67 patients and found that robotic surgery had lower short-term complications compared with laparoscopic surgery (0% and 22.4%, respectively). 12 In our study, there was unfortunately only one biliary fistula (2%) in the LAHJ group, whereas all patients in the RAHJ group were discharged safely.
Some authors have reported a significantly shorter operative time in the RAHJ group compared with the LAHJ group in the learning curve. 19 But most of the studies so far have involved adults.
This is confirmed by our study. The authors suggest that the learning curve in RAHJ may be less steep compared with LAHJ, which may be related to the fact that at our institution, robotic surgeons are all more skilled in laparoscopic surgery, saving the adaptation process to spatial manipulation. Of course, as pointed out by Franco et al., it is also possible that this result is due to the faster knotting and easier suturing of RAHJ. 20
Conclusions
For children under 6 months old, on the basis of no consideration of cost, RAHJ has fast postoperative recovery and fewer postoperative complications, which is more recommended.
Footnotes
Acknowledgements
The authors thank the Information Department of the Children’s Hospital Affiliated to Zhejiang University School of Medicine for providing the data.
Authors’ Contributions
S.C. and Q.C. completed the conceptualization, formal analysis, drafting, approval, and accountability. Z.G. contributed to critical review, approval, and accountability.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Key R&D Program of Zhejiang (2023C03029).