
Abstract
Introduction:
The traditional method of performing open common bile duct exploration (OCBDE) was replaced by a less invasive procedure known as laparoscopic common bile duct exploration (LCBDE) in elective surgery. But at present, the application of this technique is considered novel and controversial to treat acute cholangitis (AC). The aim of our systematic review was to investigate the safety and efficacy of laparoscopic surgery in patients with AC.
Methods:
Studies containing information on patients diagnosed with AC who underwent LCBDE were included. A search for relevant articles was carried out, in the Cochrane Library, PubMed, and Google Scholar databases. All studies included in the systematic review were assessed using the Newcastle‐Ottawa Quality Assessment Scale.
Results:
A total of 10 studies were included. Seven were retrospective and three were prospective. Only one was a randomized controlled trial. There were three studies that compared elective LCBDE and emergency LCBDE. Two studies compared between primary closure and T-tube drainage. Two other studies focused on the comparison between LCBDE and OCBDE. One study examined the comparison of LCBDE and endoscopic retrograde cholangiopancreatography. Another study addressed the issue of conversion in LCBDE. One study compared early and delayed LCBDE. Conversion rates ranged from 0% to 16.92%. Morbidity ranged from 0% to 26.3%, and mortality ranged from 0% to 3.07%. There was no difference in terms of retained, residual, or recurrent stones, bile leak, hemorrhage, and postoperative pancreatitis, and this, comparing the different groups of patients. Bile duct and intestinal injuries as well as biliary stricture were not common. The average length of hospital stays was approximately 5.86 days, ranging from 2 to 11.12 days.
Conclusion:
The one-stage urgent LCBDE, while subject to debate, proves to be a secure, feasible, approach for managing nonsevere AC.
Introduction
Acute cholangitis (AC) is a potentially life-threatening infection of the bile ducts, which may be caused by biliary obstruction, due to various benign diseases, such as bile duct stones, or cancerous causes.1,2
The presence of the clinical Charcot’s triad, pain–fever–jaundice, highly suggests the diagnosis of an AC. However, due to its low sensitivity in making the diagnosis, it is now recommended to use the Tokyo Guidelines 2018 (TG18) diagnostic criteria as it enables the detection of a larger number of patients with suspected AC. 2 According to the TG18, a systematic diagnostic approach that involves a combination of clinical features, laboratory data, and imaging findings is recommended for the diagnosis of AC. 2
Management of AC is an emergency treatment that is based on two basic measures: antimicrobial drug therapy and bile duct drainage. 1
Drainage is critical for preventing septic shock, death, and complications such as hepatic abscesses, and it can also enhance the effectiveness of antibiotics. There are various methods for drainage, including surgical treatment, endoscopic drainage through endoscopic retrograde cholangiopancreatography (ERCP) or echo-endoscopy with the use of metallic or plastic stents, naso-biliary drain installation, or percutaneous transhepatic biliary drainage. 1
According to the TG18, endoscopic drainage is the preferred first-line approach, regardless of the severity of the condition. This recommendation applies especially to patients with severe AC, but there are some cases of mild AC where antibiotics and general supportive care may be sufficient. 3
However, ERCP may not always be effective in removing blockages from the common bile duct (CBD), which can require further surgical intervention (either open or laparoscopic). Factors that can contribute to the failure of ERCP include the presence of peri-ampullary diverticula, multiple or large stones in the CBD, impacted stones, stones located higher up in the duct, the presence of a T-tube, a previous Billroth-II surgery, an acute angulation in the distal CBD, and patients who are aged 85 or older. 4
Furthermore, the use of the ERCP technique can result in significant complications such as duodenal perforation, pancreatitis, and bleeding. 5
Since 1990, the traditional method of performing open common bile duct exploration (OCBDE) was replaced by a less invasive procedure known as laparoscopic common bile duct exploration (LCBDE). 6
According to literature, the OCBDE procedure has been linked to increased rates of complications, including the development of incisional hernias, wound infections, thromboembolisms, pulmonary complications, and postoperative pain. Additionally, studies have found various rates of biliary leakage and mortality associated with OCBDE. 4
Over time, as surgeons became more experienced with laparoscopic procedures, the LCBDE technique was increasingly utilized to address cases of cholangitis related to common bile duct stones (CBDS). 5 But at present, the application of this technique for individuals with AC is considered novel and controversial. 6
To our knowledge, there is a lack of consensus among medical professionals regarding the feasibility and safety of laparoscopic surgery in AC cases. Nevertheless, it is important to study the feasibility of this one-stage procedure in AC as it could potentially offer several benefits over open surgery, including less postoperative pain, faster recovery time, and reduced risk of complications. Moreover, with advancements in laparoscopic techniques and equipment, it is necessary to evaluate its safety and efficacy in treating AC, which could potentially lead to improved patient outcomes and better overall management of the condition.
For the above reasons, we have chosen this subject to investigate the safety and efficacy of laparoscopic surgery in AC and contribute to the existing literature on this topic.
Methods
The systematic review was conducted according to the 2020 guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and followed the recommendations of the Cochrane Handbook for Systematic Reviews and Interventions. A priori protocol was published in PROSPERO (ID: CRD42023456140).
Eligibility criteria
Studies included in this systematic review were chosen according to PICOs criteria.
Patients (P) were included if they had undergone LCBDE for AC. The diagnosis of AC was made according to the TG 2018, which is a combination of clinical features, laboratory data, and imaging findings.
There was no restriction of patients based on the severity of the AC, the method of exploration (choledocotomy or transcystic approach), and closure of the CBD (primary closure [PC] or T-tube drainage).
All interventions (I) or observations with or without control (C), studying at least one of these outcomes (O) were included: morbidity, mortality, duration of surgical procedure, retained stones, conversion, retained and residual stones, postoperative bile leak, postoperative pancreatitis, hemorrhage, stone recurrence, bile duct injury, biliary stricture; and length of postoperative hospital stay.
Search strategy
The Cochrane Library, PubMed, and Google Scholar databases were searched, using a combination of the following terms with the Boolean AND/OR operators: choledocholithiasis, CBDS, CBD exploration, laparoscopic, minimally invasive, laparoscopy, emergency, AC. We selected articles published up to 28 February 2023. Also, references to all retrieved articles were consulted for further relevant studies.
Data extraction
The search was conducted separately by two independent authors (M.M. and I.B.), and articles were screened for relevance based on title and abstract. Full texts of potentially eligible publications were obtained. If two separate publications included the same cohort of patients, the largest study was included in the analysis. Data were extracted by one author (I.B.) with complete and independent verification by a second author (M.M.). Disagreements were resolved through discussion.
Quality assessment
All included studies in the systematic review were assessed using the quality assessment of enrolled study was conducted through the Newcastle‐Ottawa Quality Assessment Scale (NOS). It consists of three aspects: selection, comparability, and outcome assessment. The maximum score was 9. Studies with NOS values greater than 6 indicated acceptable quality studies.
Definitions
Residual stones are defined as stones that persist, including cases of stone relapse diagnosed within the first 6 months after surgery. 7
Stone recurrence is defined as the occurrence of choledocholithiasis diagnosed 6 months or more after the surgical procedure. 7
Regarding retained stones, they were defined as stones that persisted at the end of the procedure.
Results
Literature search results
Using the predefined search strategy, the electronic database and manual searches retrieved 1107 potentially eligible studies. After removing duplicates and screening the title and abstract, a total of 10 studies were included.5–14
The search and study selection history are summarized in the PRISMA flow diagram (Fig. 1).
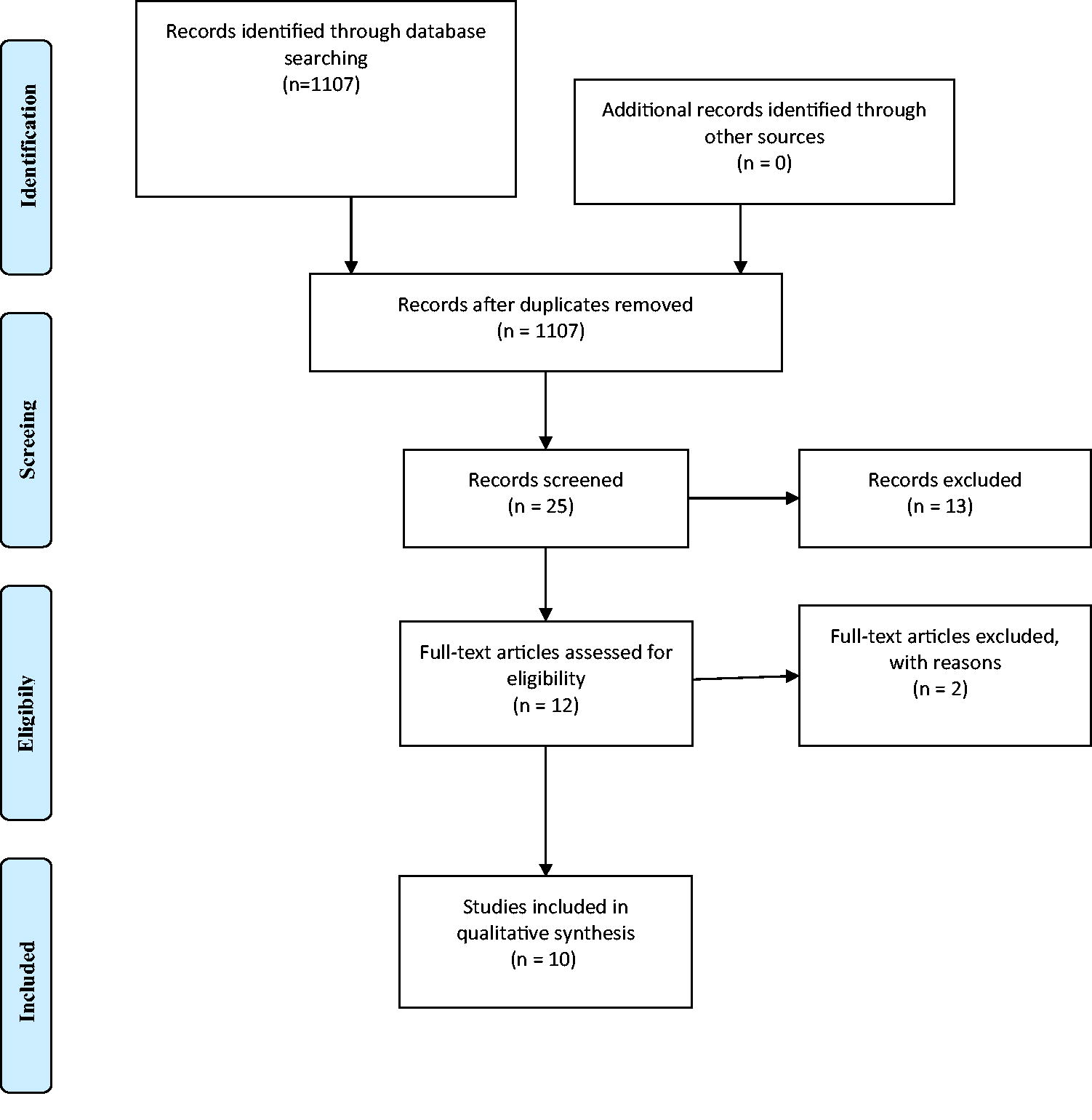
PRISMA flow diagram.
Among these studies, seven were retrospective5,7,9–12,14 and three were prospective.6,8,12 Only one 8 was a randomized controlled trial (RCT). The number of patients included varied from 37 to 255 with an average of 103.9 patients.
Seven studies5,6,8–12 focused on nonsevere cholangitis, of which five specifically mentioned T13/18 grades.5,8–11 The severity degree of the included cholangitis was not specified in the other three studies.7,13,14
In total, there were three studies that compared elective LCBDE (ElLCBDE) and emergency LCBDE.11–13 Additionally, two studies conducted comparisons between PC and T-tube drainage.5,10 Two other studies focused on the comparison between LCBDE and OCBDE in case of AC.6,14 Furthermore, there was one study that specifically examined the comparison of LCBE and ERCP. 8 Another study addressed the issue of conversion in LCBDE. 7 Finally, one study compared early and delayed LCBDE 9 in patients with AC. (Table 1).
Studies Characteristics
LCBDE all causes combined.
Emergencies including cholangitis that required LCBDE.
Choledocotomy with or without a drainage.
Total emergent LTCBDE.
AC, acute cholangitis; ACS NSQIP, American College of Surgeons National Surgical Quality Improvement Program; ERCP, endoscopic retrograde cholangiopancreatography; LCBDE, laparoscopic common bile duct exploration; N/A, not available; OCBDE, open common bile duct exploration; PS, prospective study; RS, retrospective study; TG, Tokyo Guidelines.
Outcomes
Complications
Conversion
Six studies6–11 reported conversions with rates ranging from 1.03% to 16.92%. Two studies had no cases of conversion,12,13 whereas two others did not mention conversion in their results5,14.
Postoperative Outcomes
Residual stones included persistent stones and also stone relapses diagnosed during the first 6 months after surgery. 7
Stone recurrence was defined as any choledocholithiasis diagnosed 6 months or more after surgery. 7
Persistent stones at the end of procedure.
Emergencies including cholangitis that required LCBDE.
LCBDE all causes combined.
LCBDE, laparoscopic common bile duct exploration; N/A, not available.
The main reasons for conversion to open surgery were the unclear anatomy,8,9 the presence of adhesions,8–11 the difficulty of dissection,7,10 the inability to extract the stones,6,7 uncontrolled hemorrhage,7,11 and digestive perforation. 6
The conversion rate was similar, and there was no difference between the emergency LCBDE group and the ElLCBDE group (respectively, 0.1% versus 0.5%) in the study by Czerwonko et al. 9
In the study by Llorente et al., 7 which included 52 cases of cholangitis, emergent LCBDE (EmLCBDE) for AC did not significantly influence the conversion to open surgery with a P value of .083 in the univariate analysis and P = .179 in the multivariate regression. Only three patients required conversion for EmLCBDE and ElLCBDE all combined.
The conversion to open procedures in the study of Alhamdani et al. 13 was observed exclusively among the elective patients than the EmLCBDE group, and this difference had statistical significance (P = .034).
Morbidity
The included studies revealed a wide range of overall postoperative complications, ranging from 0% to 26.3%, including cardiopulmonary complications, thromboembolism, wound infections, and bile leaks associated with LCBDE. Comparatively, OCBDE showed higher rates of associated morbidity than LCBDE, with a statistically significant difference reported in Halawani et al.’s study (P value < .0001). 14
In the study by Zou et al., comparing ERCP and LCBDE, no significant differences were found in postoperative ventilation duration between the two patient groups (P > .05 for all). 8
Regarding LCBDE, the PC and T-tube approaches showed no statistically significant difference in higher morbidity based on the two related reviewed studies.5,11 Specifically, Jiang et al.’s study found similar rates of incision infection (1.1% versus 2.2%, P = .649), pneumonia (2.1% versus 1.4%, P = 1.000), and cholangitis (1.1% versus 2.9%, P = .651) in both groups. 11 Similarly, in Zhu et al.’s study comparing early and delayed LCBDE, no statistical difference in morbidity was observed between the two groups. 12
Mortality
There was no mortality in six studies,5,6,8,9,11,12 whereas it ranged from 0.5% to 3.07% in three studies10,13,14 and was not reported in one study. 7
In their study, Halawani et al. compared the clinical outcomes between LCBDE and OCBDE and found that OCBDE was associated with a statistically significant increase in mortality (P value = .02). 14
In the study conducted by Alhamdani et al., 13 a comparison was made between EmLCBDE and ElLCBDE procedures. The findings revealed that there was no significant difference in terms of complications and mortality between the two groups (P = .71). The study reported only one death (2.08%) in the EmLCBDE group. 13
Retained stones
Retained stones were documented in seven studies,5–7,9,10,12,13 whereas they were either not present or not reported in three other studies.8,11,14 Note that Jiang et al. 11 defined retained stones at the end of the procedure as residual.
In the study conducted by Llorente et al., 7 a retrospective cohort of patients undergoing LCBDE was included. This study reported the highest incidence of retained stones, with 13 patients having persistent stones remaining at the end of the procedure.
When comparing ElLCBDE and EmLCBDE, Czerwonko et al. 9 did not find any significant difference in relation to retained stones (P = .972).
The results of Wang et al.’s study 5 comparing PC versus T-tube drainage in LCBDE for the treatment of acute mild cholangitis showed that the rate of retained stones was 2.75% (7/255), and there was no significant difference between the two groups (P = .366).
Comparing the early versus the delayed LCBDE in the treatment of nonsevere cholangitis, Zhu et al. 12 found that there was not a significant difference between the two groups in term of retained stones (P = .702). In his study which included 73 cases of acute lithiasis cholangitis, the persistent stone rate was 10.95%.
Residual stones
The study of Jiang et al., 11 involving 230 patients with nonsevere AC related to CBDS, identified 15 cases of residual stones (6.5%). The objective of their research was to compare the outcomes of PC and T-tube drainage following LCBDE. Their findings revealed that T-tube drainage resulted in a significantly higher occurrence of residual stones compared with PC (P = .029).
In their randomized controlled study that compared EmLCBDE + laparoscopic cholecystectomy (LC) and ERCP + LC for treating cases of choledocholithiasis with AC, Zou et al. 8 found one case of residual stone in the laparoscopic group compared with three cases in the ERCP group. However, this difference was not statistically significant (P = .305).
In Llorente et al.’s study, 7 which included 52 cases of cholangitis out of 357 LCBDEs for confirmed CBDS, 18 cases of residual stones were reported. Among these, 13 retained stones were also classified as residual.
These studies,5,6,9,10,12–14 either did not provide any data on the rate of residual stones or reported zero cases of them.
Bile leak
Bile leakage was reported by eight authors,5,7–13 while it was absent or not mentioned by two others.6,14
In the study conducted by Zhu et al. 12 the rate of postoperative bile leak was 8.2% for a total of 73 patients treated for nonsevere cholangitis laparoscopically. Furthermore, there was no difference statistically between the early versus the delayed groups (9.4% versus 7.3%), P = .751.
Biliary leakage occurred in 3.9% of patients who had LCBDE for nonsevere cholangitis in the study of Jiang et al., 11 and there was no difference between the PC or T-tube drainage groups (4.3% versus.3.7%), P = 1. Same for the case of Wang et al. study 5 where a total of 255 patients who underwent LC + LCBDE via choledochotomy for CBDS-related AC were evaluated. The rate of bile leak was 3.1%.
In the study by Llorente et al., the rate of biliary leakage reached 7% with a predominance of International Study Group of Liver Surgery’s type A. This rate did not significantly influence the resort to conversion (P = 1). 7
The rate of bile leakage in the study of Czerwonko et al. 9 was statistically similar in both ElLCBDE and EmLCBDE groups (0.4% versus 1%, P = .642). Whereas, it was lower in the ERCP + LC group than in the LCBDE + LC group: Zero versus five cases (12.5%) for treating AC in the study of Zou et al. 8 and the differences were statistically significant (P = .021).
Postoperative pancreatitis
In the study of Czerwonko et al. 9 which included 63 cases of nonsevere AC among 500 patients who had laparoscopic transcystic common bile duct exploration (LTCBDE), postoperative acute pancreatitis (AP) had been the most common complication (3.8%). A total of 11 patients had postoperative AP in the emergency pool.
The occurrence of postoperative pancreatitis was statistically more common in the emergency group in the univariate analysis, but was not of statistical significance (1.9% versus 3.8%, P = .062). 9
In the majority of cases, characterized as mild edematous AP, conservative management alone proved sufficient.
Among the studies included in this systematic review, only Czerwonko et al. 9 had reported cases of postoperative AP.
In the study conducted by Zou et al., 8 ERCP + LC led to seven cases of postoperative pancreatitis, whereas LCBDE + LC resulted in none. This difference was found to be statistically significant (P = .006).
Hemorrhage
In the study conducted by Zou et al., 8 one case of postoperative hemorrhage was documented after LCBDE. Notably, the ERCP procedure resulted in a higher incidence of hemorrhage in the treatment of cholangitis associated with CBDS, with a statistically significant correlation (P = .048).
Jiang et al. 11 investigated 230 cases of nonsevere AC, reported two cases of intraoperative bleeding requiring conversion to open surgery and two cases of postoperative bleeding successfully managed using nonsurgical methods.
In Wang et al.’s study, 5 which included 255 patients with CBDS-related AC, the average estimated intraoperative bleeding volume was approximately 40 mL. Postoperative bleeding, identified through peripheral blood testing and/or fecal occult blood tests, occurred in 1.96% of patients but could be effectively controlled using hemostatic drugs.
Czerwonko et al., 9 Aawasj et al., 10 and Halawani et al. 14 conducted studies involving emergencies requiring LCBDE. In these studies, 2, 3, and 20 patients, respectively, experienced incidents of bleeding.
Gholipour et al. 6 reported a single laparoscopic procedure in which intraoperative bleeding resulted from cystic artery damage, successfully managed using laparoscopic techniques.
In the study conducted by Llorente et al., 7 intraoperative bleeding occurred in eight patients (15.7%) and was a cause of conversion.
The remaining studies12,13 either did not observe any cases of intra- or postoperative bleeding or did not provide explicit mentions of such occurrences.
Intestinal perforation
Intestinal perforation was a rare occurrence across the included studies, as it was either not mentioned or absent in all of them except for one. Jiang et al. 11 documented a single case of small intestinal perforation, which resulted in the need for conversion to open surgery.
Stone recurrence
In the study conducted by Jiang et al., 11 two patients experienced recurrent stones, accounting for 0.87% of the total cholangitis cases included. Both cases underwent treatment via ERCP, and no significant differences were found in terms of stone recurrence between the T-tube and PC groups (P = .515).
Wang et al. 5 observed a stone recurrence rate of 5.1% in their study. Out of the 13 patients with recurrent stones, four required reoperation. Their findings indicated no significant difference in the stone recurrence rate between the PC and T-tube drainage groups (P = .524).
These two studies7,9 involved cases EmLCBDE. The number of patients with recurrent stones ranged from 10 to 30 in these studies. Czerwonko et al. 9 found that there was no statistically significant difference in terms of recurrent stones when comparing EmLCBDE and ElLCBDE (P = .844).
However, the rate of stone recurrence was either negligible or not mentioned in these six studies.6,8,10,12–14
Bile duct injury
In the research conducted by Czerwonko et al., 9 a single patient from the emergency LTCBDE group experienced a CBD injury. However, this injury was promptly identified and successfully repaired during the surgery, resulting in no additional complications.
It is worth noting that none of the other authors5–8,10–14 reported any biliary injuries or made mention of them in their respective papers.
Biliary stricture
Among the studies included, only Llorente’s 7 study provided information on postoperative biliary strictures. Biliary stricture was identified in two patients (0.6%) during the follow-up.
In contrast, the remaining studies either reported no cases of biliary strictures in their follow-up or did not provide any relevant data on this aspect.5,6,8–14
Hospital stays
Nine authors have investigated the duration of hospital stays following LCBDE. The average length of these stays was approximately 5.86 days, with a range spanning from 2 to 11.12 days.
In the study conducted by Zou et al., 8 ERCP resulted in a longer hospital stay than LCBDE (9.59 versus 8.76 days), but this difference did not reach statistical significance (P = .163).
Zhu et al. 12 found no significant difference in postoperative hospital stay between early and delayed LCBDE (11.91 ± 5.78 versus 10.33 ± 8.09 days, P = .355).
From the perspective of laparoscopic approaches, the length of postoperative hospital stay was shorter in the PC group compared with the T-tube group (6.59 ± 1.34 days versus 8.81 ± 1.85 days, P < .01) in the study by Wang et al. 5 The same result was observed in the study by Jiang et al., 11 where the difference was also significant (P < .001).
Studies featuring two arms and comparing hospital stays following either EmLCBDE or ElLCBDE indicate that patients tend to have a shorter hospital stay following ElLCBDE, as demonstrated in the study by Czerwonko et al., 9 where this difference was statistically significant (P < .001).
In contrast, the study by Alhamdani et al. showed that the length of postoperative stay was similar in the emergency group (ranging from 1 to 20 days) and the elective group (ranging from 1 to 17 days), with a median of 3 days in each group, and no significant difference was observed (P = .571) (Table 2).
Discussion
Main results
In this study, we have systematically reviewed and critically analyzed the published information about LCBDE used to treat AC from 2007 to 2023. We looked at a total of 10 articles. These studies were conducted in diverse centers worldwide, each adhering to its unique set of protocols.
Our data analysis revealed that the laparoscopic management of AC was correlated with acceptable mortality rates ranging from 0% to 3.07%.
The studies that underwent review revealed a wide spectrum of postoperative complications, spanning from 0% to 26.3%. These complications included various aspects such as cardiopulmonary problems, thromboembolism, wound infections, and bile leaks linked with laparoscopic exploration of the CBD.
Conversion rates ranged from 0% to 16.92%. The main reasons were unclear anatomy, adhesions, tough dissection, stone extraction problems, bleeding that couldn’t be controlled, and digestive injury. The rate of conversion to open surgery was the same for both urgent and planned LCBDE groups. Performing emergency LCBDE for AC didn’t significantly increase the need to convert to open surgery.
The rate of retained stones was similar in both urgent and ElLCBDE. Additionally, there wasn’t a significant difference in retained stones when comparing early and delayed LCBDE, or when comparing PC versus T-tube drainage for AC.
On the other hand, the number of residual stones appeared to be higher in ERCP group comparing with LCBDE. Additionally, our review found out that T-tube drainage resulted in a higher occurrence of residual stones compared with PC.
Bile leakage rates were similar in both ElLCBDE and EmLCBDE groups. Also, the timing of surgery (early or delayed) didn’t affect leakage rates. The way the bile duct was managed (PC or T-tube) didn’t show a difference either. However, leakage was less with a combined ERCP + LC group compared with LCBDE + LC group, and this difference was important.
Only one study in our review had reported cases of postoperative AP. The occurrence of postoperative pancreatitis was statistically more common in the emergency group, but was not of statistical significance. Furthermore, we found that ERCP is more likely to induce pancreatitis than LCBDE, and this difference was statistically significant.
Our review found that the ERCP procedure resulted in a higher incidence of hemorrhage in the treatment of cholangitis associated with CBDS, with a statistically significant correlation compared with the laparoscopic group. Other cases of hemorrhage, whether they were intraoperative or postoperative, were effectively managed using surgical or nonsurgical methods.
None of the related studies reported cases of intestinal injury except for one, in which a single case of small intestinal perforation occurred, necessitating conversion to open surgery.
Only four of the included studies mentioned stone recurrence. Our review revealed that there was no statistically significant difference in terms of recurrent stones when comparing EmLCBDE and ElLCBDE. From the perspective of laparoscopic approaches, no significant differences were observed in terms of stone recurrence between the T-tube and PC groups.
Bile duct injury was not a common complication in the studies we reviewed. In fact, only one study reported a single case of bile duct injury. This injury was identified and successfully repaired during the surgery, resulting in no additional complications.
Regarding biliary strictures, only one study offered information about this outcome. In this study, a total of two cases of postoperative biliary strictures were reported when considering both EmLCBDE and ElLCBDE cases combined. The remaining studies either reported no cases of biliary strictures in their follow-up or did not provide any relevant data on this aspect.
The average length of hospital stays was approximately 5.86 days, ranging from 2 to 11.12 days. While ERCP led to a longer hospital stay than LCBDE, this difference did not achieve statistical significance. Comparatively, the postoperative hospital stay was significantly shorter in the PC group compared with the T-tube group. Notably, one study found similar postoperative stay lengths in both the emergency and elective groups, whereas another study revealed a shorter stay in the elective group.
Interpretation of the data in the context of other studies
The journey of gallbladder surgery has undergone significant transformation. The roots of this evolution can be traced back to 1882 when Langenbuch performed the first cholecystectomy. However, it wasn’t until 1890 that exploration of the CBD began. The situation took a revolutionary turn in 1987 with the advent of LC by Mouret, announcing a new era for gallbladder procedures. 15
Initially met with skepticism, the feasibility of laparoscopic bile duct exploration was doubted. Yet, subsequent advancements have demonstrated that successful transcystic or supra-duodenal exploration is indeed possible. Technical success has become the norm for the majority of patients, challenging the early reservations. 15
A milestone in the field was the development of a novel laparoscopic technique for CBD exploration, as described by Stoker et al. 16 This technique involved flexible choledochoscopy, stone extraction, and T-tube drainage, successfully implemented on a series of five patients. Such innovative approaches highlight the influence of minimally invasive methods on the management of choledocholithiasis.
Since then, these techniques have been specifically described for the management of elective CBD exploration. However, for emergency cases such as cholangitis, no consensus has been reached, and this approach remains a subject of debate for primary treatment.
Management of AC involves targeting its essential components: biliary infection and obstruction. 17 Antibiotics and biliary drainage are the two basic elements in the therapeutic management of AC. 3
Since the TG18 flowchart for managing AC is quite similar to TG13, it’s now best to manage it based on its severity. 3 In cases of moderate and severe AC, The TG18 recommend early endoscopic or percutaneous transhepatic biliary drainage. 3
Nevertheless, the management of patients with nonsevere AC continues to be a subject of debate. Recent guidelines lack consistent recommendations regarding the optimal approach between LCBDE + LC or the sequence of ERCP/endoscopic biliary sphincterotomy (EST) followed by LC postantibiotic management of AC. 11
For these reasons, we decided to carry out this systematic review, which is, to our knowledge, the first to address the feasibility and safety of laparoscopic treatment in AC.
In the literature, we observed a particular emphasis on ElLCBDE, exemplified by studies such as the meta-analysis performed by Lyu et al. 18 and the systematic review conducted by Marks et al. 4
Sun et al. 17 claim that for nonsevere AC related to stones, early LCBDE emerges as a viable option, since both LCBDE and ERCP have yielded comparable success rates, especially in stone clearance from the CBD. They added that LC following ERCP is challenging due to increased postprocedure complications and a higher likelihood of converting to open surgery due to inflammation and fibrosis around Calot’s triangle. Furthermore, ERCP-induced Oddi sphincter dysfunction can cause lasting harm to the sphincter barrier, obstructing duodenobiliary reflux. 17
Choosing between these methods is intricate due to the treatment’s multidisciplinary nature, availability differences among centers, and surgeon expertise with each technique. 19
Overby et al. 20 think that performing single-stage LCBDE or the combined laparoscopic approach with intraoperative endoscopy demands a specific level of skill, experience, equipment, and time that not all surgeons and medical facilities conducting LC possess uniformly. 20
While LCBDE has been employed to treat CBDS, it hasn’t yet been incorporated into clinical guidelines for AC treatment. 12
Persisting stones stand out as a significant post-LCBDE complication, noted in around 8.5% of cases. However, the integration of choledochoscopy tools has considerably reduced this phenomenon, resulting in a reduced rate to around 2%. 5
In their study on the treatment of cholangitis, Zou et al. found that in contrast to the ERCP + LC approach, the LCBDE + LC procedure offers several benefits. It maintains the integrity of the Oddi sphincter’s structure, reduces the occurrence of complications such as pancreatitis, hemorrhage, and bile leakage, and presents a more cost-effective therapeutic option. As a result, it deserves consideration for wider adoption in clinical practice. 8
Zhu et al.’s study revealed that early or delayed LCBDE is equally safe and effective for managing nonsevere AC related to CBDS. 12 While ERCP/EST might suit severe cases and high-surgery-risk patients, LCBDE seems advantageous for nonsevere cases, enabling simultaneous gallbladder and CBDS treatment. 12 This minimally invasive approach preserves sphincter function and minimizes the need for a secondary delayed LC admission. 12
When comparing the EmLCBDE group with the ElLCBDE group, Alhamdani et al. 13 found that there were no significant differences in terms of mortality, morbidity (including bile leakage), operating time, or hospital stay. Notably, all three conversions to open surgery occurred within the elective group and not in the EmLCBDE group, making a statistically significant difference. 13 In a similar context, Aawsaj et al. 10 approve the utilization of laparoscopic bile duct exploration for both urgent and ElLCBDE.
Alhamdani et al. 13 recommend that the laparoscopic approach should be prioritized whenever feasible for CBD exploration. Their research indicates that there is a notable increase in mortality, composite morbidity, cases of bleeding, the need for additional surgery, and readmissions linked to the initial operation among patients undergoing OCBDE compared with those who undergo laparoscopic procedures. 13
Our opinion stands with Gholipour’s viewpoint, supporting the notion that urgent one-stage LCBDE, while debated, proves to be a secure, feasible, and economically viable approach in treating nonsevere acute gallstone cholangitis. This strategy effectively reduces the necessity for a subsequent delayed surgical intervention following endoscopic decompression. 6
Strengths and limitations
Our systematic review is the first to address the feasibility and safety of laparoscopic treatment in cases of acute mild-to-moderate cholangitis. While the TG strongly recommend ERCP as the first-line treatment for CBD stone-related cholangitis, LCBDE is a promising technique that is worthy of consideration. However, LCBDE is no superior to the TG recommendations for the endoscopic management of successfully removed CBDS.
Our study has encountered some limitations. The majority of the included studies in this review were retrospective observational studies, with only three being prospective studies, of which only one was an RCT. Consequently, establishing a cause-and-effect relationship between the intervention and the study outcome proved to be challenging.
Furthermore, the significant heterogeneity in patient inclusion criteria posed another limitation to our review. Not all studies exclusively focused on cholangitis. Some studies included patients who underwent LCBDE for all indications combined, including uncomplicated CBDS. Meanwhile, others included patients who underwent EmLCBDE without specifying etiologies. This heterogeneity also extended to data reporting, follow-up protocols, and intraoperative techniques. Indeed, the different laparoscopic techniques were not mentioned in all the studies. This could perhaps influence results such as the prevalence of retained stones in the transcystic or choledocotomy (T-tube or PC) groups, knowing that a wide choledocotomy with stone extraction could reduce the number of retained stones compared with the transcystic approach.
Another limiting factor was the lack of conformity in definitions, such as the severity grading of cholangitis and certain outcome definitions, as seen in the study by Llorente et al., 7 where persistently left stones were classified as residual. In addition to that, Jiang et al. 10 defined retained stones at the end of the procedure as residual.
Conclusion
The collective findings of the reviewed studies demonstrate that performing LCBDE via transductal or transcystic routes, along with options for T-tube drainage or PC of the CBD, is both safe and feasible, especially when undertaken by experienced surgeons. Notably, LCBDE showed a lower morbidity rate compared with OCBDE.
The analysis also indicates that there is no statistically significant difference in terms of complications and mortality between EmLCBDE and ElLCBDE procedures. LCBDE emerges as a favorable option, particularly for nonsevere cases, as it allows simultaneous treatment of gallbladder and CBDS. This approach preserves sphincter function and reduces the necessity for a secondary, delayed admission for LC following ERCP.
In summary, the one-stage urgent LCBDE, while subject to debate, proves to be a secure, feasible, and economically viable approach for managing nonsevere acute gallstone cholangitis.
Further well-designed studies are needed to confirm the results of this systematic review and select the ideal approach to treat AC.
Footnotes
Authors’ Contributions
I.B.: Data collection and analysis and writing. M.M.: Data collection and reviewing and editing. Y.K.: Editorial support. G.H.K.: Editorial support. M.B.M.: Editorial support.
Ethical Approval
No ethical approval required as this research project is a systematic review of previous studies.
Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.