
Abstract
Background:
The most common therapy for gallstones is laparoscopic cholecystectomy (LC). How to help young residents avoid bile duct injuries (BDI) during surgery and grasp LC seems to be a paradox.
Methods:
We retrospectively reviewed 145 cases of LC operated by two residents under indocyanine green (ICG)–guided mode or normal LC procedures to illustrate the role of ICG mode in boosting the LC learning curve. The clinic data were analyzed by logistic regression, receiver operator curve tests, Cumulative Sum (CUSUM), and Risk-Adjusted Cumulative Sum (RA-CUSUM) analysis.
Results:
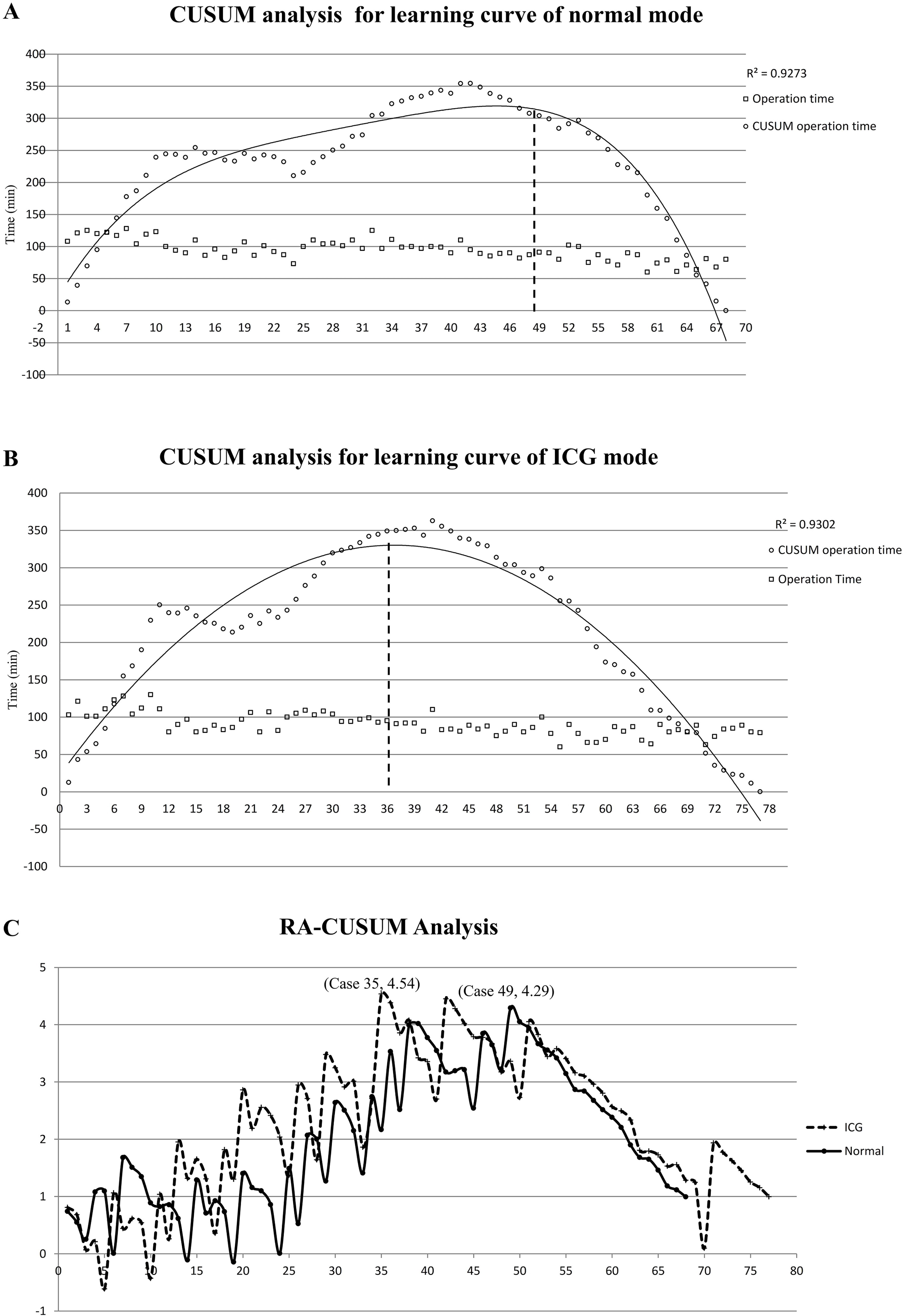
The operation failure rate is similar. However, operation time under ICG mode is shorter than that under normal mode. The peak at the 49th case represented the normal resident’s complete mastery of the surgery, while the peak point of ICG mode appeared at the 36th case in the fitting curve. The most significant cumulative risk (peak point) of operation failure of LC was at the 35th case in ICG LC mode, while it appeared in the 49th in normal LC mode.
Conclusions:
Owing to the advantage of real-time imaging and the stable success rate of cholangiography, ICG-guided LC helps residents shorten the operation time, boost the learning curve, and manage to control the operation failure rate.
Introduction
Gallstone is the most common disease in hepatobiliary surgery, with about 570,000–1,000,000 in the United States every year. 1 The standard treatment for gallstones is cholecystectomy. With the development of the laparoscopic technique, both patients and surgeons widely accept laparoscopic cholecystectomy (LC) because of quick recovery and minimal invasion advantages. Although LC is easy for most surgeons to grasp, several dangerous complications accompany it, especially bile duct injuries (BDIs). The incidence rate of BDIs is about 0.3–0.7%; there are ∼3,000 cases of BDI happening every year.2,3 Once BDI happens, it prolongs hospitalization, increases medical costs, and results in suffering for both surgeons and patients. Making young surgeons or residents avoid this complication and grasp LC safely and rapidly seems a paradox. Indocyanine green (ICG) is a dye that binds with protein in the blood and emits light in near-infrared light, and it is widely used in fundus angiography. ICG is almost entirely metabolized by the liver and excreted through bile, so it is a good and safe dye for cholangiography. Here, we report that ICG-guided LC can boost residents’ learning curves.
Methods and Materials
Participants
From September 2019 to August 2020, a series of 177 consecutive LC operations were performed by two Grade III residents. The principle of informed consent was applied and endorsed by the Ethics Committee of the hospital. The inclusive criteria contained the ultrasonic diagnosis of gallstone or gallbladder polyps (diameter over 1 cm) before surgery. The exclusive criterion contained preoperative percutaneous transhepatic gallbladder drainage (PTGD) or endoscopic sphincterotomy (EST), former abdominal surgery history, positive for an iodine allergy test before surgery, suspect of gall bladder cancer or frozen section biopsy in surgery, and combined with other procedures such as drainage of a hepatic cyst or other biopsies. The consort diagram of patients is shown in Figure 1.
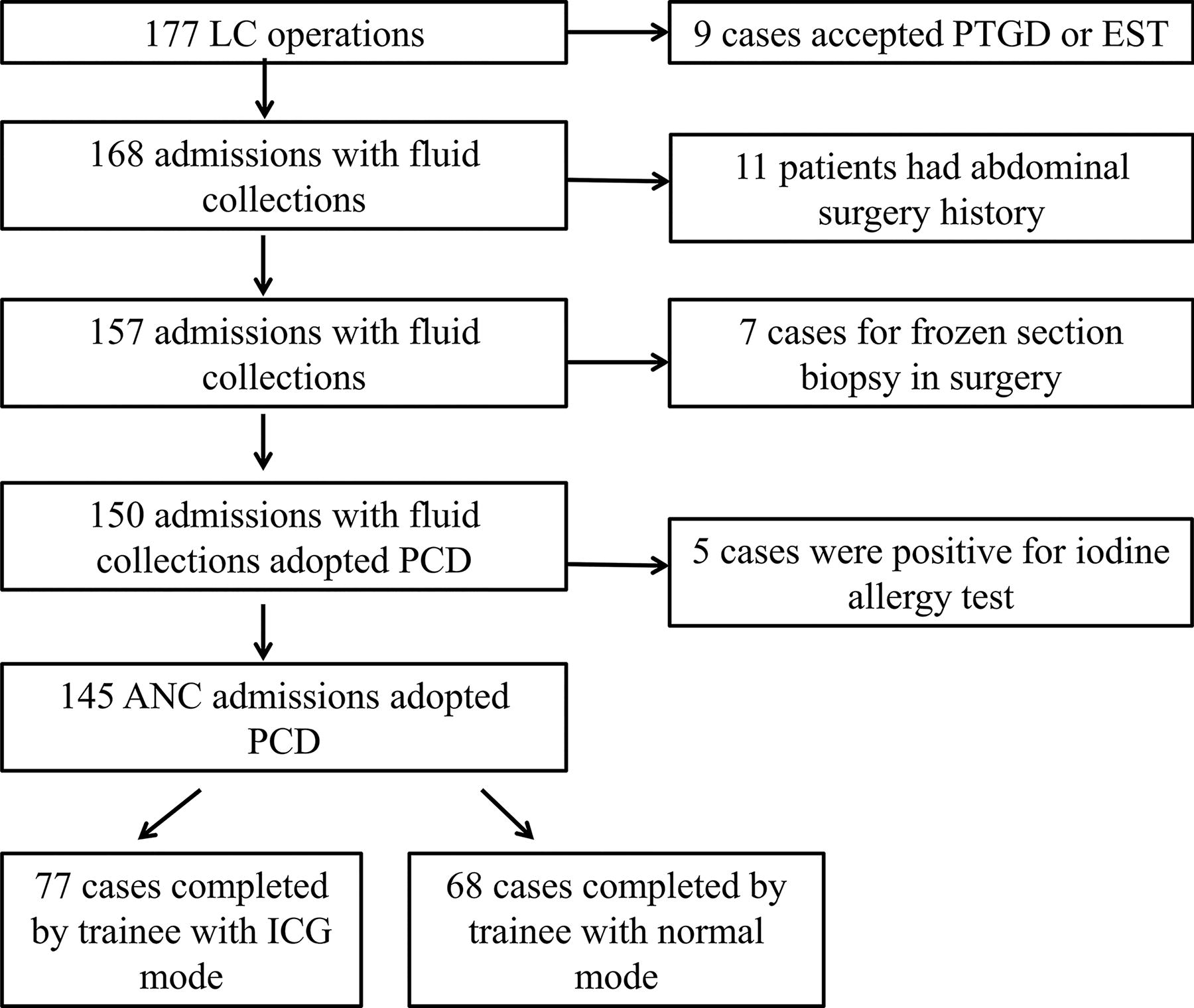
The consort diagram of case recruitment.
Two Grade III residents, both with master’s degrees, who were in the standardized resident training of China participated in this study. These two residents had similar previous surgical assistant experience of LC for 6 months. An experienced attending surgeon acted as the endoscope holder for the two residents that performed the procedure. Typically, the attending surgeon only holds the endoscope, occasionally giving verbal reminders, but does not help with the entire procedure. Sometimes, owing to local anatomical and inflammatory factors, the resident does not have good exposure to the surgical field of view, uncontrollable bleeding occurs or major structural misidentification occurs, then the attending surgeon will perform subsequent procedures on the resident’s behalf. For the resident, failure to complete the entire operation is naturally considered a failure, but all operations are completed by the attending surgeon.
Operation procedures
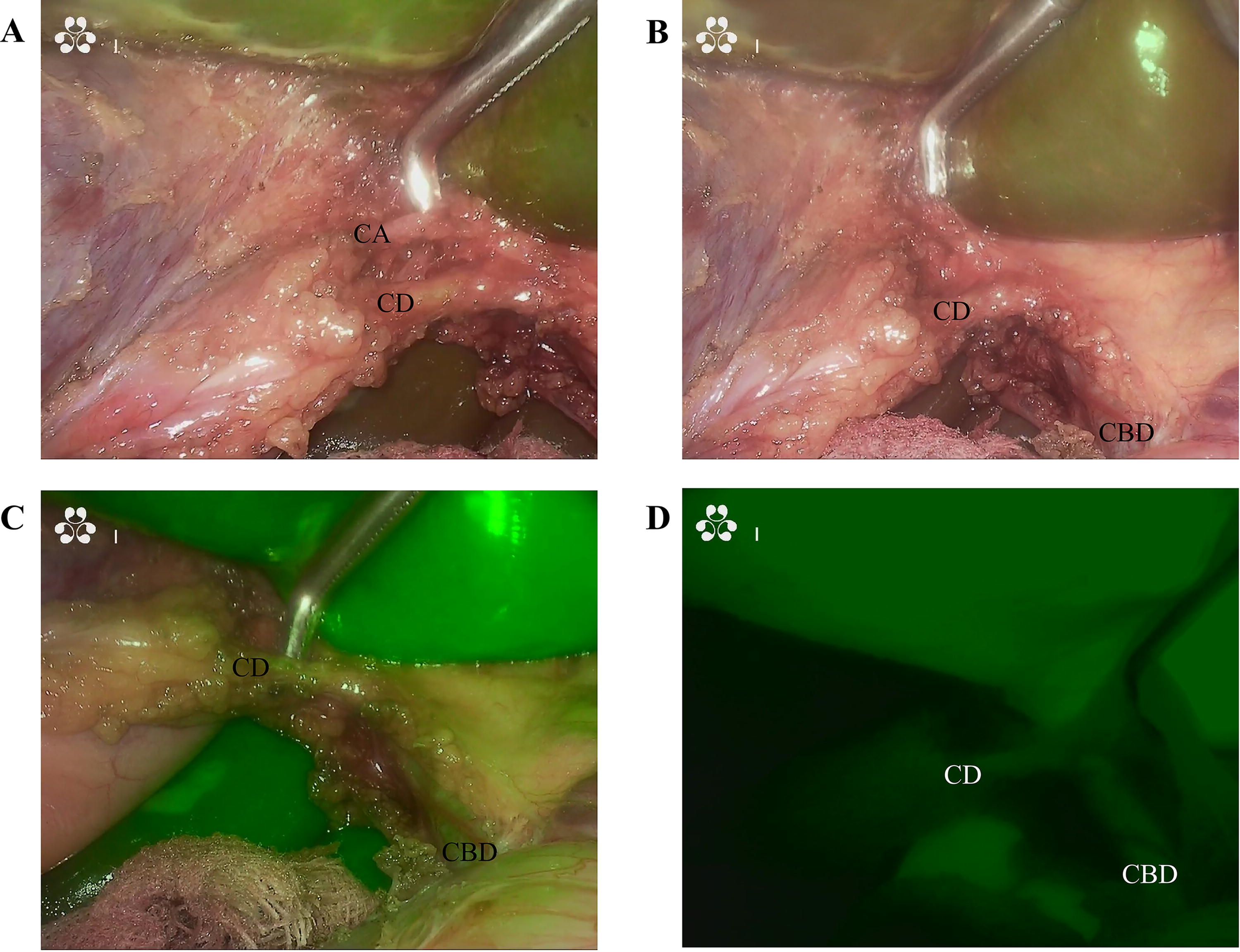
ICG (25 mg) was diluted in 10 mL sterile water and was injected intravenously after the patients were anesthetized. Fluorescence laparoscopic imaging system (OptoMedic, Fine P3, China) was used for intraoperative conventional imaging mode and ICG mode. The ICG-guided mode is shown in Figure 2A–D. The normal procedure of LC was performed via the resident’s preferred method.
Data collection and analysis
The primary endpoint was operative time for the CUSUM analysis (
Statistical analysis
Statistical analysis was performed by Excel 2010 and GraphPad Prism 5. Continuous data were presented as the mean ± standard deviation (SD) and evaluated using Fisher’s exact t-test. Categorical data were described with frequency counts and assessed using the χ2 test. Two-tailed P < .05 was considered to be statistically significant. Logistic regression was used to assess the risk factors for operation failure.
Results
Two residents completed a total of 177 cases of LC. In total, 32 cases were excluded: 9 cases accepted PTGD or EST, 11 cases with abdominal surgery history, 7 cases accepted frozen section biopsy during surgery, and 5 cases were positive for an iodine allergy test. The resident using the ICG-guided mode completed 77 cases of LC (53.10, 77/145), whereas the other resident completed 68 cases (46.90, 68/145) via normal mode LC. The characteristics of patients in the two groups are shown in Table 1. Under the ICG mode, the operation failure rate is 15.58% (12/77), whereas under normal surgery conditions, the rate was 17.65% (12/68). There is no significance between the two groups (P = .824, Table 1). When operation time was compared in two groups, ICG mode (90.10 ± 16.77 minutes) presented a shorter operation time than normal mode (95.22 ± 19.31 minutes) (Fig. 3A, P = .046).

Baseline Characteristics of All Patients in Each Group
ALP, alkaline phosphatase; GGT, Glutamyl transferase.
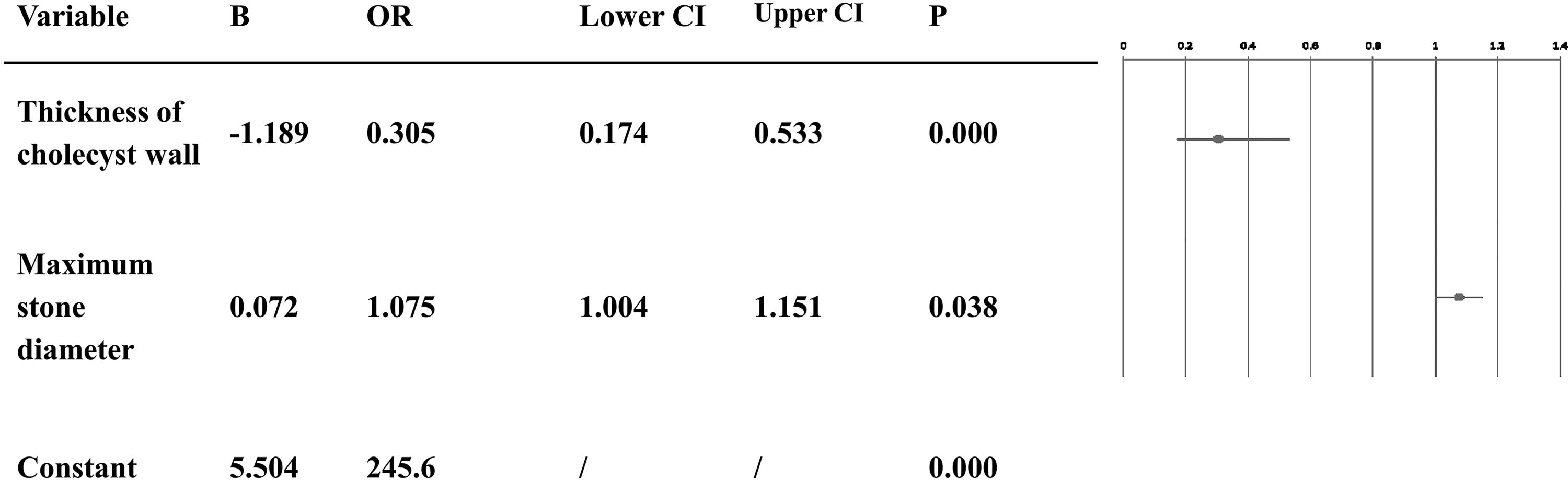
According to the CUSUM analysis, the peak point at the 49th case (Fig. 4A) represented full mastery of the surgery by the normal resident, whereas the peak point of ICG mode (Fig. 4B) appeared at the 36th case in the fitting curve, which was much earlier than in normal mode. Univariable logistic regression analysis analyzed the risk factors for operation failure in the next step. Three findings were discovered here. First, the maximum stone diameter (B = .077, P = .035, Fig. 5) and thickness of cholecystic wall (B = −1.267, P = .000, Fig. 5) were independent risk factors. Second, using multivariable logistic regression and the area under the receiver operating characteristic curve (ROC) analysis, the thickness of the cholecystic wall presented discrimination with an area under ROC of 0.7425 (P = .000, 95% CI: .593–0.856), and the thickness of the cholecystic wall of 4.5 mm gave a better indication of operation failure (Fig. 3B). Third, the formula of the expected operation failure rate Pi (

Univariable logistic regression analysis of operation failure.
Multivariable logistic regression analysis of operation failure.
Discussion
LC is an easy but risky surgery because of the incidence of BDIs. Although most BDIs are related to anatomical misidentification, 4 how to eliminate this misidentification is still a confusing question. At the same time, multiple strategies are adopted to improve the safety of this surgery to prevent the patients from the complication of BDI. Nevertheless, there are still no perfect methods. In 1995, Strasberg 5 gave a fundamental principle of critical view of safety (CVS) in LC. Based on the CVS principle, many other strategies are emerging, such as retrograde cholecystectomy (fundus first), 6 landmark of Rouvière’s sulcus,7,8 and segment IV approach. 9 Among all these strategies, the CVS principle is globally accepted by surgeons and has proved to be the most efficient tool. It contains three key points: first, the fat and fibrous tissue that cover the Calot triangle must be cleared; second, the lowest part of the gallbladder must be separated from the liver bed; finally, and most importantly, two structures (cystic duct and cystic artery), and only two, should be seen entering the gallbladder. 10 Although the CVS principle is recommended by several guidelines1,11–13 as well as supported by several large sample trials,14,15 there is no Level I evidence that CVS reduces BDI rates because of the overwhelming cost of performing a surgical trial. 10 Besides, the common bile duct (CBD) might still be mistaken as a cystic duct in case of severe inflammation. Meanwhile, some accidental injury might occur during the dissection before the CVS was achieved, or a sudden trauma happens during the over-chasing for CVS. However, CVS is an imperfection but closest to perfection strategy. To solve the difficulty of achievement of CVS in severe inflammation conditions, the fundus-first (top-down) technique versus subtotal cholecystectomy (STC) is recommended by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). 1
Fundus-first (top-down) technique versus STC means dissection starts with the fundus and directs to the Calot triangle, which is also described as “dome-down,” “fundus-down,” or “retrograde cholecystectomy.” When the dissection comes to the inseparable Calot triangle, two types of subtotal cholecystectomy could be adopted: full-thickness cholecyst remnant left on the liver bed or partial cholecyst remnant (Hartman’s pouch and cystic duct left).16,17 This approach is a choice of last resort. The persistence of a cholecyst remnant may result in bile leaking, residual stones, or new stone formation and expose the patient to the risk of recurrent gallstones with a possibly challenging reoperative cholecystectomy. 18
The Landmark of Rouvière’s sulcus and segment IV approach is a strategy with the help of anatomy markers of the liver to realize the aim of CVS. Rouvière’s sulcus was first described by Henri Rouvière, as a 2- to 5-cm sulcus, running to the right of the liver hilum anterior to the caudate process and usually containing the right portal triad or its branches. The sulcus was found to indicate the plane of the CBD accurately LC. Hugh7,8 indicates that retracting the cholecystic neck to the cephalic and midline could expose the posterior aspect of the Calot triangle, and the sulcus indicates the plane of the CBD reliably; dissection may be started safely in the triangle bounded by the liver surface, the cholecystic neck, and the plane of the sulcus. Although Rouvière’s sulcus plane is a safe marker for dissection of the posterior aspect of the Calot triangle, the absence rate of this marker is about 10%–17%, as reported.19,20 Fujioka 9 indicates that the segment IV approach’s diagonal line (D-line) is supplementary for CVS and Rouvière’s sulcus approach, especially for anomalous bile duct. D-line is an imaginary line that lies on the right border of the hilar plate, while the cystic plate can be securely isolated along the D-line without any misidentification. In a Japanese guideline (Tokyo Guidelines 2018), 13 it is recommended that a safe procedure is between the roof of Rouvière’s sulcus and the base of segment IV to perform all surgical procedures to achieve CVS. In other words, Rouvière’s sulcus gives a safe border of the posterior plate, while the base of segment IV gives a safe border of the anterior plane of the Calot triangle. It is theoretically safe above the imaginary line connecting these two landmarks. Although the segment IV approach is an efficient supplementary for CVS, especially under the circumstances of absence of Rouvière’s sulcus or anomalous bile duct; however, in cases where the margin of the cholecyst is unrecognizable because of inflammatory adhesion, the segment IV approach is not applicable, and the dissection of cholecyst from the lateral side has a risk of injuring the anterior Glisson sheath. 21 Meanwhile, the segment IV approach is an imaginary line that may not be suitable for an inexperienced surgeon to deep understanding. This wisdom and the easy-to-apply classical approach are integrated by an experienced surgeon. However, these may be challenging for inexperienced surgeons or residents.
Can we find a better strategy for that green-hand to safely and rapidly master the CVS principle? ICG fluorescence imaging, which is widely used in liver and biliary tract surgeries,22,23 was also first used for cholecystectomy by Mitsuhashi 24 in 2008, and for laparoscopic cholecystectomy by Ishizawa 25 in 2009. Herein, through the analysis of the CUSUM and RA-CUSUM model in the learning curve of LC, it is demonstrated that ICG-guided LC mode can shorten the total operation time, decrease the risk of operation failure rate, and eventually boost the learning curve of LC. These effects may rely on three reasons. First, the ICG-guided mode could give a direct visualized identification of the bile duct in almost every step during the LC surgery, which might be a kind of true CVS. Esposito 26 reports that the ICG-guided mode aided in clearly visualizing the biliary structures, including the cystic duct (CD), the CBD, and especially the CD-CBD junction, despite the presence of plenty adipose tissue, inflammation, and dense tissue adhesions. Other visualized strategies like intraoperative cholangiography (IOC) are an option but with limitations that IOC is a non-real-time image and has radiation exposure, higher costs, and requirement of performing an incision resulting in an increased incidence of BDIs. 27 Besides, IOC is recommended under the circumstance that surgeons with appropriate experience and training 1 may not be the first choice for green hands.
Second, compared with other landmark approaches, the ICG-guided mode presents a stable success rate of cholangiography. ICG can only be secreted by hepatic through bile, which facilitates imaging of the extrahepatic biliary tract. Theoretically, the success rate of the ICG-guided mode can be 100%, except for some patients with allergy. Several clinical trials report that the cholangiography success rate during surgery is over 95%.28–32 Third, the ICG-guided mode can shorten the operation time and boost the residents’ learning curve of LC. In a previous study, compared with the IOC time of 11.8 ± 5.3 minutes, the ICG mode takes only 1.9 ± 1.7 minutes to complete the imaging process. 32 Regarding the total operation time, Broderick 33 reports that a significantly short operative time for ICG and non-ICG groups was 75.57 and 104.9 minutes, respectively. In this study, it is demonstrated that the total operation time of the ICG-guided LC mode is 90.10 minutes, which is shorter than that in the normal mode of 95.22 minutes. Most importantly, it is also proved that the surgeon could master the LC technique and manage the failure risk earlier than that under normal mode, which might be helpful for the green-hand surgeons to get this surgery safer and quicker.
Limitations
Although the ICG injection is safe and efficient, ICG does carry a small risk of allergy after injection. Hence, it should be carefully administrated with an iodine allergy test. Only two residents were compared in this study, and it is difficult to eliminate personal bias. A large sample clinic trial is needed to provide solid evidence.
Footnotes
Authors’ Contributions
H.L. and T.W. were the surgeons and contributed to article editing and statistical analyses; L.X. and P.L. were the following-up physicians; C.W. and S.Z. contributed to initial article drafting.
Disclosure Statement
All authors declare that they have no conflicts of interest or financial ties to disclose. The principle of informed consent was applied and endorsed by the Ethics Committee of the hospital. N/A for the registry of the study. N/A for animal studies.
Funding Information
This work received grants by the NSFC (No. 81502696), Technology Plan Program of Sichuan Province (No. 2018JY0185), Program of General Hospital of Western Theater (No.2021-XZYG-C33), Teaching Reform Project of Chengdu Medical College (No.JG202089), and Science & Technology Department of Sichuan Provence International Cooperation Program (NO.2019YFH0056, 2020YFSY0022, and 22ZDYF1076).