
Abstract
Background:
The safety and efficacy of enhanced recovery after surgery (ERAS) following elective gastrectomy for gastric cancer in patients >80 years of age are not well described. The aim of this study was to explore whether an ERAS protocol following gastrectomy in this age group can be safely implemented and reduce postoperative length of stay.
Methods:
A retrospective, single-center analysis was performed. All patients >80 years of age with gastric cancer undergoing elective subtotal and total gastrectomy between January 2010 and December 2021 were identified. With the implementation of an ERAS protocol in January 2016, patients treated beforehand were allocated to Group A (pre-ERAS) and Group B (ERAS). The length of stay, incidence of postoperative complications and representation/readmission to the hospital were compared between the groups.
Results:
Of the 221 patients identified, 56 met the inclusion criteria with 22 patients (39.3%) allocated to Group A and 34 patients (60.7%) to Group B. There were no differences with regard to the type of resection and surgical approach. Length of stay was shorter in Group B (5 days, range 2–27 versus 10 days, 3–109, P = .040). A trend toward more discharges by postoperative day 3 was noted among patients in Group B (7/34, 20.6% versus 2/22, 9.1%, P = .253). There were no differences in the incidence of postoperative complications or readmission hospital between the groups.
Conclusion:
Among patients >80 years of age, ERAS following gastrectomy for cancer is associated with a reduced length of stay and can be safely implemented.
Introduction
Gastric cancer is the fifth most commonly diagnosed cancer in the world and the third most frequent cause of cancer-related death. 1 In locally advanced disease, the best chance of cure is afforded by multimodal treatment, including systemic chemotherapy and surgical resection. However, surgical resection represents a significant physiological insult and is associated with an 11–45% incidence of postoperative complications.2–4 Furthermore, data suggest that age ≥70 is independently associated with a heightened risk of postoperative complications. 5
With a view to reducing the physiological stress of surgery, enhanced recovery after surgery (ERAS) programs have become increasingly popular. These programs are multimodal and interdisciplinary perioperative packages of care that are designed to accelerate recovery postoperatively by reducing operative stress and promoting a swift return to normal function. Thus, the goal of an ERAS protocol is to improve surgical outcomes by accelerating rehabilitation and optimizing perioperative management. 6 Particularly, within the setting of surgery for gastric cancer, these protocols have focused on preoperative patient education, judicious intraoperative fluid management, early postoperative enteral nutrition and mobilization, multimodal analgesia while avoiding nasogastric drainage and abdominal drains.7–9
The net results of ERAS protocols following gastrectomy are to decrease the postoperative length of stay and reduce the overall cost of admission. 10 Although data varies, there is evidence that suggests ERAS is associated with a reduction in the incidence of postoperative complications, such as ileus, pneumonia, intra-abdominal infections, reoperation, death, and potentially associated with improved long-term survival.11,12 Despite these benefits, there seem to be some patients following gastrectomy for whom the benefits of ERAS are attenuated. For instance, data suggest that elderly patients and those with multiple comorbidities still seem to suffer from an increased incidence of postoperative complications, longer hospital stays and higher readmission rates despite being treated with ERAS after gastrectomy. 13 Furthermore, old age specifically has been found to be associated with failure to comply with important elements of ERAS protocols, such as early enteral nutrition and restrictive intravenous fluid intake.14–17 As such, it has been suggested that a modified protocol may be beneficial for elderly patients undergoing abdominal surgery. 18
However, much of the literature exploring the efficacy and safety of ERAS following gastrectomy define elderly as those ≥65 years. 8 Furthermore, many of the studies in the academic literature compare older with younger patients. 7 Therefore, considering the noted increase in surgical morbidity in octo- and nonagenarians, the true risks and benefits of ERAS implementation in this specific age group of patients are not well described. We hypothesize that the implementation of an ERAS protocol following gastrectomy for gastric cancer will be safe and feasible in this specific group of patients. The aim of this study is to explore whether the implementation of an ERAS protocol following gastrectomy in octo- and nonagenarians is associated with a decrease in the incidence of postoperative complications and a reduction in the length of stay.
Materials and Methods
Study design and patient population
Approval for this study was granted from the Institutional Ethics Committee. This retrospective single-center cohort study was performed in a regional upper gastrointestinal cancer program centered at the Thoracic and Upper Gastrointestinal Surgery Department of the Montreal General Hospital, a high-volume university-affiliated tertiary referral center in Montreal, Canada. Between January 2010 and December 2021, all patients who underwent elective gastrectomy for gastric cancer were identified through a search of a comprehensive and prospectively maintained departmental electronic database. Once these patients were identified, they were verified according to the following inclusion criteria: Patients must have been 80 years or older at the time of surgery; have undergone elective total, subtotal, or proximal gastrectomy for a proven diagnosis of gastric cancer; have been diagnosed preoperatively with locally advanced disease (Tany, Nany, M-); and treated with curative intent. Surgery may have been performed through a laparoscopic or open approach and the use of neoadjuvant therapy did not preclude inclusion. Patients who underwent urgent, or semiurgent gastrectomy for bleeding, obstruction, or perforation were excluded. A flow chart of patient inclusion in the study is displayed in Figure 1.

A flow chart of patient inclusion in the study.
Definition of ERAS protocol and allocation to study groups
During the study dates, a departmental ERAS program was implemented in January 2016 for patients who underwent either total or subtotal gastrectomy for gastric cancer. The core elements of this program are described in Table 1. Patients who underwent surgery before the implementation of the ERAS protocol were allocated to Group A, while those treated after implantation were allocated to Group B. There were no changes made to the ERAS protocol based on the patient’s age, physiological status, or the type of procedure performed other than an epidural being used for planned open gastrectomy. Furthermore, despite the protocol being constantly reviewed as part of a quality improvement process and changes made to reflect emerging evidence, there were no substantive changes made to the protocol during the study period.
ERAS Protocol Elements for Patients Undergoing Elective Gastrectomy for Gastric Cancer
Outcome measures, variables, and data extraction
The primary aim of this study was to explore whether the implementation of an ERAS protocol following gastrectomy in octo- and nonagenarians was associated with a decrease in the incidence of postoperative length of stay. The secondary outcome was to ascertain whether the implementation of an ERAS protocol in this specific group of patients affected other postoperative metrics, including the incidence of postoperative complications, representation to the department of emergency medicine or readmission to hospital, and 90-day mortality.
Once patients had been verified according to the above inclusion criteria, demographic and clinicopathological variables were extracted from the departmental database supplemented by electronic and paper medical records. Major postoperative complications were defined as Clavien–Dindo grade ≥3 occurring within 30 days of surgery. The number of patients for whom nasogastric/nasojejunal decompression was used at the end of surgery was noted as was the number of patients that had their urinary Foley catheter removed on PoD 1. Whether oral intake was started on postoperative day 1 was also recorded.
Statistical analyses
The data were recorded in an ExcelTM spreadsheet and processed using SPSSTM statistical software (version 27, SPSS Inc, Chicago, Illinois, USA). The data are presented as median or frequency with range or percentage in parentheses. Univariate analyses were performed using χ2 or Fisher’s exact test for categorical data, while continuous variables were compared using the Mann–Whitney U test. For all calculations, a P value of <.05 was considered statistically significant.
Results
As shown in Figure 1, 221 patients underwent gastrectomy during the study period. Following application of the inclusion/exclusion criteria, there were 56 (25.3%) patients identified of whom 22/56 (39.3%) were allocated to Group A and 34/56 (60.7%) to Group B. As is shown in Table 2, while there were more female patients allocated to Group B (15/34, 44.1% versus 3/22, 13.6%, P = .016) there were no other differences in the clinicopathological data when comparing between the groups.
Demographic and Clinicopathological Data
Furthermore, as shown in Table 3, there were also no differences in terms of operative metrics, including the type of resection performed, surgical approach, length of surgery, and intraoperative blood loss. With regard to perioperative outcomes, the incidence of major postoperative complications was similar between the groups, however, the overall length of stay was shorter among patients allocated to Group B (5 days, range 2–27 versus 10 days, range 3–109, P = .040). There were no differences noted in the utilization of nasogastric tubes or peritoneal drains. Although not significant, twice as many patients treated with an ERAS protocol were discharged on PoD 3 (7/34, 20.6% versus 2/22, 9.1%, P = .253). There was also no difference noted in the incidence of readmission to hospital, reattendance to the department of emergency medicine, or 90-day mortality.
Univariate Analysis of Perioperative Data Stratified by ERAS Use
A comparison of length of stay stratified by the group allocation is shown in Figure 2. As seen, there is a steady decline in the percentage of patients for each length of stay interval in Group B while for Group A, over 60% of patients had an admission that lasted more than 9 days.
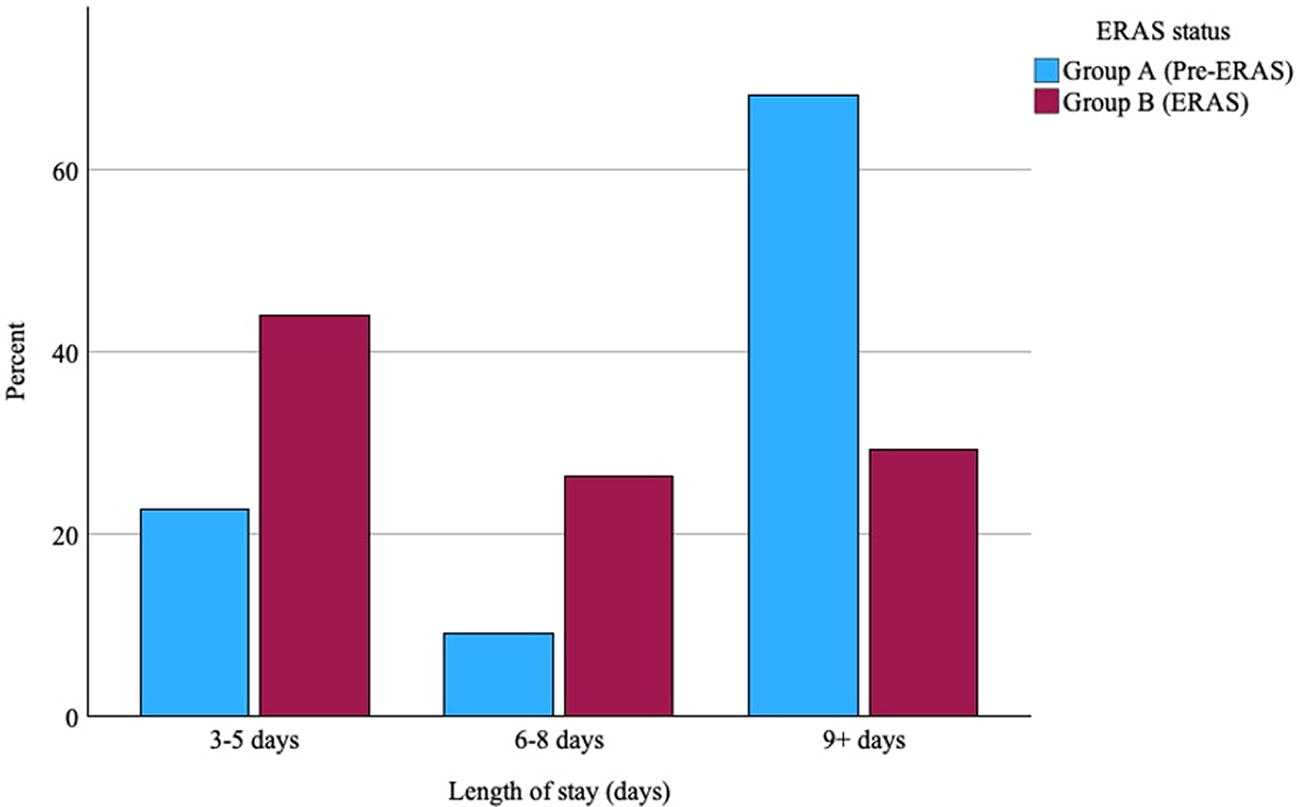
A diagram comparing length of stay between Groups A and B.
Discussion
In this study, we explored the efficacy and safety of an ERAS protocol in patients >80 years of age who underwent gastrectomy for gastric cancer. We found that the length of stay was significantly shorter among patients treated with ERAS, with no appreciable change in patient safety in terms of postoperative complications and, despite a shorter admission, no association with an increase in the incidence of representation or readmission to hospital.
The association between ERAS programs and reduced length of stay following major abdominal and foregut surgery have been well described in the literature. 19 Specifically, within the setting of benign foregut surgery, ERAS has been shown to reduce complications and engender shorter lengths of stay by challenging traditional methods of treating the postoperative patient particularly by encouraging early ambulation and oral intake. 20 Among older patients, while data vary, it seems that ERAS protocols following elective abdominal surgery can reduce postoperative length of stay in patients >70 years of age.21,22 Using a lower cutoff of 65 years of age, Cao found ERAS implantation following gastrectomy for cancer was associated with a reduction in the length of stay from 13 to 11 days (interquartile range 8–20 versus 7–11, P = <.001). 8 Similar results were described in a recently published Chinese study in patients >70 years of age. 7 The data presented in this study are the first in the academic literature to support a shortened length of stay to be associated with ERAS in patients undergoing gastrectomy within this specific age group.
Beyond shortening the length of stay, the safety of ERAS has also been well documented. For instance, a recent meta-analysis found that ERAS was associated with a reduction in postoperative complications following noncolorectal abdominal surgery (odds ratio, 0.70; 95% confidence interval, 0.56–0.86, P = .001). 19 However, following gastrectomy, the effect that ERAS has had on the incidence of postoperative complication seems to be attenuated. Specifically, among elderly patients following gastrectomy, a prospective study of patients >70 years of age found that ERAS did not reduce the incidence of complications (18% versus 16%, P = .14). 7 In comparison, a randomized trial among patients >65 years of age undergoing total gastrectomy found that the incidence of Clavien–Dindo grade ≥3 complications was lower among those treated with ERAS. 8
The variation in these outcomes may be explained by the greater number of comorbidities and frailty among older patients negating the positive benefit that ERAS may have on postoperative complications and length of stay following abdominal surgery. 23 This is despite data that suggest compliance toward ERAS protocols is high even among elderly patients. 24 Nevertheless, the findings here suggest that ERAS can be safely implemented in patients >80 years of age following radical gastrectomy for cancer without an appreciable increase in the incidence of postoperative complications. Such a finding is pertinent as old age, frailty, and comorbid status have all been associated with failure of ERAS and as such a higher incidence of postoperative complications.15,18
Representation and readmission to hospital is another important metric by which the safety of ERAS can be judged. For instance, in the randomized study by Bu et al., patients 75–89 years of age who underwent open gastrectomy were randomly assigned to conventional care or fast track recovery programs. 25 Elderly patients treated with ERAS were found to suffer from more nausea and vomiting, abdominal distention, and ileus. Furthermore, a readmission rate of 19% was described, compared with 5% among similarly aged patients treated conventionally. Of note, similar to data regarding the incidence of complications, when using a lower age cutoff, this trend does not seem to exist. 8 While older age and greater comorbid status have been associated with readmission following gastric cancer surgery, such a trend was not found in the cohort presented in this study. 26 We suggest that the reason this was the case following the implementation of an ERAS protocol at out institution was because of the early engagement by our department with a specialist nurse coordinator. While this relationship is not supported by specific data, such an approach is nevertheless strongly supported in recent international consensus guidelines concerning ERAS following emergency laparotomy. 27
There are several limitations to this study. The retrospective single-center nature limits the quality of the data collection and generalizability of the results to other institutions and surgery types. Furthermore, the small cohort means that subgroup analysis of surgery type is not possible. In addition, we were unable to account for changes in ERAS compliance over time, which may ultimately affect the trends described above. We also assumed the ERAS protocol was standardized and although it did not undergo specific changes, subtle paramedical changes beyond the protocol, such as nursing and physiotherapy-led interventions, may not be accounted for.
In conclusion, we have shown that ERAS can be safely implemented in patients >80 years of age following radical gastrectomy for cancer. Such an approach can be done safely without increasing postoperative complications and representation or readmission to hospital.
Footnotes
Authors’ Contributions
J.T.: conceptualization, methodology, formal analysis, and writing—original draft; G.S.: conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing; A.K.: writing—review and editing; M.D.: writing—review and editing; R.S.: writing—review and editing; N.A.: writing—review and editing; A.M.: writing—review and editing; S.N.: writing—review and editing; J.S.: writing—review and editing; J.C.L.: writing—review and editing; L.F.: writing—review and editing; C.M.: conceptualization, methodology, writing—review and editing, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.