
Abstract
Objective:
Our aim was to evaluate patient-related factors and compare the techniques used for surgical specimen removal [trocar extension (TE) and Pfannenstiel incision (PF)] in terms of incisional hernia (IH) occurrence in patients undergoing robot-assisted laparoscopic radical prostatectomy (RALRP).
Materials and Methods:
The records of 219 patients who underwent RALRP in our clinic between November 2017 and March 2021 were analyzed retrospectively. Postoperative complication data and functional (continence and potency status) and oncological outcomes were recorded. Hernia type, location, and treatments applied were also noted.
Results:
After exclusion, complete data were available on 192 patients undergoing RALRP between the specified dates. The TE technique for removing the surgical specimen was performed in 135 patients, and the lower abdominal transverse incision technique (PF) in 57 patients. Preoperative patient- and tumor-related characteristics (age, body mass index [BMI], American Society of Anesthesiologists (ASA) score, T stage, and prostate size) were similar in both surgical groups. IH was detected in 16 patients (14 in the TE group and 2 in the PF group) (P = .156). Thirteen patients underwent surgery for IH, and three were followed up clinically.
Conclusion:
In our study, no statistically significant demographic or surgical technique-related factors were found to explain the occurrence of IH in patients who underwent RALRP for prostate cancer. It was observed that IH occurred more frequently in the cases where the surgical specimen was removed with the TE technique compared with the PF incision, but this result was not statistically significant. There was also no statistically significant difference between these two groups regarding oncological and functional outcomes in the early postoperative period.
Introductıon
Prostate cancer is the second most frequent cancer diagnosis in men and the fifth leading cause of death worldwide. 1 Prostate-specific antigen (PSA) screening and novel diagnostic tools have made it possible to identify cancer patients in asymptomatic, localized stages, therefore there has been a significant increase in the detected incidence of prostate cancer over the past few decades. 1 Despite high morbidity rates, radical prostatectomy remains the gold standard treatment modality for localized prostate cancer. 2
To improve complication-free rates and surgical outcomes, many urologists seek new options, and minimally invasive surgical methods have come to the fore as alternative methods to open surgery in recent decades. 3 As developments in robotic surgery yield satisfactory results, robot-assisted radical prostatectomy has become a trending and widely preferred technique in minimally invasive urology. 4 Nevertheless, as with all new solutions, developments in this area have also brought about some problems. Each minimally invasive surgical technique has its own risk and spectrum of complications. One of these complications is extraction-site incisional hernia (IH), which may occur after robot-assisted laparoscopic radical prostatectomy (RALRP). However, there is a gap in the current literature concerning factors that may affect the development of IH after RALRP. Therefore, this study aimed to determine the predictors of IH development after RALRP and compare different organ removal sites regarding IH occurrence.
Materials and Methods
The data of 219 patients who underwent RALRP in our clinic between 2017 and 2022 were reviewed retrospectively. Patients without IH were included in Group 1, and those with IH in Group 2. Informed consent was obtained from the patients before the operation. Ethics committee approval was obtained (number: 404-971).
Patients with a follow-up period of more than 2 years were included in the study. Cases in which robotic surgery was converted to open surgery owing to various reasons and patients who were found to have an umbilical hernia in the preoperative evaluation were excluded from the study.
The Briganti score was calculated for all patients preoperatively. Patients who underwent preoperative magnetic resonance imaging (MRI) were evaluated using the 2018 Briganti nomogram, and those without MRI images were assessed using the 2012 Briganti nomogram. Prostate-specific membrane antigen positron emission tomography (PSMA PET) imaging was preoperatively undertaken in all patients with an International Society of Urological Pathology (ISUP) grade of 2 or higher.
The patients’ age, BMI, the ASA score, the Charlson Comorbidity Index, ISUP grade, previous abdominal surgery, prostate size, and diabetes history were noted. Intraoperative and postoperative data, including operative time, surgical margin status, estimated blood loss, intraoperative and postoperative complications, and the postoperative values of haematocrit, serum creatinine, and estimated glomerular filtration rate were also obtained.
Surgical techniques
Two senior surgeons (B.O. and C.D.) with experience in robotic surgery techniques performed the operations with the transperitoneal approach. In all operations, four 8-mm robotic reusable trocars (Intuitive Surgical) and one 10-mm and one 5-mm assistant trocars (Covidien Surgical Devices) were used. Pelvic lymph node dissection was also performed in all patients with a 2018 Briganti nomogram of 7% or greater and those with a 2012 Briganti nomogram of 5% or greater. At the last stage of surgery, prostate, periprostatic fatty tissue, seminal vesicle, and lymph node dissection specimens were placed in laparoscopic retrieval bags (EndoCatch, Covidien Surgical Devices).
Polyglactin 1/0 sutures were used with the small bites technique to close the fascia of the incision through which the specimen was removed. The fascia at the trocar and the 10-mm assistant port sites entered with the Hasson method were also sutured. No fascia suture was placed for the 8-mm trocars.
Postoperative follow-up
The patients were followed up at 3-month intervals for up to 2 years, followed by annual lifelong outpatient clinic controls. Patients who did not attend their follow-up were called or sent an e-mail. Routine imaging studies were not performed. Patients whose hernia was detected on physical examination were referred to the general surgery clinic for treatment recommendations, even if they had no complaints.
The serum PSA values were recorded at each follow-up visit and the patients were asked if they had developed any new problems since their last visit. Wound healing was confirmed by clinical examination. Erectile function and continence status were assessed. Patients with complaints of weak urine flow were evaluated using uroflowmetry and those who were suspected of having urethral stricture or bladder neck contracture were evaluated using retrograde urethrography and flexible ureteroscopy.
Statistical analysis
The statistical analysis of all data was performed using the SPSS Statistics (Version 20.0, IBM Corp) package program. The suitability of the quantitative data to the normal distribution was evaluated using the Kolmogorov–Smirnov normality test. The independent-sample t-test was used for the comparison of normally distributed numerical data. The Mann–Whitney U test was used to compare the data that did not fit the normal distribution. χ2 values and Fisher’s exact test were used in the analysis of categorical variables. The statistical significance limit of all evaluations was accepted as P < .05.
Results
Between 2017 and 2022, RALRP was performed on 219 patients, of whom 27 were excluded owing to a lack of regular follow-up or missing follow-up data (n = 20), mortality within the first year after surgery (n = 5), and conversion to open surgery for any reason (n = 2). As a result, the sample consisted of 192 patients. The patients were divided into two groups according to whether they developed IH: Group 1 included 176 patients without IH (91.6%) and Group 2 included 16 patients with IH (8.4%) (Fig. 1). See supplementary data for detailed clinical characteristics of all16 patients in Group 2 (Supplementary Data S1).
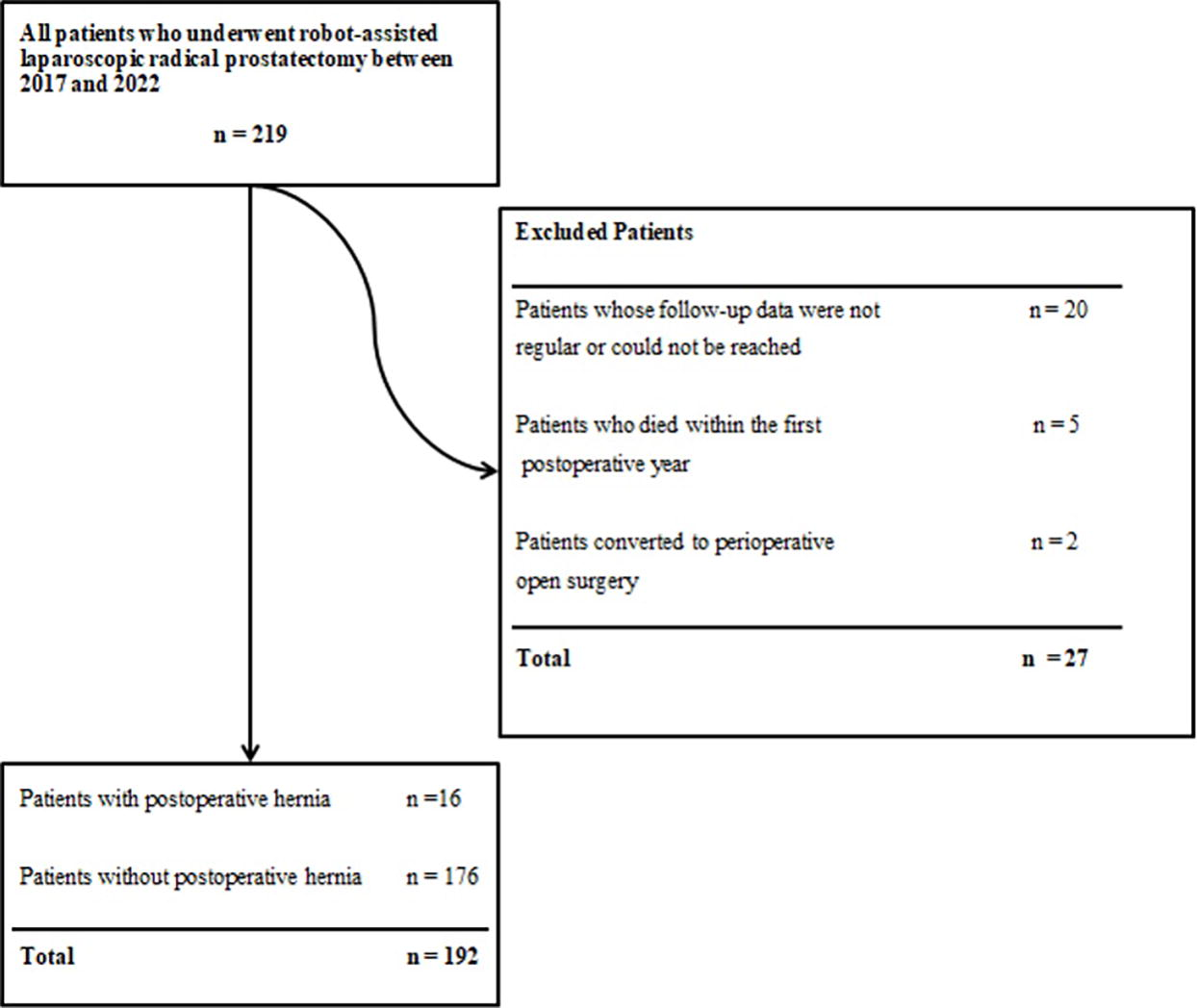
Flow chart for patient selection.
The demographic data and clinical characteristics of the patients are given in Table 1. The mean age of the patients in both groups was similar (P = .771). There was no significant difference between the two groups regarding BMI, the ASA score, or the ISUP grade (P = .241, P = .729, and P = .185, respectively). The mean prostate volume was calculated as 47 cm³ in Group 1 and 40 cm³ in Group 2 (P = .439). The number of patients with a history of abdominal surgery was 39 (22.15%) in Group 1 and 6 (37.5%) in Group 2, and there was no statistically significant difference between the groups (P = .214).
Demographics and Clinical Characteristics of All Patients
Data were expressed as median (range) or number (percentage) whenever appropriate.
Independent samples t-test.
Fisher’s exact test.
Mann–Whitney U test.
ASA, American Society of Anaesthesiologists; BMI, body mass index; ISUP, International Society of Urological Pathology.
Two preferred methods were used for specimen removal in patients: assistant port extension and the Pfannenstiel incision (PF), and the results of these methods were compared between the two groups (Table 2). Assistant port extension was preferred in 121 (89.6%) patients in Group 1 and 14 (10.4%) patients in Group 2, whereas the PF was used in 55 (96.5%) and 2 (3.5%) patients, respectively. According to these results, no significant difference was found between the two groups regarding the preferred method for specimen removal (P = .156).
Crosstab for Hernia Development
Data were expressed as number (percentage) whenever appropriate. Differences between patient subgroups assessed by
Fisher’s exact test as appropriate.
Discussion
In this study, we aimed to identify the factors affecting the occurrence of IH after RALRP and determine whether there was a relationship between the site of specimen removal and the occurrence of IH. We did not find any significant differences between different specimen removal incision techniques or any essential preoperative variables according to the IH development status of the patients. RALRP has several advantages over open surgery, including shorter recovery time, less pain, and better cosmetic results. 4 Although smaller incisions provide a better cosmetic appearance, complications such as IH may sometimes occur in these incisions. The rate of IH development was 8.3% in our study. In a systematic review of 22 studies, the incidence of trocar site hernia after laparoscopic surgery was found to be between 0% and 5.2%. 5 The risk factors affecting the development of trocar site hernia can be divided into two groups: surgical (trocar location and size, lack of fascia closure, and long operation time) and patient-related (diabetes mellitus, smoking, and advanced age).6,7
In our study, we evaluated the patients in terms of the incidence of symptomatic IH, but we may not have been able to detect the development of hernia in those who did not have clinical symptoms. Similarly, in a previous retrospective study, Christie et al. evaluated the development of IH in 104 patients who underwent robot-assisted partial nephrectomy, robot-assisted radical prostatectomy, or robot-assisted radical cystectomy and whose preoperative and postoperative computed tomography images were available. The authors found that the clinical hernia rate was 1.9% but the radiological hernia rate was higher (6.7%). 8
In this study, the demographic data and clinical characteristics of the patients in Group 1 and Group 2 were similar. There were no significant differences between the two groups in terms of BMI, prostate volume, and history of abdominal surgery. In the literature, the rate of IH after RALRP varies between 4.75% and 8.3%.9–11 Beck et al. found no statistically significant difference when they compared the mean BMI values of patients with and without IH (P = .058). 12 Seveso et al. reported that BMI did not increase the risk of IH development (P = .933). 11 Our results are concordant with the relevant literature.
It is considered that there may be a relationship between the size of the organ removed in laparoscopic surgery and the development of IH. In many studies, it has been observed that a large prostate volume constitutes a risk factor for the occurrence of IH because it requires a larger incision, especially during organ removal.11–13 Chennamsetty et al. found that the mean prostate volume was 45 g in the group with IH and 38 g in the group without IH (P < .001). 10 In our study, no significant difference was detected between the patients with and without IH in relation to prostate size; this may be related to our study being conducted with a relatively limited number of patients.
Previous abdominal surgery might affect IH occurrence. However, the current literature contains controversial data concerning this argument. Several studies observed that previous abdominal surgery other than cholecystectomy was not a risk factor for IH.8,9 Similarly, we did not find a significant relationship between previous abdominal surgery and IH occurrence.
In our study, two different incisions were used to remove specimens. When subgroup analysis was performed according to the incision method, the rates of PF and assistant port extension techniques were 3.5% and 10.3%, respectively (P = .156). At the time of our study, no other study was in the literature comparing these two incisions. In a study by Beck et al., a supraumbilical camera port was used for specimen removal, and the rate of hernia development after transverse-vertical incisions were compared. The authors found that IH occurred higher after vertical incisions (5.3% versus .6%, P = .005). 12 In another study of 800 patients, Seveso et al. compared the supraumbilical camera port (midline) with the lateral trocar site (off-midline) regarding specimen removal. According to the comparisons, the IH rate was 4.75% in the whole sample, 5% in the midline group, and 4.5% in the off-midline group, but the differences were not statistically significant. 11
Although we did not detect statistically significant differences between the incision methods, the PF seems more advantageous regarding the risk of IH occurrence. The risk of IH development may also increase as a result of impaired blood flow owing to excessive force applied to the abdominal wall by the trocars. 14 In addition, the 12-mm trocars with a blade used during assistant port access may increase the risk of trocar site hernia owing to their larger size. 15 The fact that the PF line does not have an entry hole for the trocars used during the RALRP may explain the lower risk of hernia in this incision. Moreover, since it is safer to close the fascia after the PF, the risk of IH is considered to be further reduced. However, in our study, the PF did not have significant superiority over trocar extension in preventing hernia development.
Our study has certain limitations; the most important is the retrospective design. In addition, IH was diagnosed based on physical examination findings. Some patients without IH may have asymptomatic occult hernias that can only be diagnosed radiologically, especially using computed tomography. Therefore, our IH rates may have been falsely low. In addition, the “small bite” technique, which is the method we preferred to close incisions, and the suture type we used are known to reduce hernia rates. 16
Conclusion
Ultimately, using the PF rather than the assistant port incision for specimen removal in RALRP seems to be more advantageous in terms of IH development, although it does not have statistically significant superiority. Prospective studies with a larger series of patients can provide clearer results on this subject.
Footnotes
Authors’ Contributions
E.D.: Conceptualization and writing—original draft; M.O.: Conceptualization and methodology; M.M.: Investigation, resources, and data curation; G.K.: Data curation, visualization, and formal analysis; K.C.S.: Investigation and formal analysis; M.H.G.: Project administration and methodology; C.D.: Resources and data curation; B.O.: Conceptualization, writing—review and editing, and supervision.
Ethical Approval
This study was approved by the institutional review board of our faculty.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
There is no funding source.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.