
Abstract
Introduction:
Right colon cancer often requires surgical intervention, and complete mesocolic excision (CME) has emerged as a standard procedure. The study aims to evaluate and compare the safety and efficacy of robotic and laparoscopic CME for patients with right colon cancer and 5-year survival rates examined to determine the outcomes.
Materials and Methods:
Patients who underwent CME for right-sided colon cancer between 2014 and 2021 were included in this study. Group differences of age, body mass index, operation time, bleeding amount, total harvested lymph nodes, and postoperative stay were analyzed by the Mann–Whitney U test. Group differences of sex, American Society of Anesthesiology, and tumor, node, and metastasis stage were analyzed by the Chi-squared test. Disease-free and overall survival were assessed using Kaplan–Meier curves with the log-rank Mantel–Cox test.
Results:
From 109 patients, 74 of them were 1:1 propensity score matched and used for analysis. Total harvested lymph node (P ≤ .001) and estimated blood loss (P = .031) were found to be statistically significant between the groups. We found no statistically significant difference between the groups in terms of disease-free and overall survival (P = .27, .86, respectively), and the mortality rate was 9.17%, with no deaths directly attributed to the surgery.
Conclusions:
Study shows that minimally invasive surgery is a feasible option for CME in right colon cancers, with acceptable overall survival rates. Although the robotic approach has a higher lymph node yield, there was no significant difference in survival rates. Further randomized trials are needed to determine the clinical significance of both approaches.
Introduction
Colorectal cancer is the third most common cancer and the second leading cause of cancer-related death worldwide.1,2 Despite advances in medical treatment, surgery remains a fundamental component of colorectal cancer treatment. Total mesorectal excision (TME) was first performed by Heald et al. in 1982. 3 TME involves resection of the rectum and mesorectum, along with its supplying vessels and lymph nodes, as an intact specimen. This dissection, which follows the embryological development of the rectum, has been shown to improve outcomes and decrease local recurrences.4,5 As a result, TME has become the standard treatment for rectal cancers.
In 2009, Hohenberger et al. introduced the concept of complete mesocolic excision (CME) for colon cancer, which is similar to TME. This technique involves dissection along the embryological plane, central ligation of the supplying vessels, and removal of the adequate colon. 6 By preserving the integrity of the visceral mesocolic layer and ensuring maximal lymph node resection, CME can yield better surgical specimens and improved survival and local recurrence rates compared to conventional techniques.7,8
Initially, CME was performed using laparotomy. However, with recent advances in minimally invasive surgery, laparoscopic and robotic approaches have become feasible alternatives. Laparoscopic surgery offers several advantages, such as reduced postoperative pain and shorter hospital stays. Recent studies have demonstrated that laparoscopic CME can yield high-quality surgical specimens, while also resulting in less postoperative pain, shorter hospital stays, fewer surgical infections, and better cosmetic outcomes.9–11 However, laparoscopic surgery has certain limitations, such as rigid instrumentation, limited depth perception, and range of motion. Robotic surgery may overcome some of these limitations.12,13
The aim of this study was to demonstrate and compare the safety, efficacy, and 5-year overall survival rates for robotic and laparoscopic CME for patients with right-sided colon cancer.
Materials and Methods
Study design and patient population
This single-center retrospective study includes patients diagnosed with right colon cancer stage 1-2-3 and operated on with curative laparoscopic or robotic CME between March 2014 and December 2021. Operations were done by a team with over 32 years of experience in laparoscopic surgery, and over 8 years of experience in robotic surgery. da Vinci Xi (Intuitive Surgical, Sunnyvale, CA, USA) system was used for robotic surgeries. All patients have undergone standard procedures of the department and no further care or diagnostic modality was used. Of 109 patients, 72 of them were operated with robotic CME, and remaining 37 of them were operated with laparoscopic CME. Robotic and laparoscopic CME groups were 1:1 propensity matched.
All procedures performed in the study involving human participants followed the ethical standards of the institutional and/or national research committee. The presented data within the scope of this study only involved a retrospective review of medical records. That allows for such reviews if the confidentiality of the patient’s data and her identity are protected. Informed consent was obtained. The study protocol was approved by the Institutional Review Board.
Age, gender, American Society of Anesthesiology (ASA) score, 14 and body mass index (BMI) were retrieved for patient characteristics analysis. Postoperative data include operation time, blood loss, length of postoperative stay, short-term complications (within 30 days), long-term complications (after 30 days), the total number of harvested lymph nodes, and tumor, node, and metastasis (TNM) staging data (Table 1). For the survival analysis, 1, 3, and 5 years of disease-free survival and overall survival data were retrieved (Table 2). The American Joint Committee on Cancer’s staging manual was used for staging the tumors. 15 Prior abdominal surgery histories were given with details in Table 3.
The Characteristics of the Study Sample
Details of Kaplan-Meier Curves and Log-Rank Mantel-Cox Tests
History of Prior Abdominal Surgery
Definitions
Operation time was defined as the time between the first incision and the final closure. The anastomotic leak was defined as a clinically or radiologically confirmed breach in the anastomosis. Discharge criteria were similar in both operations: Enteral feeding without any symptom established bowel or stoma function, adequate pain control with oral analgesia, and independent ambulation.
Surgical procedure
CME basically consists of a fine dissection of the visceral fascia layer from the parietal fascia layer, central vascular dissection (high tie), and adequate colonic resection. Vascular dissection starts after exposure of the superior mesenteric vein (SMV). Ileocolic, right colic, and middle colic vessels ligated from the connection of SMV or superior mesenteric artery (SMA). Feng et al. explained the detailed surgical technique of laparoscopic CME surgery 16 and used surgical technique of robotic CME surgery explained with details in previous article. 13 Circumferential radial margin involvement was accepted positive for tumors 1 mm close to the surgical margin.
All patients were placed in a supine position under general anesthesia. The surgeon and camera assistant stood at the left side of the patients. One 12-mm, one 10-mm, and two 5-mm trochars were used. The medial to lateral approach was preferred. Dissection starts with ileocolic vessels and ileocolic vessels ligated with endoclips close to the SMV. After completing the ligation of the right colic vessels, depending on the location of the tumor, colonic mesentery was dissected to its origin and middle colic vessels were identified and ligated. By doing so, the entire mesocolon removed as a whole. Lymph nodes were dissected at the origin of the vessels. Colon transection was done intracorporeally. Anastomosis was made intracorporeally or extracorporeally according to the operator’s choice.
Statistics
The statistical analyses were performed using the R Studio with R statistical software. A confidence interval (CI) of 95% was considered significant (P < .05). There was no missing data to exclude. A generalized liner model with parameters of age, sex, BMI, ASA grade, and TNM staging was used to calculate propensity scores. Propensity scores were used with 1:1 optimal matching and logistic link to diminish baseline variations between robotic and laparoscopic CME groups. A balanced match was defined as a mean standardized difference of the co-variables between the matched groups below .25. It was assumed that there was conditional independence of the outcome from the treatment status, taking into account the covariables used for matching. The skewness and kurtosis of the samples were analyzed. The Shapiro–Wilk test was utilized to assess the normality of data. All the continuous parameters were found to be not fitting the normal distribution. All the parameters were described with median ± interquartile (IQR) range. The distributions of groups are further demonstrated in Table 1. Categorical and ordinal parameters were described with absolute frequencies. Group differences of age, BMI, operation time, bleeding amount, total harvested lymph nodes, and postoperative hospital stay were analyzed by the Mann–Whitney U test. Group differences of sex, ASA, and TNM stage were analyzed by the Chi-squared test. Disease-free survival and overall survival were analyzed with Kaplan–Meier curves and compared with the log-rank Mantel–Cox test.
Results
In all, 109 patients with a mean age of 63.06 years were enrolled in the study. Of these, 74 patients with a mean age of 61.01 years were 1:1 propensity score matched and used for analysis.
Robotic and laparoscopic CME groups showed no statistically significant difference in age (robotic, 66–14.5 years [median-IQR] and laparoscopic, 61–18 years [median-IQR], P = .82), sex (P = 1), ASA (P = .35), BMI (robotic, 26.2–4.2 kg/m2 [median-IQR] and laparoscopic, 61–18 kg/m2 [median-IQR], P = .82), operation time (robotic, 340–60 minutes [median-IQR] and laparoscopic, 300–90 minutes [median-IQR], P = .09), TNM stage (P = .96), and postoperative hospital stay (robotic, 5–2 days [median-IQR] and laparoscopic, 5–2 days [median-IQR], P = .13). Robotic and laparoscopic CME groups showed statistically significant differences in bleeding amount (robotic, 10–50 mL [median-IQR] and laparoscopic, 40–90 mL [median-IQR], P = .03) and total harvested lymph nodes (robotic, 48–25 [median-IQR] and laparoscopic, 34–22 [median-IQR], P ≤ .001). Furthermore, all parameters are measured and summarized in Table 1.
None of the cases was converted. Duodenal perforation on postoperative day 4 was observed on the robotic CME group. Robotic wedge resection and primary repair were done. A patient in the laparoscopic CME group had intra-abdominal bleeding, and after a diagnostic laparoscopy, no active bleeding was observed. One intra-abdominal abscess was developed in the robotic group and successfully controlled with drainage catheter. Paralytic ileus was observed in each group.
The mortality rate was 9.17 (10/109) and none of them was directly linked to surgeries. Seven of them died from metastatic disease (five in the liver, one in the lung, and one in the duodenum), two from heart failure, and one from COVID-19.
The mean overall survival of the entire study cohort was 41.47 months (median 40.27; IQR 46.8). The mean overall survival of the matched cohort was 38.22 months (median 41.85; IQR 50.53). All patients were in the follow-up process throughout survival period.
Overall 1-, 3-, and 5-year survival was 98.9% (CI 96.7%–100%, SE 1%), 91.7% (CI 85.5%–98.3%, SE 3%), and 83.5% (CI 74.1%–94%, SE 5%), respectively, in all 109 patients and 100% (CI 100%–100%, SE 0%), 95.7% (CI 89.9%–100%, SE 3%), and 93.3% (CI 86.3%–100%, SE 4%), respectively, in 74 matched patients. Robotic CME surgery showed 93% (CI 84%–100%, SE 5%) overall survival and 87% (CI 75%–99%, SE 6%) disease-free survival. Laparoscopic CME surgery showed 94% (CI 83%–100%, SE 6%) overall survival and 71% (CI 54%–96%, SE 5%) disease-free survival. Further details of 1-, 3-, and 5-year survival and log-rank Mantel–Cox test are given in Table 2. Robotic and laparoscopic CME surgery showed no statistically significant difference with regard to disease-free and overall survival (P = .27, P = .86, respectively). Kaplan–Meier curves of disease-free survival and overall survival are shown in Figures 1 and 2, respectively.
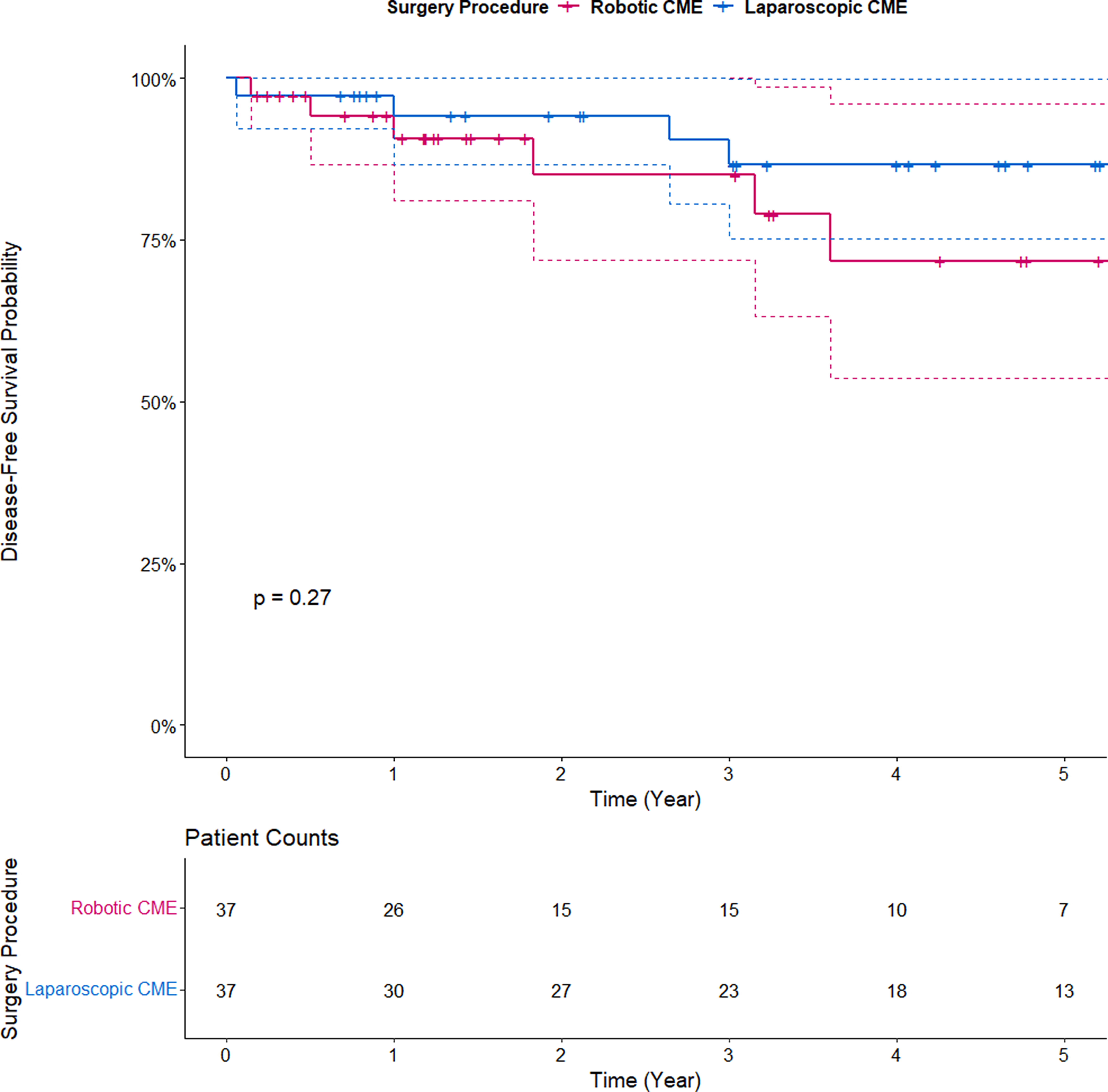
Kaplan–Meier curve of disease-free survival.
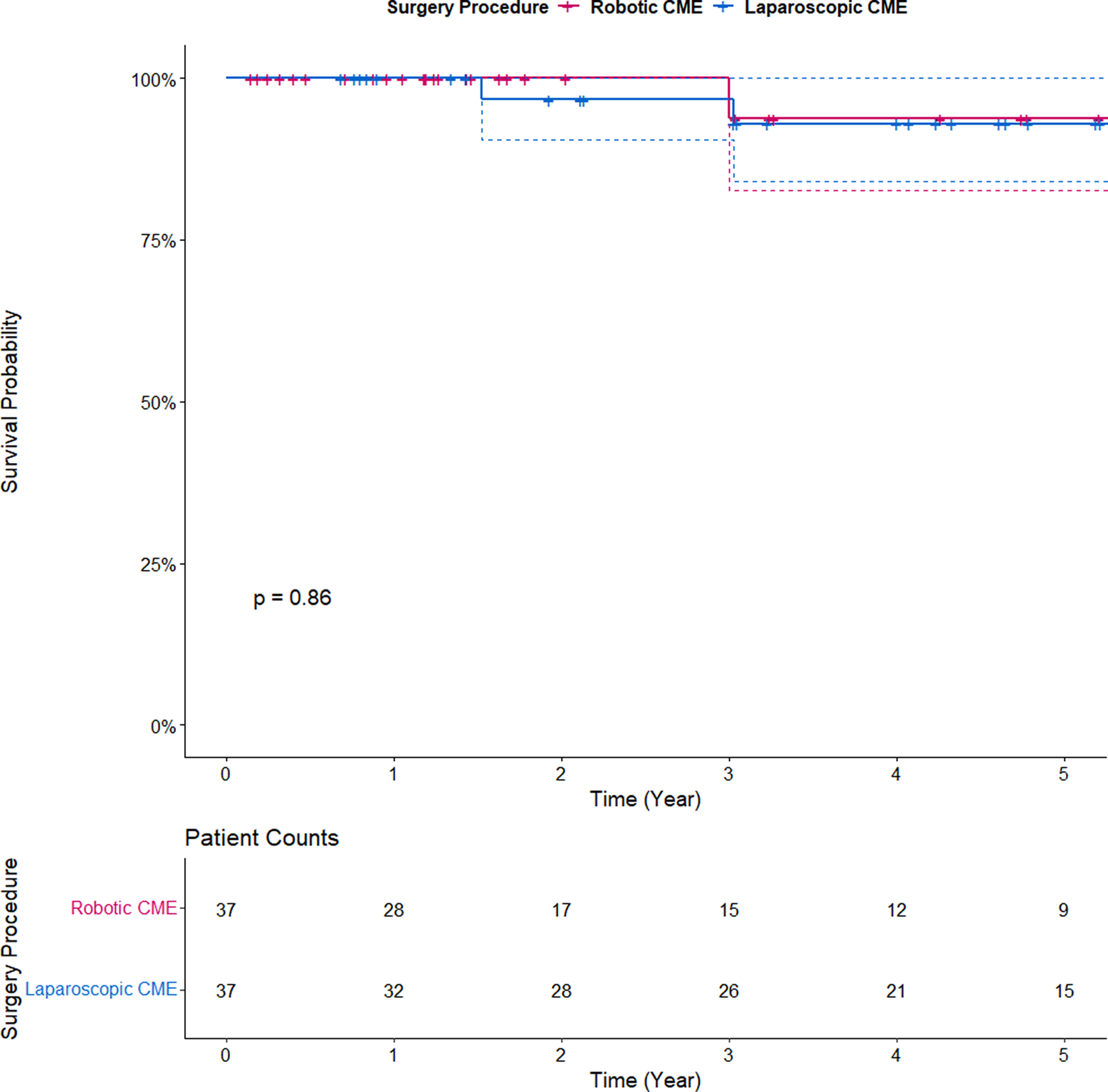
Kaplan–Meier curve of overall survival.
Discussion
In this study, laparoscopic and robotic CME for right colon cancer were evaluated and postoperative outcomes along with 1-, 3-, and 5-year survival rates were analyzed. Our study demonstrates that CME for right colon cancers is safely performable with minimally invasive surgery and total survival rates are acceptable. Despite better lymph node yield with the robotic approach, robotic and laparoscopic approaches showed no difference in survival rates.
Operation time is a factor that would be a potential difference between laparoscopic and robotic CME. A meta-analysis by Cuk et al. shows robotic CME requires a longer operative time than laparoscopic CME. 17 Docking time and most importantly surgeon’s learning curve possibly constitute this difference. Increasing surgeon experience in relation to the number of cases decreases operation time. de'Angelis et al. show that this learning process is faster for robotic surgery. 17 In this study, although robotic CME requires more time than laparoscopic CME (robotic, 340–60 minutes [median-IQR], and laparoscopic, 300-90 minutes [median-IQR], P = .09), we found no statistically significant difference in operation time between two groups. This may be explained by the experience of the surgical team in robotics.
There is always a possibility of conversion to laparotomy during minimally invasive surgery. Vascular and/or organ injury may occur and could be difficult to repair laparoscopically. 18 Technical advantages of robotic surgery may allow lower conversion rates than laparoscopy. 19 Comparisons of laparoscopic and robotic CME in the literature show that conversion to laparotomy is lower with the robotic approach.19–23 In our study, none of the cases needed to be converted to laparotomy in both groups.
Anastomosis could be done intracorporeally or extracorporeally. Intracorporeal anastomosis enables lesser short-term morbidity such as quicker bowel movement, shorter hospital stay, and better cosmetic results with smaller incision size.24,25 One controversial point is operation time. Vignali et al. report a longer operation time in the intracorporeal group in their randomized controlled trial. On the other hand, a meta-analysis showed no statistically significant difference between two techniques as in most of the studies. 26 Park et al. stated that in their randomized control trial study, port location in robotic approach limits periumbilical minilaparotomy. Thus, intracorporeal anastomosis is more often used in robotic approach in their randomized control trail. 27 This contradiction about operation time could be related to the experience level or incomplete learning curve of the operator. We preferred intracorporeal technique in our study.
Postoperative complications of colorectal resections include surgical site infection, intra-abdominal abscess, anastomotic leakage, bleeding, and ileus. Some publications claim that complications are higher with CME during vascular dissection.8,28,29 On the other hand, Anania et al. report that laparoscopy offers lower postoperative complications within the first 30 days. Lower complication rates such as estimated blood loss and wound infection rates lead to shorter hospital stays. 18 In addition, robotic CME provides better results in terms of postoperative complications in a meta-analysis that compares robotic and laparoscopic CME. 22 Robotic surgery could decrease complication rates or allow easier intervention to possible complications. We could report that similar results were obtained in our study. The estimated blood loss is significantly lower in our robotic CME group. (robotic, 10–50 mL [median-IQR] and laparoscopic, 40–90 minutes [median-IQR], P = .03).
The lymph node metastasis is an indicative factor for surgical quality and disease staging as part of the TNM staging system. 30 With the introduction of CME for colon cancers in 2009, Hohenberger et al. reported better lymph node yields with this technique. 6 A systematic review by Killeen et al. indicated that lymph node yield is greater in CME specimens. 31 Magistro et al. stated laparoscopic CME is similar in mortality and complication aspects with conventional hemicolectomy, with better nodal sampling and improved staging. 32 After implementing the minimally invasive techniques for colorectal surgery, higher lymph node yields were obtained with the highest ratios using robots, as shown in the studies of Widmar et al. and Yozgatli et al.33,34 Likewise, Dohrn et al. reported that in the robotic approach, lymph node yield was significantly higher with similar postoperative morbidity. 35 In this study, the number of total harvested lymph nodes is high in both groups. In comparison, we report better lymph node yield in our robotic group (robotic, 48–25 [median-IQR], and laparoscopic, 34–22 [median-IQR], P ≤ .001). Three additional evaluable lymph nodes (IQR) were obtained by robotic assistance without evidence that staging is impacted, and thus survival was not altered. Our findings are compatible with existing studies in the literature.34,36
Survival rates are an important element to understand and compare long-term outcomes. In meta-analysis, De Simoni et al. stated that CME exhibits better survival rates than conventional hemicolectomy, with similar postoperative complication rates. 37 According to some comparative studies, both approaches did not provide advantages over each other in survival rates.21,22 A prospective randomized study presented no statistically significant difference between laparoscopic CME and robotic CME in terms of overall survival and disease-free 3- and 5-year survival rates. 23 Despite the acceptable overall survival rates, we also found no significant difference between the laparoscopic and robotic groups.
The strengths of this study are the follow-up to 5 years and the use of equivalent procedures during surgery for both groups. However, this study also has certain limitations. The retrospective design of this study generates its major limitation. Long-term results of the randomized controlled trials are needed to confirm the differences between the outcomes of the two techniques. At present, the COLD Trial, RELARC, and RoLaCaRT-1 trials are in progress.37–40 After the trials are ended, our results are going to be compared to achieve high-quality evidence. This study does not include cost calculation, and this could be a potential limitation. Moreover, studies with bigger population sizes could produce more robust results.
Conclusion
Our study demonstrates that CME for right colon cancers is feasible with minimally invasive surgery and total survival rates are acceptable. Despite better lymph node yield with the robotic approach, robotic and laparoscopic approaches showed no difference in survival rates. Further randomized trials are needed to define the significance of both approaches.
Footnotes
Authors’ Contributions
Each author has made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data. Each author has approved the submitted version (and any substantially modified version that involves the author’s contribution to the study). Each author has agreed to be personally accountable for the author’s contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated and resolved, and the resolution documented in the literature.
Ethical Statement and Consent to Participate
All procedures performed in the study involving human participants followed the ethical standards of the institutional and/or national research committee. The presented data within the scope of this study only involved a retrospective review of medical records. That allows for such reviews if the confidentiality of the patient’s data and her identity are protected. Informed consent was obtained. The study protocol was approved by the Institutional Review Board.
Availability of Data and Material
Data access requests by qualified researchers trained in human subject confidentiality protocols should be sent to the corresponding author.
Oral Presentation
Findings of the study were presented as oral presentation (National Surgery Congress, March 23–27, 2022, Antalya, Turkey).
Disclosure Statement
All authors declare no conflict of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.