
Abstract
Background:
Laparoscopic common bile duct exploration (LCBDE) proves a safe and effective treatment for choledochal stones. After LCBDE, preferred choledochal closure is favored for short- and long-term outcomes compared with t-tube drainage. However, there are no relevant studies on the technique of layered closure of the common bile duct with double-needle bidirectional barbed suture at home and abroad.
Materials and Methods:
A retrospective study of 37 patients who underwent laparoscopic choledochotomy from January 2021 to October 2023 in our hospital was performed. A continuous layered one-stage suture using two-needle bidirectional barb wire. The primary outcomes were stone clearance, operative time, blood loss, and complications. Secondary outcomes were complications, length of hospitalization, and time to drain removal.
Results:
During the study period, laparoscopic surgery was successful in all cases, and the initial stones were removed without complications.
Conclusion:
The treatment of choledocholithiasis with continuous layered one-stage suture with double-needle bidirectional barbed wire after LCBDE is a new convenient and effective treatment in selected patients.
Introduction
Cholelithiasis is a common and frequent disease of the digestive system, mainly including gallbladder stones and common bile duct stones. The incidence of gallbladder stones in adults is 6%–10%, of which 5%–15% of patients also suffer from choledocholithiasis, which can cause a series of serious complications, such as acute cholangitis and cholestatic pancreatitis. 1 Laparoscopic common bile duct exploration (LCBDE) proves a safe and effective treatment for choledochal stones. On the one hand, it can achieve stone removal rates comparable to endoscopic surgery without increasing morbidity and mortality. 2 On the other hand, it is a single-stage procedure and also preserves the function of Oddi’s sphincter. After LCBDE, preferred choledochal closure is favored for short- and long-term outcomes compared with t-tube drainage. 3 Historically and presently, choledochotomy incisions are primarily closed intermittently with 3/4–0 Vycho thread. Due to visual and spatial constraints, knots needed to be tied after each stitch and therefore could take a lot of time. In recent years, the utilization of barbed sutures in abdominal surgery has been increasing. 4 However, there are no relevant studies on the technique of layered closure of the common bile duct with double-needle bidirectional barbed suture at home and abroad (Fig. 1). Our team innovatively used a two-needle bidirectional barbed wire for one-stage suturing of the common bile duct, and we now report the application of this method with clinical experience and personal experience.
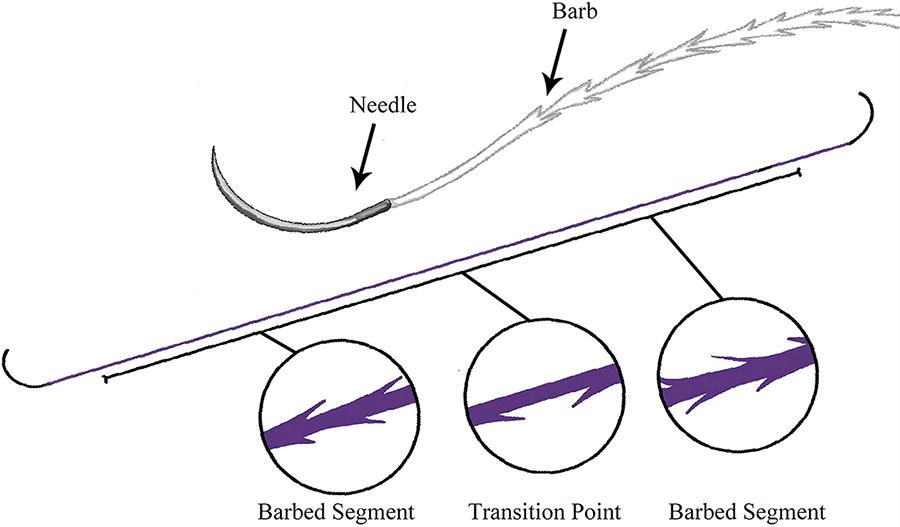
Schematic diagram of a two-needle bidirectional barbed wire.
Materials and Methods
The study included 37 patients who underwent laparoscopic choledochotomy with continuous layered one-stage suture using two-needle bidirectional barb wire from January 2021 to October 2023 at our hospital. The mean age was 64.6 years and 28 (75.7%) were female. Three patients who had already undergone previous cholecystectomy. The mean diameter of the common bile duct was 12.9 ± .3 mm.
Under general anesthesia, the patient was placed in the supine position with the head elevated and the right side elevated. A 1 cm incision was made below the umbilicus, a pneumoperitoneum was established, and the intra-abdominal pressure was controlled at 12–14 mmHg. The main operation hole of 1 cm was located at 4–5cm below the xiphoid process, and two 5 mm auxiliary operation holes were located at the right midclavicular line and 2–3 cm below the rib margin of the right anterior axillary line. The bottom of the gallbladder was clamped and pulled upward to the right, the triangle of the gallbladder was separated and dissected, the gallbladder artery was cut off after the supra-hemlock, and the choledochal duct was clamped without being cut off, the neck of the gallbladder was lifted by the grasping forceps and the hepatic-duodenal ligament was revealed by upward traction. Electrocoagulation hook cut the anterior peritoneum of the common bile duct to reveal the common bile duct, electrocoagulation hook set the pre-cut line, cut the anterior wall of the common bile duct with scissors from the pre-cut line, adjust the size of incision according to the size of the stone, and suction the overflowed bile. The common bile duct stones were removed in the order of silicone tube flushing, choledochoscope exploration, and stone extraction basket grasping. Use choledochoscope to probe the common bile duct up and down without any abnormality and then suture the common bile duct. The common bile duct was closed with a double-needle, bidirectional barbed wire (RA-1012Q, QUILL, USA) in consecutive layers, with the first stitch starting from the normal bile duct, and after the completion of the first stitch, another stitch was placed in the original position, and the double-needle, bidirectional was bounded by the midpoint of the barbed wire.
The inner layer was closed with continuous sutures on the anterior wall of the common bile duct using a single needle on one side (Fig. 2), while the outer layer was closed with continuous sutures on the anterior plasma membrane of the common bile duct using a single needle on the other side (Fig. 3). Sutures were positioned at a distance of approximately 2.0–3.0 mm, with margins of approximately 1.0–2.0 mm, extending a point 2.0 mm below the common bile duct incision, followed by a final back stitch. After the suture was completed, saline was used to rinse, and gauze was used to wipe the suture with slight pressure to check for bleeding and bile leakage. The gallbladder and stones were excised and removed, the abdominal cavity was rinsed with saline and suctioned, and an abdominal drainage tube was routinely placed through the anterior axillary line puncture hole in the Winch’s orifice, and the nature and amount of drainage fluid was observed and recorded postoperatively.

Continuous suture of the anterior wall of the common bile duct.

Continuous suture of the anterior plasma membrane of the common bile duct.
The gallbladder and stones were excised and removed, the abdominal cavity was rinsed with saline and suctioned, and an abdominal drainage tube was routinely placed through the anterior axillary line in the foramen of Winters, and the nature and amount of drainage fluid was observed and recorded after the operation.
Results
Laparoscopic surgery was successful in all cases during the study period and initial stones were removed. The mean operative time was 111.2 ± 39.3 minutes, the estimated blood loss was 16.8 ± 9.4 mL, the postoperative hospital stay was 7.4 ± 2.2 days, and the time to remove the drain was 4.6 ± 1.3 days. The perioperative patients had no complications such as postoperative hemorrhage or biliary fistulae. There were no deaths during the perioperative period.
Discussion
Barbed suture was first introduced in 1951. 5 So far, it has made great progress in material and design. Barbed sutures are sutures that have protrusions along the length of the fibers that promote self-anchoring of the surrounding tissue. These barbs enhance suture adhesion at the wound site and reduce the amount of time the surgeon has to spend using these barbed sutures during the procedure. Barbed sutures have a lower and more uniform stress distribution than traditional smooth monofilament sutures. Because barbed sutures are manufactured from monofilaments without any internal holes, there are fewer infections and a lower risk of an immune response from the host. Barbed sutures are used in a variety of procedures, most commonly in reconstructive and plastic surgery, as they help surgeons approach the skin efficiently and quickly and provide better tissue adhesion and support during and after surgery. When using barbed sutures, surgeons have also found that less suture material is needed to close the dermal tissue and the procedure takes less time compared to traditional sutures. 6
Bidirectional barbed sutures are unique in that there is an intermediate transition point where the direction of the barb changes. Using a bidirectional barbed suture instead of a traditional monofilament suture offers significant advantages in terms of increased placement speed, easier handling, and freedom from knots. Relevant clinical studies suggest that the use of barbed sutures significantly reduces suture time compared with conventional sutures. Procedures such as abdominoplasty, brachioplasty (upper arm lift) and breast fixation (breast lift) require approximation of three layers of tissue, i.e., superficial fascia/deep tissue, deep dermis, and superficial dermis. Using traditional suturing techniques with conventional sutures to approximate these three layers requires three separate sutures, whereas when using bidirectional barbed sutures, only two running sutures are required, reducing the suturing time by approximately 50%. 7
A large number of studies have been conducted on the use of unidirectional barbed wire for continuous whole-layer suturing or ordinary absorbable wire for layered suturing. However, there are no studies at home and abroad on the application of continuous layered bile duct closure with two-needle bidirectional barbed wire in laparoscopic stage I bile duct closure surgery, which was summarized and improved by our team and applied in the clinic with certain results.
Double-needle bidirectional barbed wire continuous layered suture was not performed in the same needle under the anterior wall of the common bile duct and the anterior plasma membrane of the whole layer of suture, but the formation of cross-layer suture, not only reduces the single suture internal soft tissue, reduces the tension of the suture, but also reinforces the effect of the whole layer of the suture, played a “double insurance” role, even if there is a local needle eye leak in the common bile duct, the anterior plasma layer of the common bile duct that is sutured by the layer of the suture can play a part of the role of the blocking of leakage of bile, so as to further reduce the biliary bleeding, bile leakage, and the complications such as bile duct stenosis, and to reduce the number of days of hospitalization after the operation and the total hospitalization cost, which is in line with the acceleration of the rehabilitation of the surgical concept.
Conclusion
In conclusion, the treatment of choledocholithiasis with continuous layered one-stage suture with double-needle bidirectional barbed wire after LCBDE is a new convenient and effective treatment in selected patients.
Institutional Review Board Statement
The study was reviewed and approved by the Institutional Review Board at Wujin Hospital affiliated with Jiangsu University approved this study (2024-SR-001).
Footnotes
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.