
Abstract
Background:
Celiac axis stenosis can potentially lead to insufficient blood supply to vital organs, such as the liver, spleen, pancreas, and stomach. This condition result in the development of collateral circulation between the superior mesenteric artery and the hepatic artery. However, these collateral circulations are often disrupted during pancreaticoduodenectomy (PD), which may increase the risk of postoperative complications.
Methods:
A retrospective analysis was conducted on patients who underwent laparoscopic pancreaticoduodenectomy (LPD) from April 2015 to April 2023. Celiac trunk stenosis is classified according to the degree of stenosis: no stenosis (<30%), grade A (30%–<50%), grade B (50%–≤80%), and grade C (>80%). The incidence of postoperative complications was evaluated, and both univariate and multivariate risk analyses were conducted.
Results:
A total of 997 patients were included in the study, with mild celiac axis stenosis present in 23 (2.3%) patients, moderate stenosis in 18 (1.8%) patients, and severe stenosis in 10 (1.0%) patients. Independent risk factors for the development of bile leakage, as identified by both univariate and multivariate analyses, included body mass index (BMI) (HR = 1.108, 95% CI = 1.008–1.218, P = .033), intra-abdominal infection (HR = 2.607, 95% CI = 1.308–5.196, P = .006), postoperative hemorrhage (HR = 4.510, 95% CI = 2.048–9.930, P = <0.001), and celiac axis stenosis (50%–≤80%, HR = 4.235, 95% CI = 1.153–15.558, P = .030), and (>80%, HR = 4.728, 95% CI = .882–25.341, P = .047). Celiac axis stenosis, however, was not determined to be an independent risk factor for pancreatic fistula (P > 0.05). Additionally, the presence of an aberrant hepatic artery did not significantly increase the risk of postoperative complications when compared with celiac axis stenosis alone.
Conclusion:
Severe celiac axis stenosis is an independent risk factor for postoperative bile leakage following LPD.
Introduction
Median arcuate ligament compression and atherosclerosis are identified as the primary etiologies of celiac axis stenosis. In cases of severe celiac axis stenosis, there is often relative insufficient blood supply to organs, such as the liver, spleen, pancreas, and stomach, thereby fostering the development of collateral circulation between the superior mesenteric artery (SMA) and the hepatic artery. 1 Pancreaticoduodenectomy (PD), the standard procedure for periampullary tumors, 2 frequently disrupts these collateral circulations, with a complication rate of approximately 30% to 60%.3,4
Among various complications, anastomotic leakage holds a prominent position, which not only contributes to intra-abdominal infection and bleeding but also prolongs hospital stay and increases health care costs, and can even result in mortality. 5 To reduce the incidence of postoperative complications, several risk factors have been investigated, including BMI, intraoperative blood transfusion, malnutrition, pancreatic texture, pancreatic duct size, and celiac axis stenosis.
However, regarding the risk factor of celiac artery stenosis, further investigation is needed to determine whether varying degrees of stenosis consistently increase the occurrence of postoperative complications. Previous studies have predominantly focused on reporting the definition of celiac axis stenosis and its intraoperative management.6,7 There is a scarcity of research reports regarding the relationship between the grading of stenosis and postoperative complications.
Therefore, in this article, we categorized the severity of celiac axis stenosis and examined whether varying degrees of celiac artery stenosis is all an independent risk factor contributing to postoperative complications.
Methods
Study population
A retrospective analysis was conducted for this comparative study. Due to the retrospective nature of this research, ethics approval was waived. The study included a total of 1176 patients who underwent laparoscopic pancreaticoduodenectomy (LPD) at our center from April 2015 to April 2023. To ensure homogeneity in patient characteristics, the final analysis excluded patients with the following clinical conditions: (1) Receiving palliative resection; (2) Surgical conversion due to various reasons; and (3) Lack of complete clinical data. As a result, 45 individuals lacked complete clinical data, 34 individuals underwent palliative surgical resection, and 100 individuals experienced surgical conversion due to various reasons. Consequently, the final analysis comprised a total of 997 patients (Fig. 1).

Flow chart of cohort creation.
Study variables
This study analyzed a comprehensive dataset encompassing preoperative, intraoperative, and postoperative parameters. Preoperative data included patient demographics, American Society of Anesthesiologists classification, CA125, CA199 levels, diabetes, celiac axis stenosis, and aberrant hepatic artery. Intraoperative variables encompassed surgical resection duration, estimated blood loss, transfusion requirement, and pancreatic texture. Postoperative data included postoperative pancreatic fistula (POPF), bile leakage, delayed gastric emptying (DGE), postoperative hemorrhage (PPH), Clavien–Dindo classification ≥ grade III, and duration of postoperative hospital stay.
The definitions and classifications of postoperative POPF, PPH, DGE, and bile leakage were based on internationally recognized guidelines.5,8–10 Postoperative complications were categorized according to the Clavien–Dindo classification system. 11
Assessment of CAS
To assess the presence of celiac axis stenosis, all participants underwent preoperative abdominal CT scans with contrast-enhanced phases, followed by further processing with three-dimensional reconstruction. Subsequently, three associate professors, blinded to clinical outcomes, evaluated the sagittal images of the three-dimensional reconstructions to determine the presence of celiac axis stenosis.
The stenosis was classified based on its etiology as either extrinsic or intrinsic. Furthermore, employing the grading system proposed by Sugae T, it was further categorized as mild (<50%), moderate (50%–≤80%), or severe (>80%) (Fig. 2). 12

The sagittal plane three-dimensional reconstruction examples of the celiac trunk are presented, including the normal celiac trunk
Statistical analyses
All statistical analyses were performed using SPSS statistical software (version 27). Continuous variables are expressed as mean ± standard deviation, while categorical variables are presented as frequencies and proportions. For continuous variables, the Kruskal–Wallis test was employed, whereas the chi-square or Fisher’s exact test was used for categorical variables. A univariate analysis was performed to identify factors associated with bile leakage and pancreatic fistula following LPD. Variables that were significant (P < .05) in the univariate analysis were incorporated into a multivariate binary logistic regression analysis to determine independent predictors of POPF and bile leakage following LPD. A P value less than .05 was considered statistically significant.
Results
Demographic characteristics and preoperative data
Between April 2015 and April 2023, a total of 997 cases were analyzed in this study, after excluding missing and disqualified data. The average age of all patients was 58.54 ± 10.85 years, with 567 males (56.87%). The most common indications for LPD were cholangiocarcinoma (29.5%), followed by pancreatic cancer (26.8%), and then periampullary cancer (24.1%). Demographic and preoperative data for the study cohort are summarized in Table 1.
Demographic Characteristics and Preoperative Data of the Patients
BMI, Body mass index; ENBD, endoscopic nasobiliary drainage; PTCD, percutaneous transhepatic cholangial drainage; PTGBD, Percutaneous transhepatic gallbladder puncture drainage.
Celiac axis stenosis and aberrant hepatic artery
A comprehensive three-dimensional postprocessing evaluation identified a total of 23 cases with mild celiac axis stenosis, 18 with moderate stenosis, and 10 with severe stenosis. The perioperative complications associated with celiac axis stenosis of different etiologies are presented in Table 2.
Perioperative Complications of Intrinsic and Extrinsic Stenosis of the Celiac Axis
DGE, delayed gastric emptying; POPF, Postoperative pancreatic fistula; PPH, postoperative pancreatic hemorrhage.
Of these patients, 11 had concomitant aberrant hepatic arteries. The most prevalent type was the replaced right hepatic artery originating from the superior mesenteric artery (45.45%), followed by the accessory right hepatic artery originating from the superior mesenteric artery (27.27%) (Table 3).
Classification of Celiac Axis Stenosis and Variation of Hepatic Artery
aLHA, accessory left hepatic artery; aRHA, accessory right hepatic artery; CHA, common hepatic artery; LGA, left gastric artery; rLHA, replace left hepatic artery; rRHA, replace right hepatic artery; SMA, superior mesenteric artery.
The relationship between celiac axis stenosis and postoperative complications
The correlation between celiac axis stenosis (CAS) and postoperative outcomes is illustrated in Table 4. A significant association was observed between CAS and intraoperative blood loss (P = .017), time of operation (P = .046), bile leakage (P = .030), and chylous leakage (P = .016) following LPD. As the severity of celiac axis stenosis increased, we noted a gradual increase in the incidence of pancreatic fistula and Clavien–Dindo ≥ 3, as well as an increase in intraoperative blood loss, surgical duration, bile leakage, and chylous fistula (Fig. 3). However, no statistically significant differences were found in Clavien–Dindo grade ≥ 3 and pancreatic fistula.
Perioperative Outcomes of Those Patients
DGE, delayed gastric emptying; POPF, Postoperative pancreatic fistula; PPH, postoperative pancreatic hemorrhage.
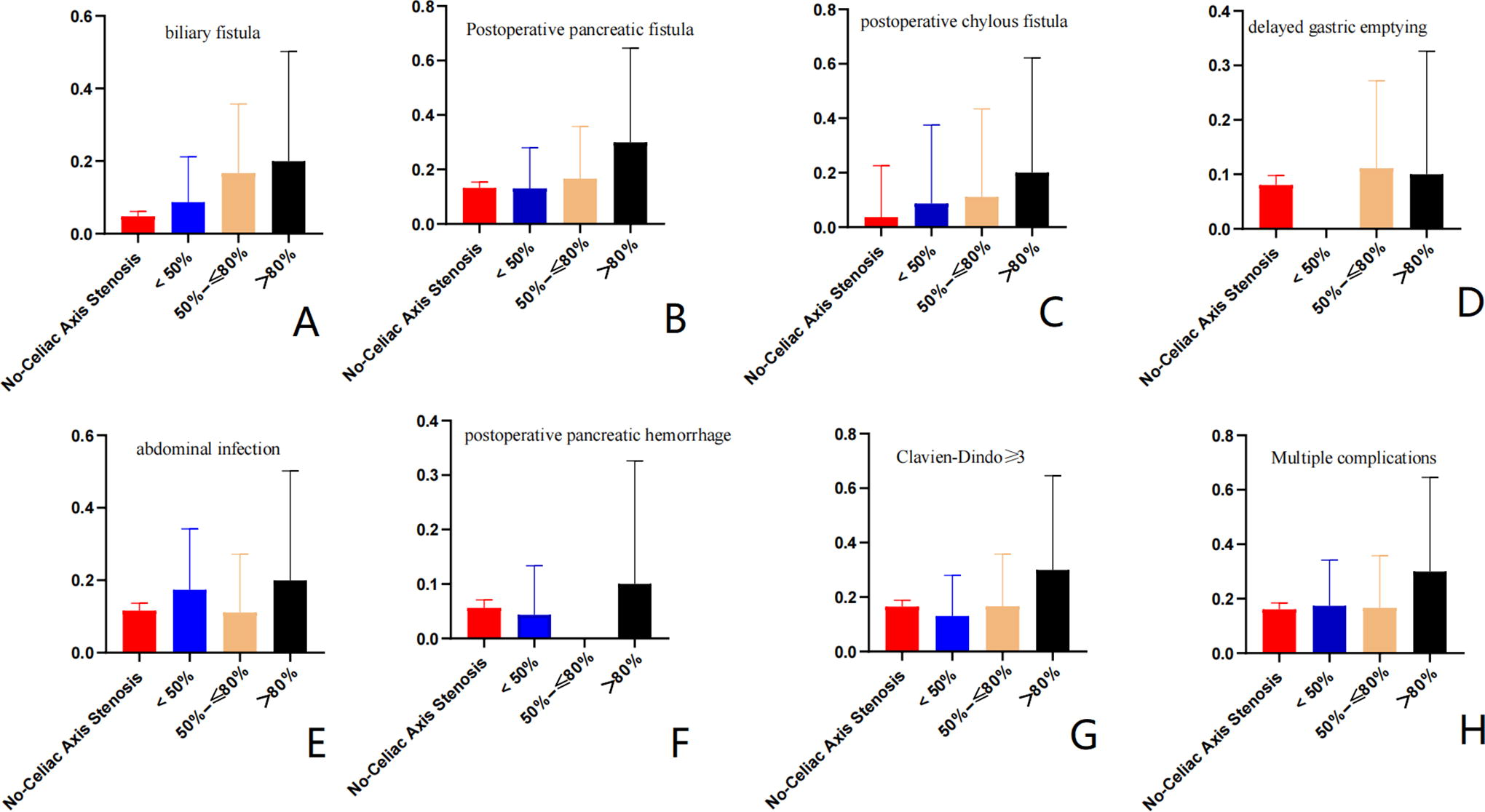
The relationship between grades of celiac axis stenosis and postoperative complications.
The relationship between celiac axis stenosis with aberrant hepatic artery and postoperative complications
An analysis was conducted to explore whether aberrant hepatic artery presence could improve the incidence of perioperative complications. However, we founded that the occurrence of perioperative complications, including chylous fistula, POPF, DGE, abdominal infection, and in-hospital mortality, was markedly elevated in the celiac axis stenosis with an aberrant hepatic artery. However, it is important to note that these differences did not reach statistical significance (Table 5).
Compare Outcomes of Those Patients with Celiac Axis Stenosis (with or without AHA)
AHA, Abnormal hepatic artery; DGE, delayed gastric emptying; POPF, postoperative pancreatic fistula; PPH, postoperative pancreatic hemorrhage.
Celiac axis stenosis as independent risk factor for biliary fistula
To further investigate the relationship between celiac axis stenosis and bile leakage and POPF, we conducted a univariate and multivariate analysis revealed that BMI (HR = 1.136, 95% CI = 1.065–1.212, P < 0.001), postoperative pancreatic hemorrhage (HR = 10.042, 95% CI = 5.391–18.705, P < 0.001), pancreatic duct diameter (HR = .795, 95% CI = .680–0.930, P = .004), and intra-abdominal infection (HR = 3.387, 95% CI = 2.078–5.520, P < 0.001) were independent risk factors for POPF. Additionally, we discovered that BMI (HR = 1.108, 95% CI = 1.008–1.218, P = .033), intra-abdominal infection (HR = 2.607, 95% CI = 1.308–5.196, P = .006), postoperative hemorrhage (HR = 4.510, 95% CI = 2.048–9.930, P = <0.001), and celiac axis stenosis(50%–80%, HR = 4.235, 95% CI = 1.153–15.558, P = .030), and (>80%, HR = 4.728, 95% CI = .882–25.341, P = .047) were independent risk factors for postoperative bile leakage (Table 6).
Univariable and Multivariate Analysis of Pancreatic Fistula and Bile Leakage after LPD
ASA, American Society of Anesthesiologists; BMI, Body mass index; LPD, laparoscopic pancreaticoduodenectomy; POPF, postoperative pancreatic fistula; PPH, postoperative pancreatic hemorrhage.
Discussion
In recent years, advancements in surgical techniques and improvements in perioperative management have significantly reduced the postoperative mortality rates following pancreaticoduodenectomy (PD), from around 25% to approximately 3% to 5%. 13 Despite these advancements, the incidence of postoperative complications remains high, ranging from 20% to 30%, with many of these complications associated with anastomotic issues. 14 Among these, bile leakage, which occurs in 1% to 8%, has a relatively lower incidence rate compared with other complications such as pancreatic fistula, postoperative hemorrhage, and delayed gastric emptying. 15 Several studies have identified risk factors for postoperative bile leakage following PD, including preoperative nutritional status, serum albumin levels, bile duct diameter, and gender.3,16,17 In our study, we explored the impact of celiac axis stenosis on perioperative complications and found that celiac axis stenosis is an independent risk factor for bile leakage after LPD.
Celiac axis stenosis may present as intrinsic, often frequently attributed to atherosclerosis, or as extrinsic, typically induced by the median arcuate ligament.
In cases of stenosis, the pancreaticoduodenal arcade and the dorsal pancreatic artery become essential collateral pathways. Notably, about 28% of individuals with celiac axis stenosis are asymptomatic, which is largely attributable to the compensatory collateral circulation between the celiac axis and the superior mesenteric artery.
However, during PD, interruption of this collateral circulation can lead to inadequate perfusion of the residual pancreas, bile ducts, liver, and stomach, resulting in complications. 15 In a study by Al-Saeedi et al., it was reported that celiac axis stenosis increases the occurrence of postoperative pancreatic fistula, inadequate liver perfusion, and gastric complications. It is an independent risk factor that should not be underestimated following PD. 18 On the contrary, Smith et al. suggest that there is no correlation between celiac axis stenosis and postoperative complications in PD when the degree of stenosis is less than 60%. 13 According to Yoshida et al., in cases of severe stenosis (with a stenosis rate of 80% or higher) and a small distance between the stenosis and the aorta, it is necessary to preserve collateral circulation or perform reconstruction as much as possible to reduce the occurrence of postoperative complications. 19 In a retrospective analysis of data from our center, we also observed a higher occurrence of bile leakage in patients with celiac axis stenosis, which is consistent with Zhou Y’s report. 3 Meanwhile, in terms of univariate analysis of bile leakage, previous studies have reported that bile leakage is correlated with advanced age, 20 longer operation duration, POPF, PPH,16,21 low levels of serum albumin, wound infections, DGE or sepsis, 20 which are largely consistent with our own report. Meanwhile, while the incidence of bile leakage is notably higher in patients with severe celiac axis stenosis, it is not the exclusive or primary cause of mortality. As a result, there is no statistically significant disparity in mortality rate or the occurrence of complications between the two groups.
Further investigating whether celiac axis stenosis with aberrant hepatic artery increases postoperative complications after LPD, we found that it does not increase the risk of bile leakage or POPF compared with celiac axis stenosis alone. However, regarding POPF, our results are inconsistent with Al-Saeedi’s report, as we did not find that severe celiac axis stenosis increases the incidence of POPF. This may be due to the fact that we had fewer cases with celiac axis stenosis, and we also wrapped the pancreaticoenteric anastomosis with greater omentum tissue during surgery, which helps to reduce the incidence of pancreatic fistula.22,23
Therefore, prior to surgery, it is crucial to thoroughly evaluate the severity and location of stenosis in the celiac trunk, to determine the appropriate treatment measures during the operation. Sugae T et al. classifies celiac axis stenosis into three levels. 12 Level A refers to mild stenosis without collateral circulation formation, which does not require any special treatment during the operation. In level B, collateral pathways only form around the pancreatic head, and it may be necessary to divide the median arcuate ligament. Level C is characterized by a high likelihood of arterial reconstruction or preservation of collateral pathways, as the collateral pathways can form a large arch from the inferior pancreaticoduodenal artery to the gastroduodenal artery. 12 Meanwhile, in some patients with a short distance between stenosis and the celiac trunk, even after the relief of external compression, approximately 20% of patients may not have celiac trunk blood flow restored. 19 Therefore, intraoperative ultrasound evaluation of liver blood flow is crucial. Yamamoto et al. reported a case in which intraoperative ultrasound was used to guide the assessment of a patient with severe celiac axis stenosis undergoing PD without vascular reconstruction. 19 In our center, we have not performed vascular reconstruction on patients with severe stenosis following the relief of external compression; however, two cases developed multiple hepatic abscesses two weeks postsurgery.
This study has several limitations. First, it is a retrospective study with a small size of patients with celiac axis stenosis, therefore, more cases need to be included, and further prospective studies are required to validate the findings. Additionally, the evaluation of the severity of celiac axis stenosis relied on the results of 3D reconstruction, and preoperative angiography was not performed in all patients. Finally, we did not compare the effect of releasing arcuate ligament during surgery on postoperative complications.
Conclusion
Severe celiac axis stenosis is a new independent risk factor for bile leakage following LPD, but it does not increase perioperative mortality.
Footnotes
Acknowledgment
The authors thank Y.H.L., who came up with the idea.
Authors’ Contributions
Conception and design: Y.L. and S.W. Data analysis and interpretation: L.T. and Y.F. Article writing: All authors. Final approval of article: All authors.
Consent for Publication
All authors agreed to publish this article.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.