
Abstract
Background:
Appropriate surgical techniques for controlling bleeding and preserving residual liver function are key to the success of laparoscopic liver resection. This study aims to evaluate the application effect of intraoperative ultrasound in the Pringle maneuver of laparoscopic liver resection.
Materials and Methods:
Between January 2022 and June 2023, 100 patients underwent laparoscopic liver resection and were randomly allocated to receive application of intraoperative ultrasound for Pringle maneuver (intraoperative ultrasound group, n = 50) or conventional Pringle maneuver (conventional group, n = 50). Intraoperative blood loss, blood transfusion, operation time, hepatic portal block time, complications (bile leakage, hemorrhage, ascites, and posthepatectomy liver failure), and hospital stay were compared between groups, along with the alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (TB) levels at postoperative days 1, 3, and 7.
Results:
The operation time, postoperative ALT, AST, and TB levels on postoperative days 1, 3, and 7, complications (bile leakage, hemorrhage, ascites, and posthepatectomy liver failures), and hospital stay were comparable between groups. Compared with the conventional group, the intraoperative ultrasound group had significantly less intraoperative blood loss (P = .015), lower blood transfusion rate (P = .035), and less hepatic portal block time (P = .012).
Conclusions:
Applying intraoperative ultrasound in laparoscopic liver resection for hepatic pedicle occlusion is a safe, simple, and effective method.
Introduction
Laparoscopic hepatectomy holds a significant position in liver surgeries and, just like open hepatectomy, maintaining control of bleeding during liver transection remains a major issue and a primary reason for converting to open surgery.1,2 Research indicates that significant bleeding and subsequent transfusions can notably increase the rates of postoperative complications and mortality, and transfusions also increase the risk of postoperative tumor recurrence in patients.3–6 The Pringle maneuver can reduce the blood flow entering the liver, thereby decreasing intraoperative blood loss and providing a clear surgical field, facilitating the identification of hepatic structures by the surgeon, and promoting safe hepatic parenchymal transection. 7 In clinical practice, many centers have proposed different methods for hepatic pedicle occlusion,8–10 all of which can control intraoperative bleeding effectively, but whether the inflow to the liver is completely blocked is not entirely clear. Onda et al. 11 used the laparoscopic Satinsky vascular clamp for complete control of the hepatic inflow, which was confirmed by intraoperative Doppler ultrasound. We applied intraoperative ultrasound in laparoscopic hepatectomy to ensure that the inflow to the liver was completely blocked by ultrasound probing, thereby reducing the amount of intraoperative blood loss.
Materials and Methods
Patients
Between January 2022 and June 2023, 100 patients who underwent laparoscopic liver resection in the Shaoxing People’s Hospital were selected. The protocol was approved by the local ethics committee, and informed consent was obtained from all patients before being enrolled in the study. These patients with surgically resectable lesions were randomly assigned to undergo laparoscopic liver resection using the application of intraoperative ultrasound for the Pringle maneuver (intraoperative ultrasound group, n = 50) or conventional Pringle maneuver (conventional group, n = 50).
Surgical techniques
In this study, all surgeries were performed by the same highly experienced physician. The liver reserve function was assessed preoperatively using the Child–Pugh score and the ndocyanine green retention at 15 minutes (ICG-R15) test. Preoperative upper abdominal computed tomography (CT) and magnetic resonance imaging (MRI) were performed to fully understand the variations of intra- and extrahepatic ducts and their relationship with the lesion. Both groups of patients were routinely placed in a supine position, intubated, and under general anesthesia, with trocar positions selected based on the surgical site. Adhesions in the abdominal cavity were separated, and the round ligament of the liver was transected. The peritoneal ligaments around the liver were selectively freed depending on where the liver was to be cut, and then the round ligament was lifted upward to expose the porta hepatis. Fluid administration was controlled to lower central venous pressure. A 14-Fr urinary catheter was modified to create a hepatic pedicle clamping device 8 (Fig. 1). The intraoperative ultrasound group used intraoperative Doppler ultrasound to check the blood flow in the hepatic artery and portal vein to ensure complete inflow occlusion to the liver (Figs. 2–4). The conventional group employed hepatic pedicle clamping based on the surgeon’s experience. After clamping the hepatic pedicle, the liver parenchyma was dissected. The lead surgeon performed “small step fast cut” techniques with the ultrasonic scalpel to dissect the superficial liver tissue. The assistant helped to retract the liver, allowing the liver-cut surface to open like “flipping through a book,” keeping a certain tension in the liver tissues on both sides. When encountering vascular structures during liver dissection, each was severed using titanium clips, Hem-o-lok ligation clips, or laparoscopic Endo-GIA, with suturing using 4-0 or 5-0 prolene thread when necessary until the specimen was completely removed. Each hepatic pedicle clamping lasted no longer than 15 minutes, with an interval of 5 minutes. In cases with cirrhosis, the clamping time needed to be appropriately shortened and the interval time extended. After specimen removal, thorough electrocoagulation was used for hemostasis of the liver-cut surface. If hemostasis was uncertain, suturing was done using 3-0 or 4-0 prolene thread. The liver-cut surface and abdominal cavity were repeatedly rinsed with saline to exclude active bleeding and bile leakage. A multichannel drain was placed on the liver-cut surface and through the lesser omentum hole. The incisions were sutured one by one, and the drainage tube was secured, concluding the surgery.
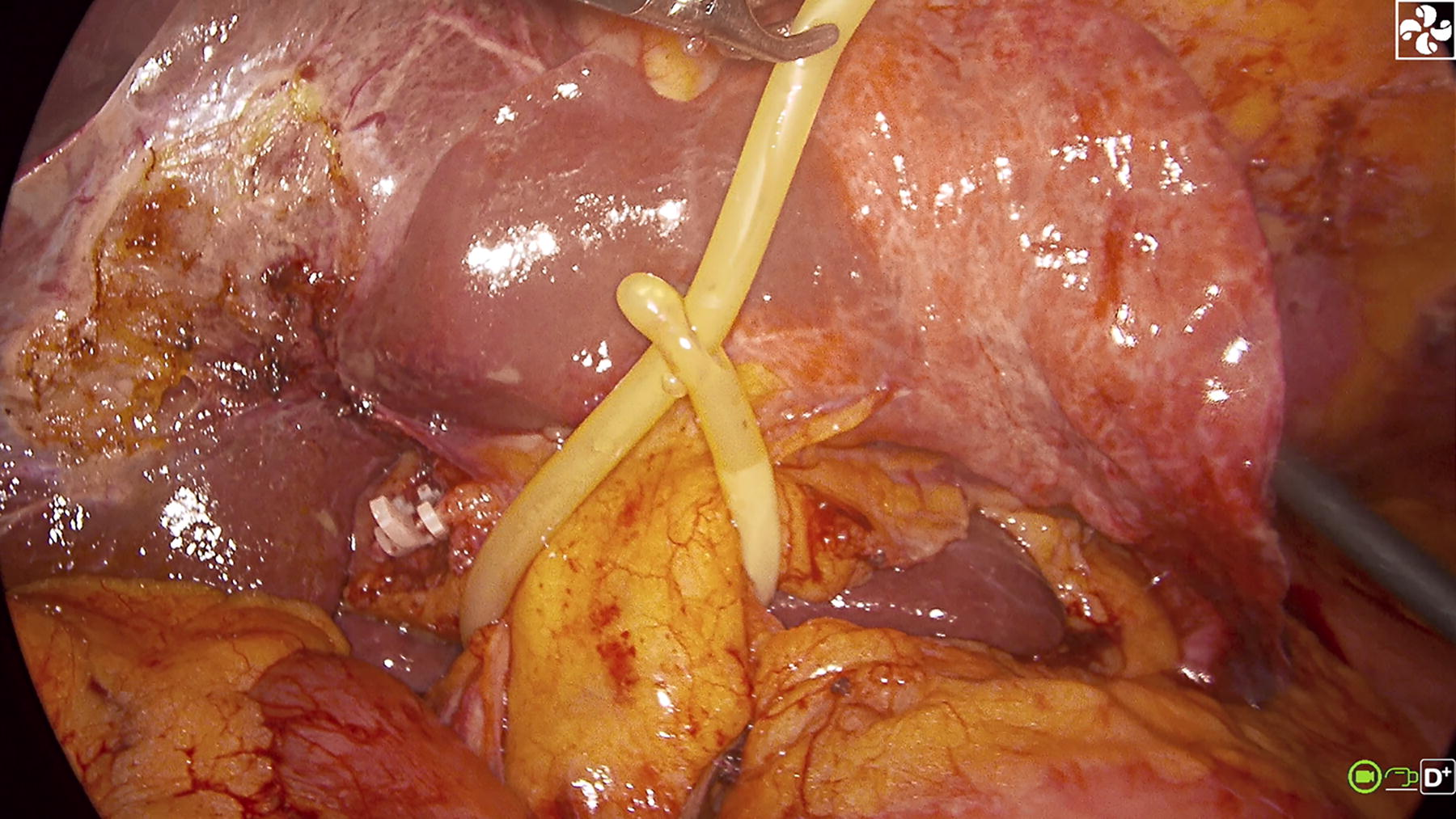
Clamping the hepatic pedicle with a modified 14 Fr catheter.
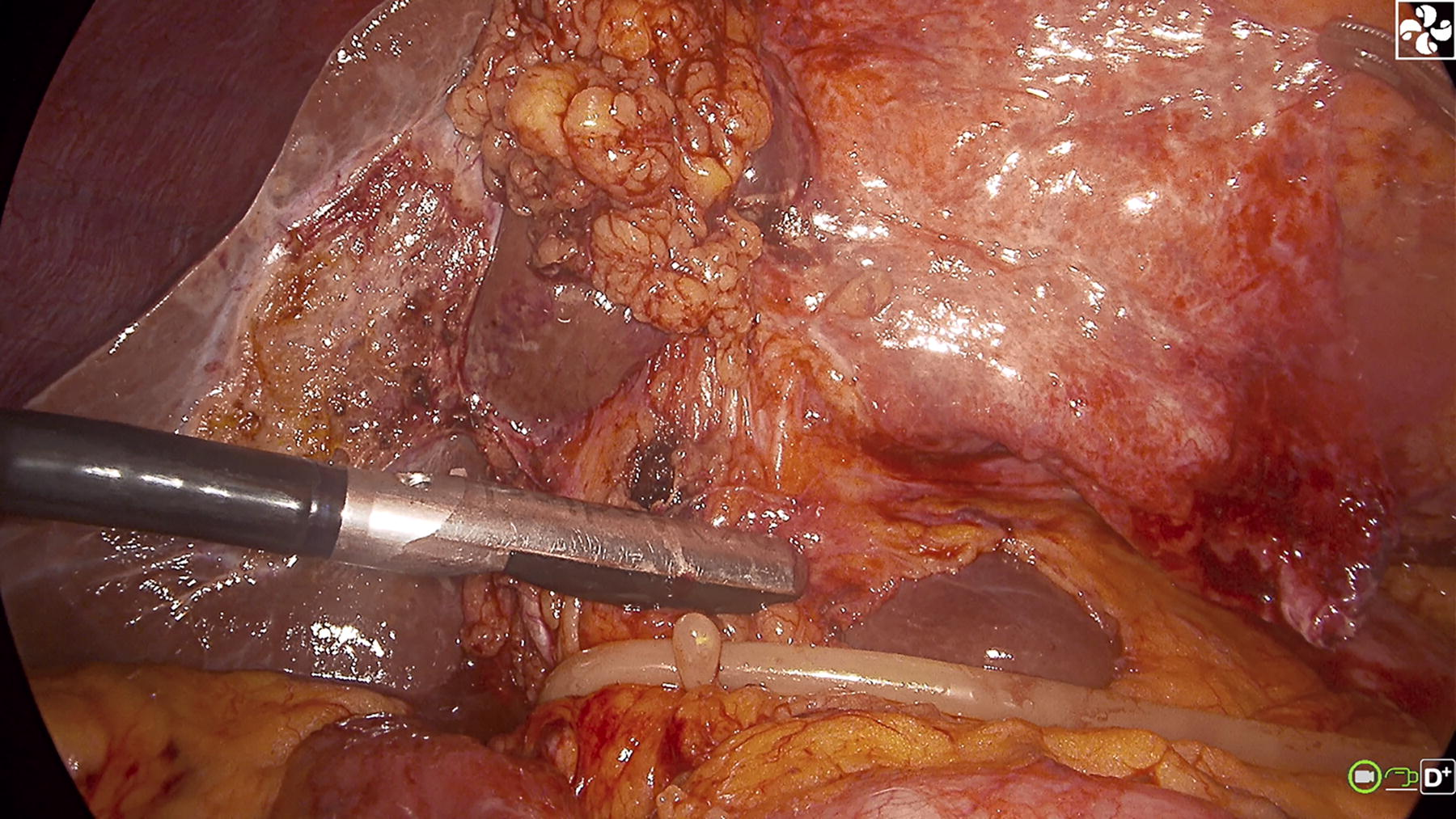
Intraoperative Doppler ultrasound detection of blood flow in the hepatic artery and portal vein.

Doppler ultrasound before hepatic pedicle occlusion.
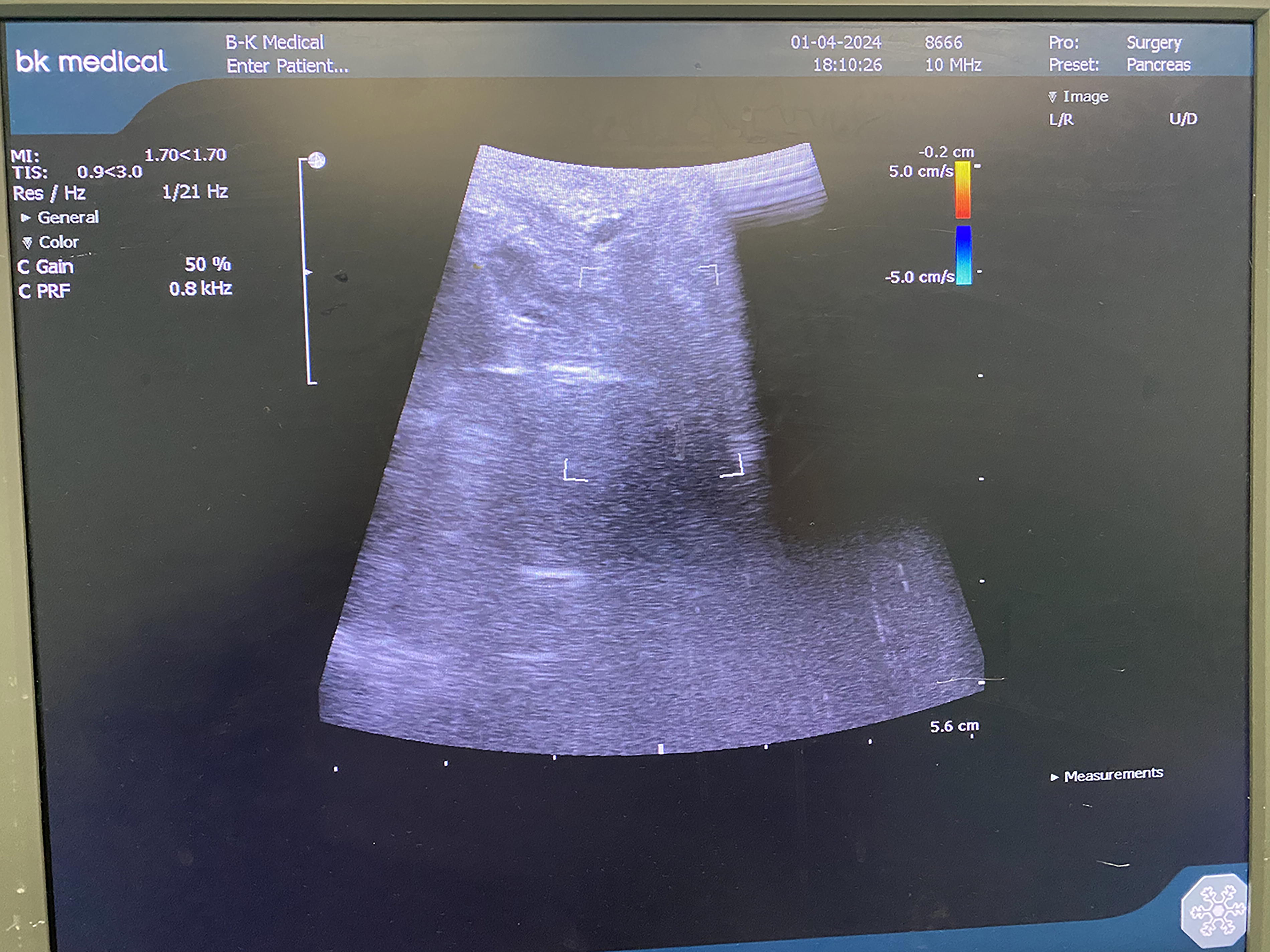
Doppler ultrasound after hepatic pedicle occlusion.
Measurements
All demographic and clinical data were retrieved from medical records. Clinical parameters that were evaluated included age, sex, body mass index (BMI), the severity of cirrhosis, range of hepatic resection, the Child–Pugh classification, and pathological classification. Liver function was monitored by serum levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (TB) at postoperative days 1, 3, and 7. Intraoperative parameters, including blood loss volume, rate of blood transfusion, operation time, and hepatic portal block time, as well as postoperative parameters, including major complications (bile leakage, hemorrhage, ascites, and posthepatectomy liver failure) and length of hospital stay, were analyzed.
Statistical analyses
Numerical data were expressed as mean–standard deviation if normally distributed. Group differences were compared using Student’s t-test or analysis of variance for numerical data following a normal distribution as appropriate. Categorical data were compared with Pearson’s chi-square test. A two-sided P <. 05 was taken as statistically significant. SPSS version 18.0 (SPSS, Inc., Chicago, IL) was used for statistical analyses.
Definitions
Operative time was calculated as the time from the skin incision to the entire skin closure. Blood loss was recorded carefully by the anesthetist through a postoperative complications vacuum system. Length of stay was defined as the days from admission to discharge. Bile leakage 12 was defined by an international study group of liver surgery as bilirubin concentration in the drain fluid at least thrice the serum bilirubin concentration on or after postoperative day 3 or as the need for radiological or operative intervention resulting from biliary collections or bile peritonitis. Posthepatectomy hemorrhage 13 is defined as a drop of hemoglobin level >3 g/dL after the end of surgery compared to postoperative baseline level and/or any postoperative transfusion of packed red blood cells for a falling hemoglobin and/or the need for invasive reintervention (e.g., embolization or relaparotomy) to stop bleeding; postoperative ascites 14 was defined as daily ascite fluid drainage exceeding 500 mL and/or grade 2 ascites in ultrasonography, computed tomography, or clinical assessment showing a moderately symmetrical distension of the abdomen.
Results
No significant differences were observed in age, gender, and BMI between the intraoperative ultrasound group and the conventional group (Table 1). The number of patients with liver cirrhosis, range of hepatic resection, Child–Pugh scores, and pathological classifications were very close between the intraoperative ultrasound group and the conventional group, and these differences were not statistically significant.
Clinical Characteristics of Patients Allocated to the Intraoperative Ultrasound Group and Conventional Group for Laparoscopic Liver Resection
ICC, intrahepatic cholangiocarcinoma; HCC, hepatocellular carcinoma; SD, standard deviation .
As shown in Table 2, the average operation time of the intraoperative ultrasound group was comparable to the conventional group, but the hepatic portal block time of the intraoperative ultrasound group (30.60 ± 11.21 minutes) was significantly less than that of the conventional group (36.90 ± 13.15 minutes, P = .012). The intraoperative blood loss in the intraoperative ultrasound group (102.40 ± 77.05 mL) was significantly less than that in the conventional group (153.00 ± 121.30 mL, P = .015). Only 26% of the patients in the intraoperative ultrasound group required intraoperative blood transfusion, which was significantly lower than 46% in the conventional group (P < .05).
Intraoperative Outcomes of Patients Allocated to the Intraoperative Ultrasound Group and Conventional Group for Laparoscopic Liver Resection
Liver function before and after the surgery was compared, such as levels of ALT, AST, and TB (Table 3). There were no significant differences in preoperative serum ALT, AST, and TB levels between the intraoperative ultrasound group and the conventional group. On postoperative days 1, 3, and 7, the postoperative serum ALT and AST levels in the intraoperative ultrasound group were slightly lower than those in the conventional group, but not significantly. The levels of ALT, AST, and TB in both groups were significantly elevated temporarily after the surgery and then gradually returned to near preoperative levels by the 7th postoperative day, but they were still significantly higher than the preoperative levels.
Preoperative and Postoperative Serum Levels of Alanine Aminotransferase, Aspartate Aminotransferase, and Total Bilirubin in Patients Allocated to the Intraoperative Ultrasound Group and Conventional Group for Laparoscopic Liver Resection
Postop, postoperative.
Two patients (4%) in each group experienced bile leakage, and there was no difference in the incidence of this complication between the two groups (Table 4). Both groups had similar postoperative hemorrhage complication rates. The conventional group had a slightly higher number of patients with postoperative ascites compared to the intraoperative ultrasound group, but the difference was not significant (36% versus 30%, P = .523). Neither group experienced posthepatectomy liver failure. Therefore, the hospital stay for patients in both groups was close.
Complications and Outcomes in Patients Allocated to the Intraoperative Ultrasound Group and Conventional Group for Laparoscopic Liver Resection
Discussion
It is well known that hepatic blood flow occlusion mainly includes two categories: inflow occlusion and total hepatic blood flow occlusion. The former can be further divided into continuous complete inflow occlusion, intermittent complete inflow occlusion, hemihepatic flow occlusion, and segmental flow occlusion. The latter includes total hepatic flow occlusion, selective hepatic flow occlusion, or the so-called liver blood flow occlusion preserving the vena cava. 15 Clinically, inflow occlusion is generally preferable, such as selective hemihepatic flow occlusion.16,17 The authors believe that selective hemihepatic flow occlusion can reduce intraoperative bleeding, mitigate liver function damage, and lower the incidence of postoperative complications and mortality. Glissonian pedicle transection for liver resection was first proposed and applied to open liver resection by Japanese scholar Takasaki. 18 Ke et al. 19 believe that Glissonean pedicle transection with hepatic vein exclusion is a safe, simple, and effective procedure for hepatic resection. Although various new methods of liver blood flow occlusion are emerging, the Pringle maneuver remains the most commonly used method for hepatic blood flow occlusion. A review 7 summarized three common Pringle maneuver techniques: (1) the Rummel-tourniquet technique, (2) vascular clamp use, and (3) the Huang loop technique. The authors prefer the modified Huang loop technique because it is inexpensive, reliable, and quick to apply or release.
The results of our study reveal that compared to the conventional group, the intraoperative ultrasound group experienced less bleeding, required fewer intraoperative blood transfusions, and had a less hepatic portal block time (all P < .05), while there was no significant difference in operation time, liver function on days 1, 3, and 7 after surgery, the incidence of postoperative complications, or postoperative hospital stay (all P > .05) between the two groups. This indicates that the use of intraoperative ultrasound in the application of hepatic pedicle occlusion during laparoscopic liver resection ensures complete occlusion of the hepatic pedicle, thereby reducing intraoperative blood loss and blood transfusion quantity. Although the intraoperative ultrasound group required additional steps such as ultrasound scanning and multiple tightens of the hepatic pedicle occlusion band, we found this did not increase the total operation time. We had the assistants tighten the hepatic pedicle occlusion band through two operating ports, while the primary surgeon performed the ultrasound scan through the main operating port and adjusted the pressure of the occlusion band according to the scanning results. Once we mastered the technique of intraoperative ultrasound scanning, this step became very simple. The hepatoduodenal ligament is exposed, and one only needs to place the ultrasound probe closely against it to scan the internal vessels. Moreover, we only need to judge the presence or absence of blood flow in the vessel to confirm the complete occlusion of the hepatic pedicle. The intraoperative ultrasound group ensured a completely occluded hepatic pedicle, thus reducing bleeding at the liver-cut surface and providing a clear field of vision for the surgeon. The surgeon could safely complete the operation within a shorter duration of hepatic pedicle occlusion.
For half-liver inflow occlusion, although the ischemia–reperfusion injury (IRI) and complications16,20 are reduced, a large amount of bleeding from the unoccluded side of the liver occurs during liver transection, especially in patients with cirrhosis who have more collateral bleeding.21,22 Some surgeons believe that there is no need for complete hepatic pedicle occlusion during laparoscopic liver resection, as controlling occlusion pressure can ensure complete portal vein flow occlusion while allowing hepatic artery blood flow. They believe that this can reduce IRI in liver tissue and allow a single occlusion time to extend beyond 15 minutes. We do not agree with this view. Since the purpose of the hepatic pedicle occlusion is to reduce bleeding, keep the surgical field clear, and avoid damage to important vessels, we should completely occlude the hepatic inflow. What we need to do is to perform a rigorous preoperative liver function evaluation, such as liver function tests, three-dimensional liver residual volume calculation, and ICG-R15 testing. At the same time, strictly adhere to the “15-5-15” occlusion time interval which has been verified countless times. 23 After all, the hepatic pedicle occlusion can only control the inflow to the liver, and it does not have much effect on bleeding originating from the hepatic veins. Therefore, low central venous pressure during surgery is also a necessary measure to reduce intraoperative bleeding. 24
Surgeons often only focus on whether the inflow to the liver is completely occluded and whether the surgical cut surface is bleeding, rarely paying attention to whether the pressure of occlusion is too high. Excessive occlusion pressure can easily damage vessels and bile ducts within the hepatoduodenal ligament and might even lead to long-term complications such as vascular intima injury 11 or common bile duct stricture. Cai et al. used an elasticated cuff from a surgical glove to occlude hepatic inflow, admitting they did not apply intraoperative ultrasound to confirm complete occlusion of hepatic blood flow. 9 We tried this method and found that ordinary tightening force could not completely occlude hepatic vessels. With increasing force, the thin glove belt can easily cut tissues, thereby damaging tissues within the hepatoduodenal ligament. The Huang’s loop is thicker, reducing the risk of damaging tissues within the hepatoduodenal ligament. When the intraoperative ultrasound confirms complete occlusion of hepatic blood flow, the pressure at that time has reached an effective occlusion pressure. Any increase in pressure above the effective occlusion pressure is meaningless, and excessive occlusion pressure will only cause unnecessary collateral damage. Under intraoperative ultrasound monitoring, we continuously and slowly increase the occlusion pressure, and once complete occlusion of the hepatic inflow is achieved, we no longer increase the pressure. This ensures that we can successfully complete the operation without increasing collateral damage while maintaining the effective occlusion pressure.
In this study, neither of the two methods of hepatic hilar occlusion induced acute liver failure, and there were no significant differences observed in the rates of postoperative complications or length of hospital stay. Thus, it can be inferred that different occlusion methods have no significant impact on postoperative recovery in patients under appropriate postoperative hepatic care.
In summary, we believe that the application of intraoperative ultrasound in hepatic pedicle occlusion during laparoscopic liver resection can ensure complete occlusion of the inflow to the liver and provide a clear surgical field, facilitating precise surgical maneuvers. It has the advantages of less bleeding, less blood transfusion, and less hepatic portal block time without increasing the duration of the surgery, damaging postoperative liver function, or the incidence of postoperative complications. Based on this research, we are further able to study the pressure type of occlusion bands, digitize the occlusion pressure, and allow the occlusion pressure to change with changes in arterial pressure, dynamically maintaining an effective occlusive pressure. By precisely controlling the occlusion pressure, we can ensure the occlusion effect while minimizing collateral damage to the tissues within the hepatoduodenal ligament.
Footnotes
Acknowledgments
B.L. would extend his sincere gratitude to Kangze Wu for his valuable suggestions and inspiring advice on the article. Special thanks should go to my beloved wife and my parents for their continuous support and encouragement.
Authors’ Contributions
X.G. formed the concept, designed the trial, and wrote and drafted the protocol. T.H.J. designed the statistical plan for the trial. L.B.C. made substantial contributions to the trial design and critically revised the protocol. All authors have read and approved the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
The work was sponsored by Zhejiang Provincial Medical and Health Science and Technology Projects under grant no.