
Abstract
Background:
The gastric neuroendocrine tumor (g-NET) is now more frequently diagnosed due to the widespread use and advancement of endoscopy. In our study, we aimed to discuss the superiority, if any, between the watch-and-wait approach and endoscopic treatment methods for the controversial management of type 1 g-NETs, as well as to evaluate their long-term outcomes.
Materials and Methods:
The data of 81 patients who underwent gastroscopy due to complaints related to the upper gastrointestinal system and were diagnosed with type 1 g-NET as a result of biopsy taken from suspicious stomach lesions were examined. After exclusion criteria, 48 patients were included in the study. Patients were categorized into two groups: the watch-and-wait group, where no invasive procedure was performed, and the group that underwent any form of endoscopic resection.
Results:
Thirty-seven patients were followed up regularly without any treatment. Eleven patients were followed up after endoscopic resection (endoscopic submucosal dissection–endoscopic mucosal resection). Endoscopic resection was performed in 5 of 37 patients with tumor size <10 mm and in 6 of 11 patients with tumor size between 10 and 20 mm. The median follow-up duration for all patients was 5 years, during which no instances of metastasis, tumor progression, or mortality were observed in any patient, regardless of whether they underwent endoscopic resection or not.
Conclusion:
This outcome prompts a questioning of the necessity for invasive treatment methods such as endoscopic resection, which comes with a relatively high cost and the potential for complications, in this particular patient group.
Introduction
Gastric neuroendocrine tumors (g-NETs) are neoplasms that originate from enterochromaffin-like cells of the gastric mucosa. 1 They are rare lesions showing nonaggressive behavior and neuroendocrine differentiation, constituting <1% of all gastric neoplasms. 2 The widespread use of upper gastrointestinal endoscopy and the technical advancements among endoscopists have led to an increased diagnosis of these lesions.1,3–5
A study dated 2015 incorporating national records from several countries reported a prevalence rate of g-NETs per 10,000 individuals: 0.32 in Europe, 0.17 in the United States, and 0.05 in Japan. 6 G-NETs are categorized into three groups with different biological behaviors and prognoses.7,8 Type 1 tumors constitute 70%–80% of all usually smaller than 1 cm, often appearing as multiple small polypoid lesions with a small central ulceration and secreting gastrin. Type 2 and type 3 gastric tumors, although less common, present distinct characteristics. Type 2 tumors are smaller in size and are frequently associated with MEN1 or gastrinoma. Conversely, type 3 tumors are larger and typically do not secrete gastrin.8–10 Type 1 tumors present various treatment options, both invasive and noninvasive. However, the role of medical treatment (such as dietary modifications, acidification maneuvers like diluted oral hydrochloric acid, or somatostatin analog [SSA] therapy for antigastrin effects) is debated over surgical intervention.11–14 Regardless of gastrin levels, patients require endoscopic surveillance.
In this study, we aimed to discuss whether there is a superiority between the watch-and-wait approach and endoscopic treatment methods for the controversial management of type 1 (g-NETs) and to evaluate their long-term outcomes.
Materials and Methods
The study, conducted retrospectively, commenced following approval from the local ethics committee. The data of 81 patients diagnosed with type 1 g-NET based on biopsy samples taken from lesions identified endoscopically at XXX Education and Research Hospital between January 1, 2011, and April 1, 2019, were analyzed via the computer system. Exclusion criteria for the study were defined as having an additional history of malignancy, lack of regular follow-up, death due to unrelated causes, and incomplete computerized data. After exclusion criteria, 48 patients were included in the study. Patients were divided into two groups: the “watch-and-wait” group, utilizing only proton pump inhibitors without invasive intervention, and the endoscopic treatment group, which underwent either endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). Patients’ ages, genders, tumor localization and sizes at the time of diagnosis, Ki-67 indices, mitotic rates in biopsy samples, positron emission tomography (PET) results, follow-up endoscopies, and endoscopic pathology results were examined. During the follow-up, the progression of patients’ tumors and the development of recurrence in those who underwent resection were monitored.
Statistical analysis
SPSS 26.0 for Windows program was used for statistical analysis. Descriptive statistics: numbers and percentages for categorical variables, mean, standard deviation, median, minimum, and maximum for numerical variables were given. Comparisons of numerical variables in two independent groups were made with Student’s t-test for the variable satisfying the normal distribution condition, and with the Mann–Whitney U test when the normal distribution condition was not met. A chi-square test was used to analyze the ratios in the groups. The statistical alpha significance level was accepted as P < .05.
Results
The study encompassed 48 patients meeting the inclusion criteria following the application of the specified exclusion criteria (Fig. 1). Of these patients, 26 were male and 22 were female, with a mean age of 55.2 ± 14.8. Upon reviewing indications for gastroscopy in patients, it was determined that the most common reason, observed in 41 patients (85.4%), was upper gastrointestinal symptoms associated with dyspeptic complaints. The corpus of the stomach was identified as the most frequent site for g-NET detection in 70.8% of patients. Multiple tumoral foci were present in 60.4% of patients. Calculation based on the largest tumor diameter among patients with multiple tumoral foci revealed an average tumor size of 6.2 × 3.8 mm for all included patients. Histopathological examination of biopsy samples showed a mitotic index of 0/10 in 46 patients and 1/10 in 2 patients, whereas the Ki-67 index was found to be <3% in 93.8% of patients. T1 tumors were identified in 46 patients (95.83%), whereas T2 tumors were observed in 2 patients (4.17%). The mean follow-up duration for patients included in the study was determined as 5.8 years (Table 1). Among the 37 patients with tumor sizes below 10 mm, FDG uptake was observed in 2 patients (5.40%), while among the 11 patients with tumor sizes ranging from 1 to 2 cm, 6 patients (54.54%) showed FDG uptake on PET imaging, indicating a statistically significant difference (P = .001). Endoscopic resection was performed in 5 out of the 37 patients with tumor sizes below 10 mm (refer to Table 1). In the “watch-and-wait” group, 37 patients (77.1%) solely used proton pump inhibitors, whereas in the endoscopic resection group, 11 patients (22.9%) underwent either EMR or ESD. A comparison of the parameters between the groups showed that ESD–EMR was significantly more preferred than “watch and wait” in tumors sized 1–2 cm (Table 2). No cases of endoscopic resection-related perforation or major bleeding were detected in any patient who underwent EMR or ESD. During gastroscopic assessments conducted every 3–6 months and abdominal computed tomography (CT) or PET-CT scans performed every 1–2 years, no instances of metastasis or tumor progression were observed in any of the patients.
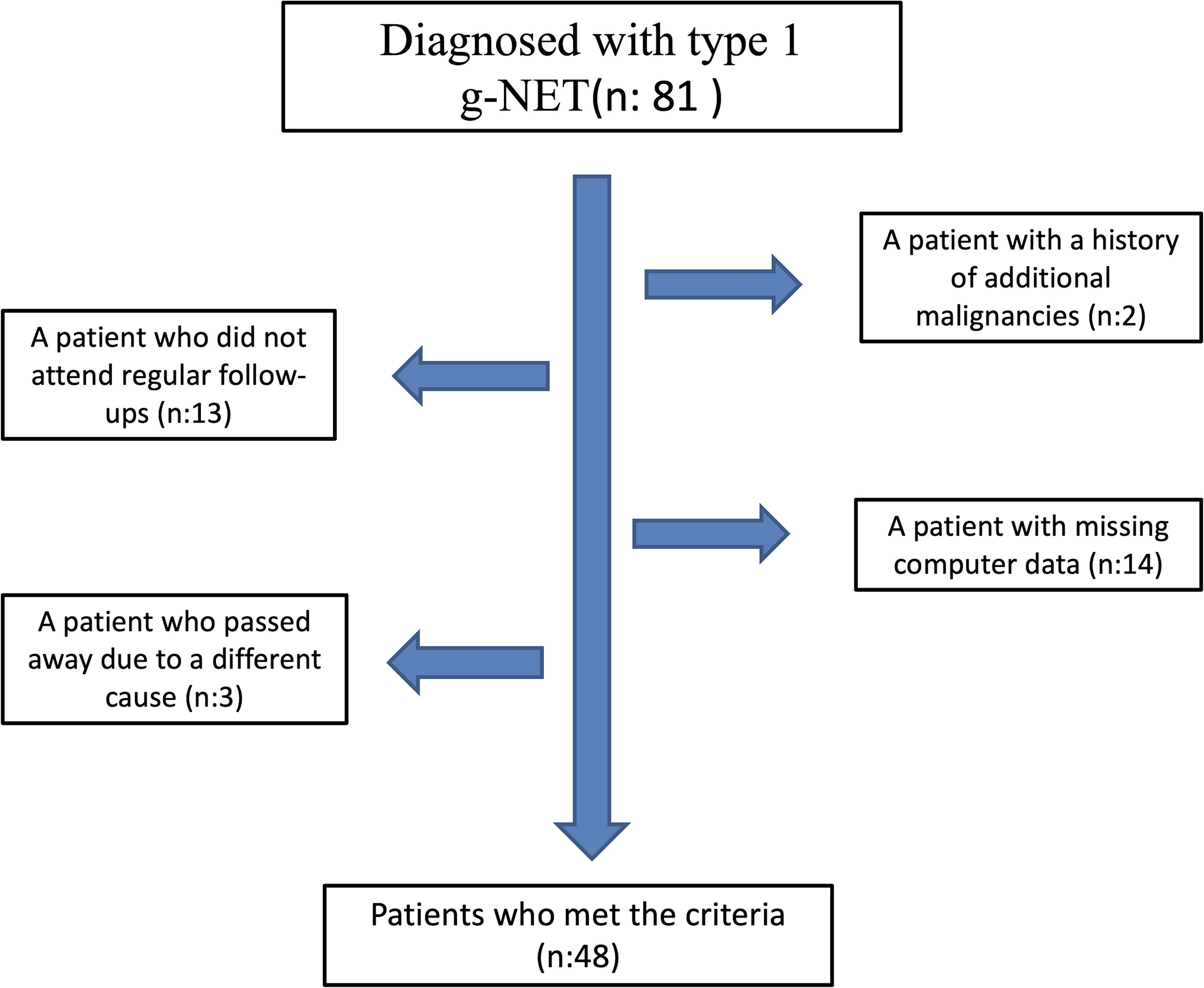
A flowchart for patient selection.
Patient and Tumor Characteristics
IQR, interquartile range; EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection; SD, standard deviation.
The Comparison Between the Group of Patients Treated with ESD–EMR and the Group Managed with a “Watch-and-Wait” Approach
EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection; SD, standard deviation.
Discussion
The timing for the indication of surgery in patients with type 1 g-NETs remains unclear. There is no consensus in the literature regarding resection versus watch and wait. The only recognized risk factor for the progression of type 1 g-NETs is the size of the tumor. The European Neuroendocrine Tumor Society (ENETS) has set the reference size at 10 mm for intervention. Most centers advocate for conservative treatment approaches involving endoscopic surveillance and/or endoscopic resection in patients. While some authors propose the resection of all visible lesions, others have suggested establishing a size threshold for this intervention.15,16 In our study, among patients with type 1 g-NETs who underwent a watch-and-wait approach, a lengthy follow-up averaging around 5 years did not reveal any instances of progression or metastasis. Similar to several previous studies, our research also found upper gastrointestinal symptoms generally present in patients.8,12,17 While studies often indicate a predominance of females, our research observed a higher number of male participants.18,19 However, we believe that gender may not play an influential role in type 1 neuroendocrine tumor diagnoses. Various methods have been historically utilized in the treatment of patients with type 1 g-NET. One such method is antrectomy, although it remains a contentious option for type 1 g-NETs. Antrectomy reduces hypergastrinemia by diminishing the mass of cells producing gastrin in the antrum of the stomach; in most cases, this leads to tumor regression. 8 In a study analyzing 51 patients with type 1 neuroendocrine tumors, antrectomy was performed on 10 patients. Among these cases, 9 patients treated with antrectomy remained tumor-free during long-term follow-ups, while tumor progression was observed in 1 patient. It has been evidenced that antrectomy is effective in preventing tumor recurrence in the majority of cases. 8 Furthermore, a study revealed that performing antrectomy required fewer endoscopies during follow-up, reduced the risk of recurrence, and could alleviate concerns about malignant development in patients. 20 However, it should be noted that in particular cases involving multifocal disease, surgical resection, including antrectomy, may extend to total gastrectomy, thereby increasing mortality and morbidity, a consideration that needs to be kept in mind. Another option used in the treatment of type 1 g-NETs, less invasive than antrectomy, is endoscopic resection. Endoscopic resection is considered a curative treatment modality for limited tumors in the mucosa and submucosa. There are two distinct methods of endoscopic resection: EMR and ESD. Endoscopic resection can be performed using biopsy forceps, EMR, ESD, and argon plasma coagulation,21–23 representing a less invasive method compared with surgical treatments but with various associated complications. When reviewing the EMR and ESD series, the most commonly observed complications are bleeding and perforation. 24 In a study conducted by Jin Hee Noh et al., 23 103 patients diagnosed with type 1 g-NETs were followed after undergoing EMR in 62 cases and ESD in 41 cases. Throughout a 63-month follow-up period for both resection methods, the local recurrence rates were 6.5% for EMR and 2.4% for ESD groups. No mortality was observed among the patients. Four patients underwent wedge resection, and 1 patient underwent total gastrectomy. No superiority was detected between ESD and EMR. Based on the positive long-term outcomes observed in this study, endoscopic resection was considered an effective and safe treatment strategy for type 1 neuroendocrine tumors. However, no patients were followed without resection, either endoscopically or surgically. Another study involving 22 patients who underwent EMR for type 1 neuroendocrine tumors found that among these patients, 4 had polyp sizes >1 cm, while 18 had sizes ranging between 0.5 and 1 cm. Recurrence was observed in 4 patients, and 1 patient experienced perforation due to resection. Throughout long-term follow-up, no mortality or local/systemic metastasis was detected among any of the patients. 16
In cases of type 1 g-NET, SSAs can sometimes be used to suppress gastrin levels. SSAs offer the advantage of tumor regression; however, they have not been compared with other treatment strategies and have not gained widespread acceptance for routine use. SSAs may be beneficial for multiple small lesions that are not amenable to endoscopic resection. 25 In several studies, it has been considered that both gastrectomy and SSAs could be used to reduce serum gastrin and tumor control when lesions are numerous, impossible to remove endoscopically, or when there are recurrences following endoscopic treatment.25,26 Klaire Exarchou et al. 27 conducted a study involving 87 patients diagnosed with type 1 g-NETs who underwent only endoscopic follow-up without resection. Throughout an average follow-up period of 62 months, tumor size remained below 1 cm in 75 patients, and no progression was observed in any of these cases. Among the 12 patients monitored within the 1–2 cm range, progression requiring a change in treatment management was detected in only 2 patients.
Our study has several limitations. These include the retrospective nature of the study and variability in the choice of resection among cases dependent on the endoscopist. Additionally, the small sample size (n = 48) may limit the generalizability of our findings. Moreover, the absence of standardized blood sampling for both gastrin and chromogranin A levels restricts the robustness of our conclusions. This precludes to make stronger conclusions on this topic. Future studies should aim to include larger sample sizes and incorporate routine measurements of these biomarkers to provide more definitive insights into the management of type 1 g-NETs.
Conclusion
In conclusion, treatments for patients with type 1 g-NET exhibit low recurrence, progression, and metastasis rates across various methods; however, invasive treatment methods particularly bring along various complications. Although definitive boundaries for each treatment method are not clearly defined, they necessitate periodic follow-ups. In our study, regardless of whether endoscopic resection was performed or not, no progression or metastasis was observed in any patient during a median 5-year follow-up period. Especially in patients with g-NETs smaller than 10 mm, constituting the majority of our cohort, a “watch-and-wait” approach appears suitable as a primary intervention. For patients with tumor sizes between 1 and 2 cm, further studies investigating only endoscopic surveillance versus resection are warranted.
Footnotes
Authors’ Contributions
Critical review: C.T. and U.O.I. Study concepts and design: O.A. and U.O.I. Literature research: O.A., Y.C.A., U.O.I., and H.S. Clinical studies: O.A., M.G., H.S., and C.T. Data collection and analysis: O.A., Y.C.A., M.G., and C.T. Statistical analysis: O.A., M.G., C.T., and H.S. Writing article: O.A. and C.T. Final approval of the article: O.A., M.G., H.S., Y.C.A., U.O.I., and C.T.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement
All of the authors reported no biomedical financial interests or potential conflicts of interest. There is no organization or person that funded our study.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.