
Abstract
Background:
Single-incision laparoscopic cholecystectomy (SILC) is a minimally invasive procedure designed to minimize the number and size of the incisions needed for cholecystectomy. Titanium clips are traditionally used to close the cystic duct and artery. Although it is considered safe, dislodgement can result in bleeding and biliary leakage. Using LigaSure for duct sealing is still controversial. The aim of this study was to evaluate the safety and feasibility of using LigaSure to close the cystic duct during SILC.
Methods:
A prospective study over two years was conducted at the General Surgery Department, Mansoura University Hospital, on 102 patients, 51 in each group. They underwent SILC using LigaSure (Group 1) or titanium clips (Group 2) to control the cystic duct and artery.
Results:
The data analyzed included demographic data, operative time, intra- and postoperative complications, postoperative pain, and hospital stay. The operative time was significantly shorter in LigaSure group (68.5 ± 9.8 versus 72.9 ± 10.6 minutes in the clips group, P .03). There was no significant difference between the two groups regarding postoperative bile leak or bleeding. However, two cases in Group 1 and four cases in Group 2 were converted to multiple port laparoscopic cholecystectomy; this was statistically nonsignificant. Postoperative pain and hospital stay showed no significant difference between the two groups. Two patients in each group developed port-site incisional hernia.
Conclusions:
Clipless SILC using LigaSure is a feasible and safe procedure with acceptable morbidity with shorter operative time than SILC using clips. Nevertheless, the risk of port-site incisional hernia should be explained to the patients.
Introduction
Eric Muhe performed the first laparoscopic cholecystectomy (LC) in 1985, 1 and now it is the most commonly performed laparoscopic surgical operation and the gold standard treatment for benign gallbladder diseases. 2
Three or four ports are used during conventional laparoscopic cholecystectomy (CLC), through which a camera and instruments gain entry. CLC is associated with postoperative port site pain and a wound infection risk of 1.3% to 3.5%.3,4
In recent years, several new techniques have been developed to reduce the number and size of incisions, postoperative pain, wound infection, recovery time, and improve cosmesis.4–7
Single-incision laparoscopic cholecystectomy (SILC) is one of these techniques; it was first performed in 1997 by Navarra et al. 8 In SILC, the procedure is carried out with a single umbilical incision by inserting the laparoscope and instruments through a special access device.
Advantages of SILC include decreased postoperative pain, better cosmesis with virtually scarless surgery because the scar is concealed within the umbilicus, and quicker recovery. 9
In contrast, SILC led to instrument crowding, their crossover, and a lack of triangulation, which led to prolonged operative time and an increased workload on surgeons. In addition, it is associated with higher rates of incisional hernia (13.3% versus 4.7%).6,9–12
Recently, specially designed ports, articulating instruments, and improved optics have facilitated SILC. 13
In CLC, titanium clips are used to seal the cystic duct and artery before their division. Even though it is considered safe to place these clips to seal the cystic duct and artery, slippage of the clips may occur, leading to biliary leakage and bleeding, and these clips may also result in strictures due to foreign body reaction, migrate into adjacent structures, and act as a nidus for formation of stones.14,15
Vessel sealing devices (Harmonic™, LigaSure™, etc.) were created to seal, coagulate, and cut blood vessels during laparoscopic surgery. These devices gained popularity in laparoscopic surgery due to the difficulty of using the traditional surgical hemostasis techniques laparoscopically.16–18
The safety and feasibility of using vessel sealing devices for duct sealing during SILC, especially LigaSure, are still controversial.19–22
The advantages of LigaSure are minimal risk of injury to the nearby structures because of the computer guided bipolar cautery, and no metallic clips will be left in the body, consequently preventing clip related complications like slippage and migration.
The aim of this study was to assess the safety and feasibility of using LigaSure for cystic duct closure during clipless SILC.
Patients and Methods
This prospective randomized clinical study was conducted at the Department of General Surgery, Mansoura University Hospital, between March 2018 and March 2020. SILC was offered to patients with symptomatic gallbladder stones as an elective operation with a detailed explanation of the procedure, including the possibility to convert to CLC or open technique. This study included 102 patients after fully informed written consent, and Mansoura Faculty of Medicine Institutional Review Board (approval number: MS/17.03.02) approved the study.
The inclusion criteria included patients with symptomatic gall stones aged between 18 and 70 years, a body mass index (BMI) <35 kg/m2, and an American Society of Anesthesiology (ASA) score of 1–3. Patients with acute cholecystitis, a history of gallstone complications (cholangitis, choledocholithiasis, jaundice, and pancreatitis), patients with liver cirrhosis, pregnant females, previous upper abdominal surgery, uncontrollable coagulopathy, and an ASA score of 4 or 5 were excluded.
Patients were subjected to preoperative evaluation by clinical examination, routine laboratory investigations, and abdominal ultrasound.
Eligible patients were randomly (1:1) assigned by the closed envelope method of randomization into two groups, Group 1: SILC with LigaSure™ for closure of the cystic artery and duct (n = 51); and Group 2: SILC with conventional closure of the cystic artery and duct with titanium clips (n = 51). One dose of preoperative antibiotic was given to each case (Ceftriaxone 1 gm, IV) at the induction of anesthesia.
Surgical technique
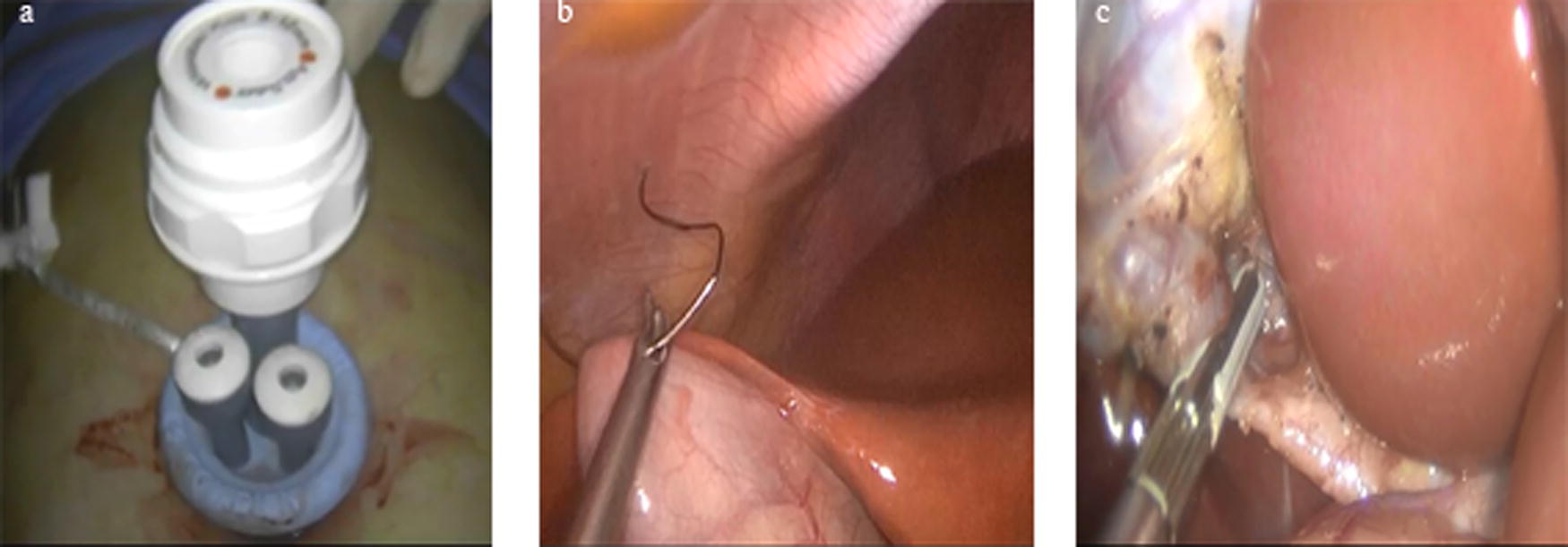
The same surgical team performed the procedure to all of the patients. Under general anesthesia, the patients were placed in lithotomy position with anti-Trendelenburg and left lateral tilt. The surgeon stood in between the patient’s legs. A single 2–2.5 cm transumbilical incision was made, a mini-laparotomy was performed, and the peritoneal cavity was visualized, then the SILS port (Covidien, Inc., Norwalk, USA) was inserted (Fig. 1a), and the pneumoperitoneum was established with CO2 at a pressure of 14 mmHg. The gallbladder fundus was retracted ventrally by a transabdominal suture with Vicryl 0 (Fig. 1b). Then laparoscopic cholecystectomy was carried out like conventional four port laparoscopic cholecystectomy, and articulating laparoscopic instruments were used.
Clipless SILC.
In Group 1, 5-mm LigaSure™ (Valleylab, Boulder, Colorado, USA) was applied to seal and divide the cystic duct at least 3 mm from the common bile duct (Fig. 1c), and then the cystic artery was also sealed and divided separately. In Group 2, each of the cystic duct and artery were closed using 3 titanium clips, divided in such a way that 2 clips were left in the residual stump of cystic duct and artery. The medium-large (9 mm) LIGACLIP™ (Ethicon, Cincinnati, USA) was used. Dissection of the gallbladder from the liver bed was done. The gall bladder was retrieved through the umbilical port site after meticulous hemostasis of the liver bed, then a drain was placed in the Morrison pouch.
Finally, the umbilical port site fascia was closed by continuous stitches using Vicryl 1, and subcuticular closure of the skin with Prolene 3/0 was routinely done.
After surgery, analgesics were given intravenously (paracetamol 1000 mg) as needed throughout the fasting period and thereafter orally when the patient tolerated oral feeding (paracetamol 500 mg tab/8 hours) for 3 days or more if necessary. During this study, no opioids were given. All patients started oral feeding once intestinal sounds were audible (usually 4–6 hours after the operation). Patients were discharged when they were pain free (visual analog scale [VAS] score <3), hemodynamically stable, tolerating oral feeding, and ambulant.
Descriptive data about patient characteristics included age, sex, BMI, comorbidities, and previous abdominal surgery.
Outcomes
Primary outcomes were biliary leak and postoperative bleeding. The secondary outcomes evaluated were the operative time, intraoperative complications (such as intraoperative blood loss [as expressed in the suction and number of gauzes used], gall bladder perforation, injury to the bile ducts, visceral injury, and conversion to open surgery), postoperative pain, length of hospital stay, and postoperative complications like incisional hernia and wound infection. The VAS, which is graded from 0 to 10, was used to assess postoperative pain. A score of 0 denotes no pain, a score of 1–3 denotes mild pain, a score of 4–6 denotes moderate pain, and a score of 7–10 denotes severe pain.
After surgery, patients were followed up at 7 days, 2 weeks, 1 month, 6 months, and 1 year.
Statistical analysis
SPSS software version 22.0 (IBM Corp., Armonk, NY, USA) was used to analyze data. Qualitative data were described using numbers and percentages. Quantitative data were described using the mean and standard deviation. For data analysis, qualitative data: chi-square test for comparison of the two groups was used. For quantitative data between the two groups: Student’s t-test was used. P value <.05 was considered statistically significant.
Results
From March 2018 to March 2020, an elective laparoscopic cholecystectomy was performed on 319 patients; out of them, 102 patients were included in the current study (Fig. 2). The patients were randomly allocated into two equal groups by the closed envelope method, Group 1 (SILC with LigaSure for closure of the cystic duct and artery) and Group 2 (SILC with closure of the cystic duct and artery with titanium clips), each group containing 51 patients. In Group 1, 46 females and 5 males were present, and in Group 2, 44 females and 7 males were present. Their mean age was 39.3 ± 13.5 years and 41.6 ± 12.8 years in Group 1 and 2, respectively. Regarding the patients’ demographic data and comorbidities, there were no significant differences between the two groups (Table 1). All patients had uncomplicated symptomatic cholelithiasis, and all procedures were elective.
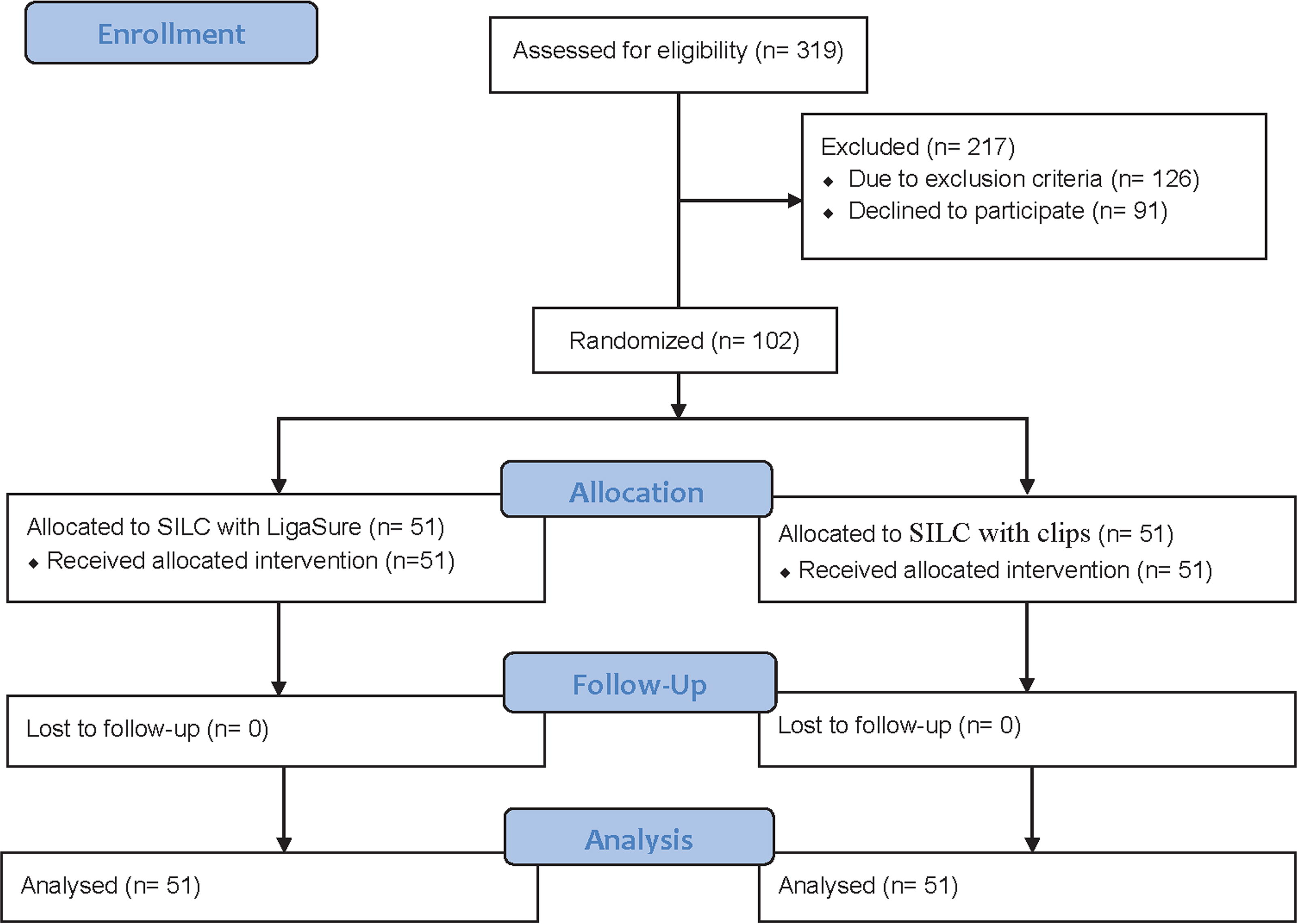
The CONSORT flow diagram of this study. SILC, single-incision laparoscopic cholecystectomy.
Patient’s Demographics and Preoperative Data
BMI, body mass index; CS, Cesarean section; SD, standard deviation.
Primary outcomes
The two groups did not show any significant difference regarding post-operative bile leak (0 in Group 1 versus 1 in Group 2, P 1.00). There was one case of bile leak in Group 2, diagnosed by bile discharge from the drain, MRCP showed leakage from the cystic duct stump due to a slipped clip. The case was managed by ERCP and a stent. None of the patients in our study developed postoperative bleeding (Table 2).
Postoperative Data
SD, standard deviation.
Secondary outcomes
The operative time was significantly shorter in the LigaSure group (68.5 ± 9.8 versus 72.9 ± 10.6 minutes in the control group, P .03). There was no significant difference between the two groups regarding intraoperative blood loss (19.3 ± 4.2 mL in Group 1 versus 22.5 ± 6.8 mL in Group 2, P .51). Regarding perforation of the gall bladder, there was no significant difference between the two groups, with five cases (9.8%) in Group 1 and three cases (5.9%) in Group 2 (P .46).
Two cases were converted to multiple port laparoscopic cholecystectomy (MPLC) in Group 1 and four cases in Group 2 (P .68). These cases were converted to MPLC because of the difficult dissection due to extensive adhesions or inadequate delineation of Calot’s triangle. There were no cases of bile duct injury or visceral injury in both groups, and no case in our study was converted to an open cholecystectomy (Table 3).
Operative Details
Statistically significant (P < .05).
MPLC, multiple port laparoscopic cholecystectomy; SD, standard deviation.
No significant difference was noted in postoperative pain 6 hours after surgery between Groups 1 and 2 (4.6 ± 1.7 versus 4.8 ± 1.5, P .58). The duration of hospital stay in Group 1 was similar to Group 2 (2.1 ± 0.3 versus 2.2 ± 0.8 days, P .22). Wound infection occurred in three cases in Group 1 and two cases in Group 2 (P 1.00), and all of them were resolved by conservative management with drainage, antibiotics, and frequent daily dressing. Two patients in each group (P 1.00) developed port-site incisional hernia. Three of them were managed by mesh repair, and one was lost during follow-up (Table 2).
Discussion
The current study was conducted to evaluate the feasibility and safety of using LigaSure for closure of the cystic duct during clipless SILC. Several studies showed that SILC is associated with reduced postoperative pain, faster recovery, decreased wound infection, and better cosmesis.4,23–25 In contrast, SILC is technically more challenging than CLC7,22 and associated with loss of triangulation, instruments conflict, and prolonged operative time.6,10,26
In our study, there was no significant difference between Group1 and Group2 with regard to demographic characteristics and BMI. Despite the wide range of the targeted age of the study (18–70), the mean age of the patients in Groups 1 and 2 was 39.3 ± 13.5 and 41.6 ± 12.8, consequently; this was related to the interest of this age group in our locality in a better cosmetic outcome. In contrast, in a study by Sang et al., the mean age of the included patients was 47.5 ± 12.2 with older age group more interested in the cosmetic outcome. 27
In the current study, most cases were female (88.2%) due to the lower interest of male patients in participating in the study, and they frequently present with acute cholecystitis.
Thirty-three patients in our study had undergone prior abdominal surgery; all of them were lower abdominal surgeries, which did not affect the procedure, and they were successfully completed without conversion. In a retrospective study by Ryu et al., which reported 309 SILCs, 40 patients of them had previous abdominal surgery, and 6 patients out of these 40 patients had previous upper abdominal surgery. Most of the procedures (96.8%) were performed without additional ports. An extra port was added or an open conversion was performed because of technical difficulties like bleeding and severe adhesions. 28
LigaSure was designed to seal blood vessels up to 7 mm and proved to be effective like other sealing methods such as Harmonic Scalpel, bipolar coagulation, and conventional vessel ligation.29,30 In addition, LigaSure has been shown to be effective in parenchymal dissection and transection31–35 and was found to be effective in hepatic resection, including division of small bile ducts.36,37 It has also been documented to seal the cystic duct in animals38,39 and in CLC in humans and proved to be safe.20,40,41 Therefore, LigaSure performs an efficient sealing of the cystic artery and duct with minimal blood loss.
The efficacy and feasibility of sealing the cystic duct during SILC with LigaSure have been evaluated in limited number of studies.
In the current study, we did not encounter any case of bile leak or postoperative bleeding. This was in harmony with Downes et al., who reported no bile leak or postoperative bleeding after LigaSure sealing of the cystic duct and artery in 28 patients who underwent clipless SILC with LigaSure. 19 Abdelmonem et al. reported two cases [6.7%] of biliary leakage after sealing of the cystic duct with LigaSure in 30 adult patients and no biliary leakage after sealing of the cystic duct with LigaSure in 15 pediatric patients who underwent CLC, and no postoperative bleeding was encountered in both groups. 41 In contrast, Abdallah et al. 14 in an ex vivo study stated that the Harmonic Scalpel is the best sealer for the cystic duct, followed by clips, and finally LigaSure. 22
The mean blood loss in our study was 19.3 ± 4.2 mL in Group 1 versus 22.5 ± 6.8 mL in Group 2 (P .51). This was consistent with the results of other studies using LigaSure, which showed a significant reduction of blood loss.31–35
The operative time was significantly shorter in Group 1 than that in Group 2 (68.5 ± 9.8 versus 72.9 ± 10.6 minutes, P .03). This could be explained by the fact that with LigaSure, there is no clipping, and the time lost in loading and inserting the clip applier into the abdomen is avoided. In addition, LigaSure was used to dissect the gallbladder from the liver bed; thus, the key steps of the procedure were performed with the same instrument, and instruments do not need to be shifted, which reduced the operative time and dissipation of heat and thermal injuries to surrounding structures. Comparable results of shorter operative time were reported in other studies using vessel sealing devices for sealing of the cystic duct.42,43
There was no significant difference in the intra- and postoperative complications between the two groups. The incidence of gall bladder perforation was not significantly different between the two groups (9.8% in Group 1 and 5.9% in Group 2). It occurred due to suture perforation or during dissection of the gallbladder from the liver. The results of our study were in accordance with data from previous researches by Guo et al. and Qu et al., who mentioned an incidence of gallbladder perforation after SILC of 12.3% and 10.6%, respectively, while Arezzo et al. showed an incidence of only 4.7%.7,44,45
In this study no cases of bile duct injury were encountered, which is consistent with the data in the literature after SILC.7,9,19,46
Two cases (3.9%) in Group 1 and four cases in Group 2 (7.8%) (P .68) were converted to MPLC. The clear visualization of Calot’s triangle is the most important point, and if it cannot be visualized properly, conversion to MPLC should be performed. This was in line with a study conducted by Downes et al., which included 28 cases subjected to clipless SILC with LigaSure; two of them (7%) were converted to MPLC due to technical difficulties. 19
In SILC, the common fulcrum between instruments and restricted number of working channels constrains the separation of hands, which is required to provide proper and easy manipulation of the tissues and lead to clashing of instruments. In our study, we used articulating laparoscopic instruments to overcome this problem. Many authors recommend the use of articulating instruments as they decrease the workload on the surgeons and make the procedure less stressful.47–49
Postoperative pain was well controlled with analgesics, and the mean pain score did not show significant difference between the two groups. Previous studies showed that postoperative pain was reduced with SILC compared with CLC.4,44,50 However, other authors concluded that SILC did not offer a significant benefit regarding postoperative pain in comparison with CLC.7,51,52
There was no significant difference between the two groups as regard the length of hospital stay (2.1 ± 0.3 days in Group 1 versus 2.2 ± 0.8 days in Group 2, P .22). This was in accordance with Arezzo et al. and Koirala et al., who reported hospital stay after SILC of 2 ± 0.74 and 2.64 ± 0.67 days, respectively, while Qu et al. reported shorter hospital stay of 1.02 ± 0.14 days, which could be due to a lower postoperative pain score than our study, which consequently shortens the length of hospital stay.7,53,54
In the current study, we encountered five cases of wound infection 3 (5.9%) in Group 1 and two (3.9%) in Group 2. This agreed with Downes et al., who reported a wound infection rate of 7% after clipless SILC with LigaSure. 19 Several studies showed that the risk of wound infection did not change with SILC compared with CLC.7,9,50
One major concern about SILC is the potential for an increased risk of incisional umbilical hernia because it requires a bigger fascial incision (2–2.5 cm) to accommodate a port device with multichannel. Therefore, it is mandatory to close the fascial defect efficiently and to avoid heavy exercises during the first 2 months postoperatively. In our study, the port-site incisional hernia incidence was 3.9% in both groups; this agreed with Klein et.al. and Lurje et al., who mentioned incidence of 5.6% and 4.1% after SILC.46,55
It is critically important to evaluate the cost-effectiveness of any surgical procedure because of the limited financial resources of the health care system. In our study, the higher cost of LigaSure was its major disadvantage, 240 US$ per LigaSureTM hand piece versus 10 US$ for a medium/large clip cartridge. The shorter operative time may partially compensate the higher cost of clipless SILC. In contrast, further research is required to determine whether it is cost-effective to recommend the routine use of clipless SILC, and larger studies with longer follow-up periods are needed for a better evaluation.
The small number of cases and short follow-up period are the limitations of this study. Nevertheless, the results were fruitful in processing a prospective randomized clinical trial comparing clipless SILC versus SILC with clips.
Conclusion
Based on the present findings, we found that clipless SILC using LigaSure is a safe, feasible, and affordable procedure with acceptable morbidity with shorter operative time than SILC using clips. Nevertheless, the risk of port-site incisional hernia should be explained to the patients. More studies are needed with a larger sample size and a longer follow-up period to adequately evaluate the outcomes of clipless SILC using LigaSure.
Footnotes
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by H.E., A.M., A.N., and A.T.-E. The first draft of the article was written by A.T.-E., and all authors commented on previous versions of the article. All authors read and approved the final article.
Disclosure Statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.