
Abstract
Objective:
To assess both the clinical effectiveness and practical experience of utilizing laparoscopic methods for addressing direct inguinal hernia in the pediatric population.
Method:
The study collected clinical data from 10 pediatric patients with direct inguinal hernia treated at the Children’s Hospital of Anhui Province from July 2014 to July 2023. Among them, there were 8 males and 2 females, with an average age of 43.4 ± 22.0 months. All were initially diagnosed with indirect inguinal hernia before surgery. During the laparoscopic procedures, direct hernia was confirmed. Two cases had undergone open hernial sac high ligation surgery due to misdiagnosis as indirect hernia, resulting in recurrent groin bulges postoperatively. For these cases, laparoscopic direct hernia neck ligation with reinforcement and repair using the inner side of the umbilical ligament was performed.
Results:
All 10 cases of pediatric patients underwent surgeries smoothly without any need for open conversion. The average surgical duration was 29.8 ± 15.0 minutes, with minimal intraoperative bleeding. Patients were discharged on the first day postoperatively, and no significant surgery-related complications were observed. During the 12-month follow-up period, it was noted that the scar at the umbilical ring was superficial and inconspicuous. There were no occurrences of hernia recurrence, testicular retraction, or atrophy.
Conclusion:
Laparoscopic treatment for pediatric direct inguinal hernia has demonstrated favorable therapeutic outcomes, ensuring a safe surgical process, rapid recovery, and a low postoperative recurrence rate. The laparoscopic approach, specifically utilizing direct hernia neck ligation with reinforcement and repair using the inner side of the umbilical ligament, proves to be a secure and effective treatment for pediatric direct inguinal hernia. It can be considered as a conventional treatment method.
Introduction
In children, inguinal hernia is one of the most common conditions in pediatric surgery, with the majority being indirect inguinal hernias, resulting from the failure of the congenital processus vaginalis to close, exceeding 95%. 1 In addition to indirect hernias, there are also some rare types of hernias, such as direct hernias, sliding hernias, and femoral hernias. Among these uncommon types, direct hernias are relatively more prevalent, constituting approximately 81.5% of rare hernias. 2 Direct inguinal hernia can be either congenital or acquired, resulting from the weakening of the abdominal wall, allowing abdominal contents to protrude through the fascia. 3 The hernial sac of a direct inguinal hernia is located on the inner side of the inferior epigastric artery, making it relatively easy to diagnose during laparoscopic surgery. However, it is often prone to misdiagnosis in the preoperative stage of pediatric direct inguinal hernia. 4 From July 2014 to July 2023, a total of 9827 cases of pediatric inguinal hernia were treated with laparoscopic procedures at the Children’s Hospital of Anhui Province. Among them, 10 cases of direct inguinal hernia were identified intraoperatively through laparoscopy, with an incidence rate of approximately 0.1%. The incidence rate in this study is comparatively lower than that reported in previous studies on direct inguinal hernia.5,6 This study explores the therapeutic efficacy and clinical experience of utilizing laparoscopic direct hernia neck ligation with reinforcement and repair using the inner side of the umbilical ligament for the treatment of pediatric direct inguinal hernia.
Clinical Data and Methods
Clinical data
This study collected clinical data from 10 pediatric patients with direct inguinal hernia treated at the Children’s Hospital of Anhui Province from July 2014 to July 2023. Among them, there were 8 male and 2 female patients, with an average age of 43.4 ± 22.0 months. All were initially diagnosed with indirect inguinal hernia before surgery. During the laparoscopic procedures, direct hernia was confirmed. Two cases had undergone open hernial sac high ligation surgery due to misdiagnosis as indirect hernia, resulting in recurrent groin bulges postoperatively. Specifically, five cases were on the right side (including one case with bilateral direct inguinal hernias), three on the left side, and two were bilateral. Detailed patient information is provided in Table 1.
Clinical Data of Pediatric Patients
Surgical methods
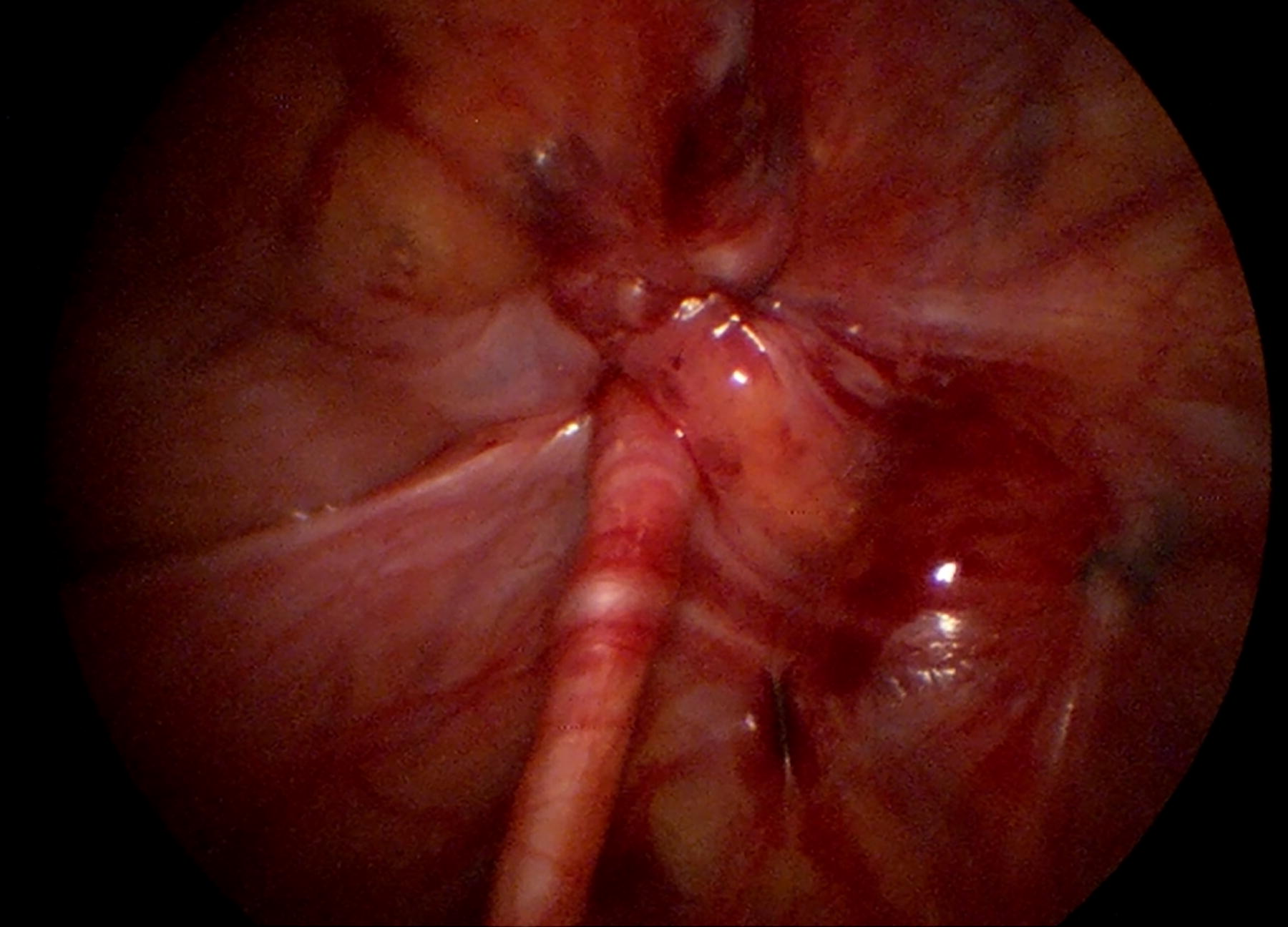
All 10 pediatric patients underwent laparoscopic direct hernia neck ligation with reinforcement and repair using the inner side of the umbilical ligament. The specific surgical procedure is as follows: the patients received combined general anesthesia with endotracheal intubation and were placed in a supine or Trendelenburg position. A 5 mm incision was made at the right edge of the umbilicus, and a trocar was inserted to establish CO2 pneumoperitoneum with a pressure of 6–12 mmHg. A 30° laparoscope was inserted, and an assistant held the camera. A 3 mm incision was made on the left edge of the umbilicus for the placement of a trocar (Fig. 1). The intra-abdominal situation was observed under laparoscopy, and the direct hernia sac was visualized between the abdominal wall and the inferior epigastric vessels and the inner side of the umbilical ligament (Fig. 2). A vascular clamp was used to press and adjust on the skin surface to determine the midpoint of the projection of the direct hernia sac opening as the needle insertion point. Using a handmade hernia needle with a No. 4 suture, the needle was inserted from the skin surface projection of the direct hernia sac opening, passed externally around the hernia sac for half a circle, and reentered the abdominal cavity. The suture end was left inside the abdominal cavity, and the hernia needle was withdrawn outside the peritoneum, then reinserted from the inner side of the hernia sac opening, passed internally to the original puncture hole, entered the abdominal cavity, and pulled the suture out of the abdominal wall to tie a knot and close the hernia ring (Fig. 3). Using the same handmade hernia needle and No. 4 suture, the needle was inserted from the outer side of the hernia sac opening, entered the abdominal cavity, pierced the inner side of the umbilical fold, and left the suture in place. The hernia needle was withdrawn outside the peritoneum, reentered the abdominal cavity 1 cm below the initial puncture point, and pulled the suture out of the abdominal wall to tie a knot, completing the reinforcement and repair (Fig. 4, Fig. 5). After confirming no intra-abdominal injuries or bleeding, the laparoscope was removed, and the incision near the umbilicus was closed with sutures (Fig. 6).
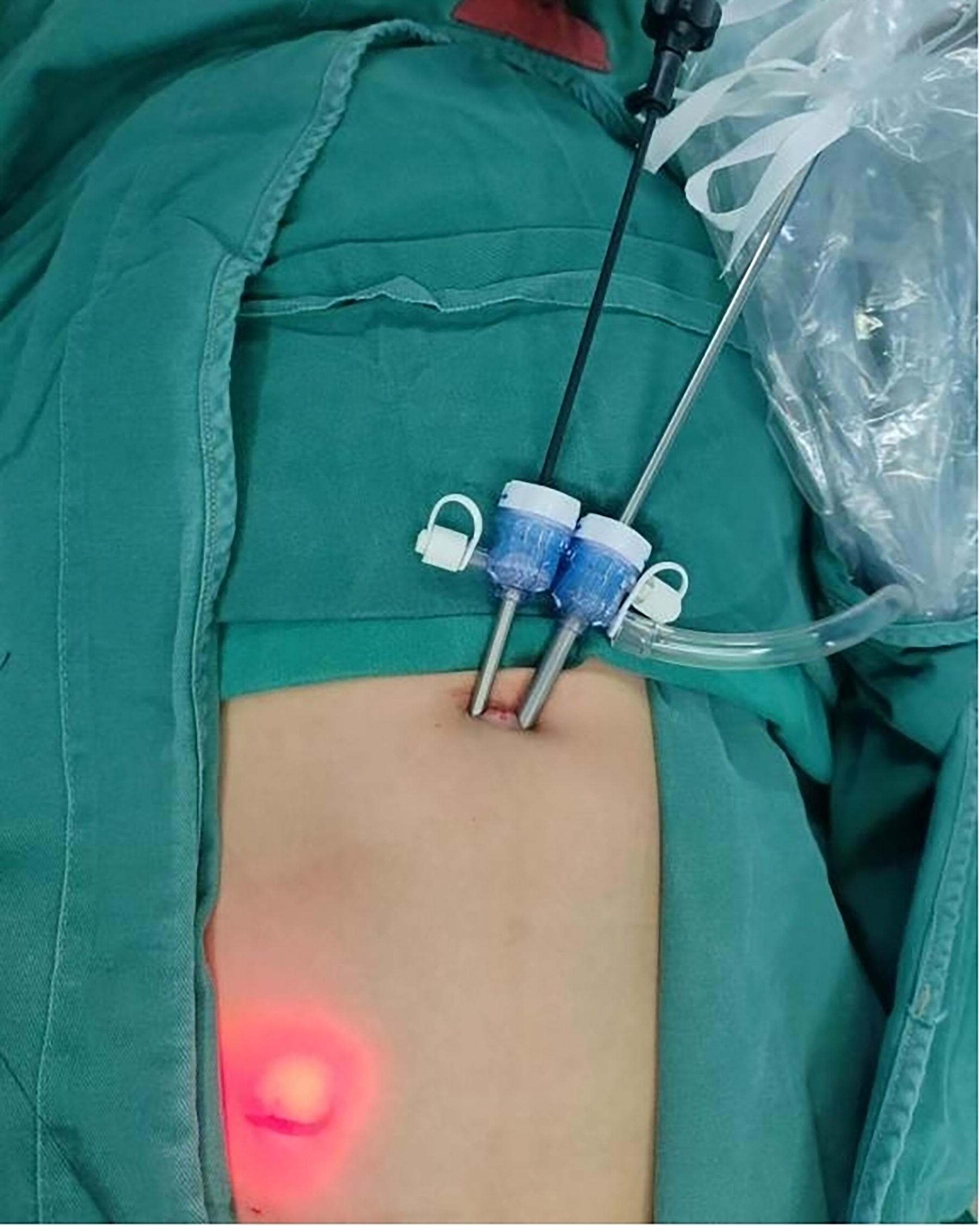
Surgical trocars placed on both sides of the umbilicus.
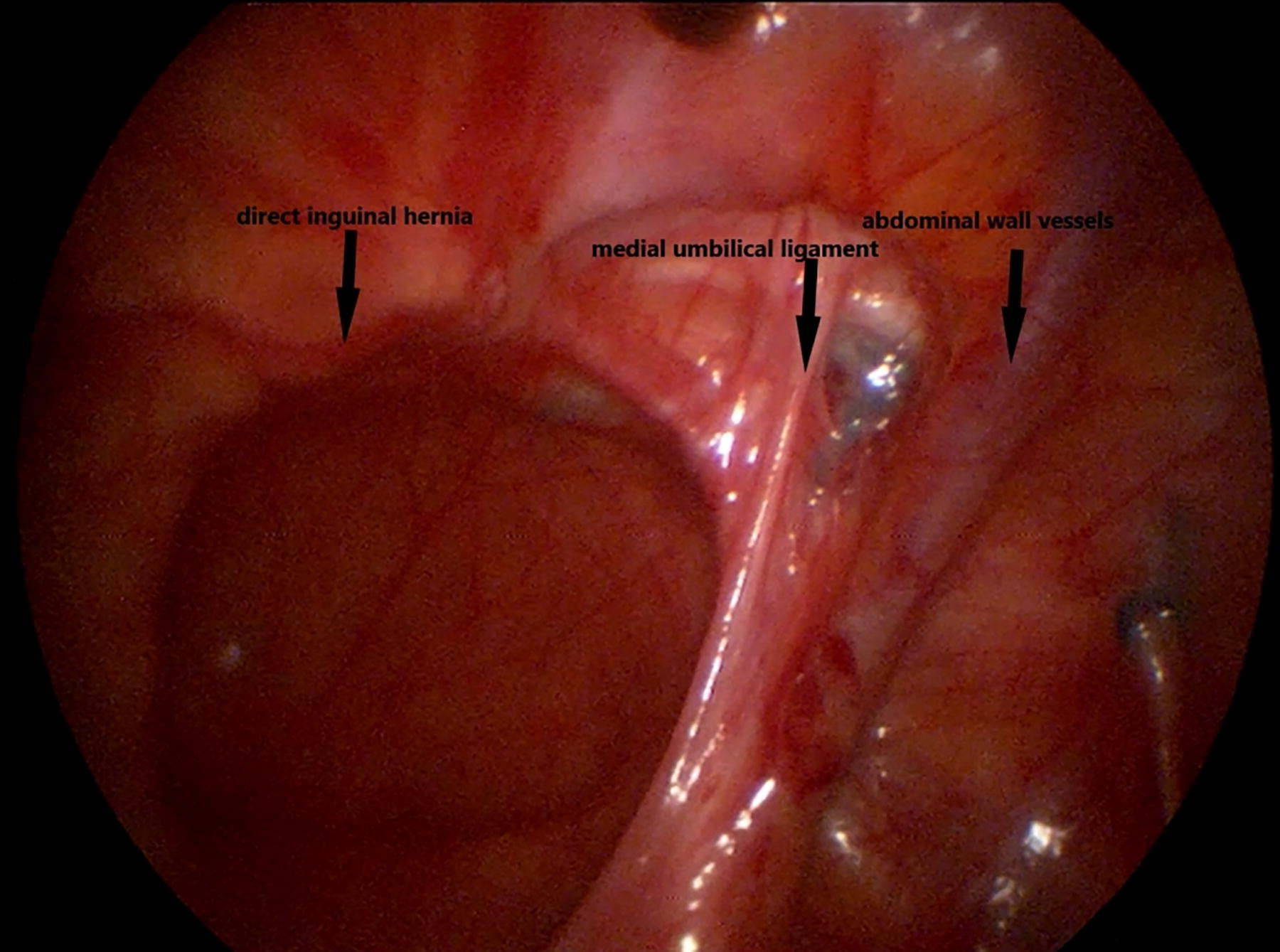
Perioperative anatomy of inguinal direct hernia under laparoscopy.

Laparoscopic ligation of the direct hernia ring.

Covering and reinforcing with the preperitoneal side of the inguinal ligament.
Post-surgery visuals for direct inguinal hernia.

Appearance of umbilical closure after surgery.
Results
All patients underwent the procedures smoothly without any need for open conversion. The average surgical duration was 29.8 ± 15.0 minutes, and there was minimal intraoperative bleeding. No significant surgery-related complications were observed. On the morning of the first postoperative day, all patients were discharged successfully, and there were no signs of incision infection or scrotal hematoma. During the follow-up period of 12 months, it was noted that the scar at the umbilical ring was superficial and inconspicuous. There were no occurrences of hernia recurrence, testicular retraction, or atrophy.
Discussion
Direct inguinal hernia is relatively uncommon in childhood, constituting approximately 0.98% to 3.9% of inguinal hernia cases. Its anatomical foundation lies in the congenital weakness or deficiency of the local abdominal wall. This condition is more prevalent in boys than girls and typically manifests between 6 months and 10 years of age, with a higher incidence on the right side than the left.7,8 The primary risk factors for the occurrence of direct inguinal hernia in children include weakened abdominal wall and transversalis fascia, increased intra-abdominal pressure, abnormalities in the genitourinary system, and preterm birth.8,9 Direct inguinal hernia is characterized by an incomplete and insufficient muscle covering in the triangle formed by the inferior epigastric artery, the outer edge of the rectus abdominis muscle, and the inguinal ligament. At this site, the peritoneum and fascia are relatively weak. In addition, the gap between the transversalis fascia arch formed by the internal oblique muscle and transversus abdominis and the inguinal ligament is excessively large. These factors contribute to the protrusion of abdominal organs from the posterior to the anterior, leading to the formation of direct inguinal hernia. 10 The herniated contents of a direct inguinal hernia protrude outward from the Hesselbach’s triangle, typically not entering the scrotum. In contrast, the herniated contents of an indirect inguinal hernia enter the same-side scrotum through the inguinal canal, exerting pressure on the inner ring but not extending further outward. In the case of a direct inguinal hernia, the herniated contents continue to protrude continuously. 5 In theory, distinguishing between the two types of hernias can be based on this criterion. However, due to the proximity of Hesselbach’s triangle to the inner ring and the short length of the inguinal canal in pediatric patients (<0.5 cm), where the inner and outer rings almost overlap, it becomes challenging to differentiate inguinal hernias preoperatively, especially in cases of indirect hernias with herniated contents located at the inguinal canal, such as spermatic cord hernias or inguinal hernias in female children. 11 In recent years, with the increasing prevalence of laparoscopic surgery, a reliable method for diagnosing direct inguinal hernia has been provided. Consequently, literature reports have shown a noticeable increase in the incidence of direct inguinal hernia compared with the past. 12 If, during laparoscopic surgery, it is observed that the internal ring of an indirect inguinal hernia has closed, careful exploration of the direct hernia triangle for any defects is necessary. Preoperative bladder emptying is also beneficial for accurate exploration during the procedure. With laparoscopy, the position of the hernia sac opening can be visually inspected. If it is located on the inner side of the inferior epigastric artery, a diagnosis of direct inguinal hernia can be made, whereas if it is located on the outer side of the vessels, it is indicative of an indirect hernia. 13 It is worth noting that on the same side, there may be simultaneous presence of both direct and indirect hernias, a condition also known as Pantaloon hernia. This is more easily observed during laparoscopic examinations. 14
The surgical approach for pediatric direct inguinal hernia can be categorized into open repair and laparoscopic repair. The classical open technique is the McVay procedure, which involves high ligation of the hernia sac followed by suturing the arch formed by the transversalis fascia arch, the internal oblique muscle, and the transversus abdominis to the inguinal ligament. This anatomically aims to eliminate the weakness and defect in the abdominal wall. 15 The use of laparoscopy for identification and repair of pediatric direct inguinal hernia has been proven to be a safe, swift, and effective approach. 16 Compared with traditional open surgery, laparoscopic surgery offers advantages such as reduced postoperative pain, smaller scars, effective detection of contralateral occult patent processus vaginalis, decreased risk of metachronous hernias, and accurate identification of other rare hernias and intra-abdominal diseases. 17 While laparoscopic ligation of the direct inguinal hernia sac opening can temporarily eliminate the peritoneal defect, it does not address the abdominal wall defect, leading to a higher risk of postoperative recurrence.18,19 Ideally, reinforcement and repair of the direct hernia triangle region should be performed. However, suturing and repairing this area can be challenging during laparoscopic procedures, and it is not advisable to use mesh for tension-free repairs in children.20,21 In children, the development of the inner side of the umbilical ligament is robust, providing adequate tension and flexibility. Covering and reinforcing it over the hernia sac opening can effectively prevent intra-abdominal organs from protruding through the weakened abdominal wall, reducing the risk of hernia recurrence. 22 Moreover, the umbilical ligament tissue is native to the child, avoiding potential complications such as rejection and infection that may arise from using mesh. This reduces the adverse impact on the child’s reproductive structures and functions. A study indicates that approximately 89% of children have fibrous cord-like umbilical ligaments, suggesting that a sufficient amount of umbilical ligament can be found for covering in the surgical repair of direct inguinal hernia in the majority of children. 23 Esposito et al. 24 summarized the key points of laparoscopic repair for direct inguinal hernia as follows: (1) ensure bladder emptying preoperatively to avoid interference with the field of view, (2) remove the fatty tissue at the base of the hernia sac to prevent recurrence, (3) intermittently close the defect with nonabsorbable sutures, and (4) utilize the inner side of the umbilical ligament for covering and reinforcement. In this study, all 10 patients did not have fatty tissue, and we utilized the inner side of the umbilical ligament as the repair material. This was used to reinforce the posterior wall of the inguinal canal, strengthen the direct hernia triangle, and compensate for the limitations of simple high ligation of the hernia sac. Postoperatively, none of the 10 patients experienced a recurrence of direct inguinal hernia, and no specific complications were observed, demonstrating the safety and effectiveness of this method.
The limitations of this study include a small sample size, short follow-up duration, and regional bias as a result of being a single-center study. Despite these potential limitations, the study results still offer valuable insights into the safety and effectiveness of laparoscopic surgery for the treatment of pediatric inguinal hernia. Future research could enhance the study findings, improve credibility, and broaden applicability by increasing the sample size, extending the follow-up period, and conducting multicenter studies. In summary, compared with traditional open surgery, laparoscopic procedures offer advantages of a broader field of view and clearer anatomy, enabling accurate diagnosis of various types of inguinal hernias. For pediatric patients with direct inguinal hernia, if conditions permit, it is recommended to prioritize laparoscopic exploration. Following the confirmation of a direct hernia, it is advisable to perform high ligation of the hernia sac and then utilize the inner side of the umbilical ligament on the same side to cover the direct hernia triangle. This represents a simple, safe, and effective surgical approach.
Footnotes
Authors’ Contributions
C.T., Y.C., and C.M. contributed to study concept and design. All authors contributed to data collection. C.T., Y.C., and C.M. contributed to data analysis and writing the first draft of the article.
Ethics Approval
This study was conducted with the approval of the Ethics Committee of Anhui Children’s Hospital.
Consent to Participate
Informed consent was obtained from parents or legal guardians who were present during examination, history, and sampling sessions.
Disclosure Statement
C.T., Y.C., and C.M. declare that they have no conflicts of interest or financial ties to disclose.
Funding Information
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.