
Abstract
Background:
This investigation evaluates the utility and benefits of integrating interprofessional education (IPE) into laparoscopic training, aiming to enrich medical education and skill acquisition methodologies.
Methods:
The study randomly allocated 36 participants of a 2023 laparoscopic training course into experimental and control groups, each comprising 18 individuals. The control group underwent traditional theory and practical training, whereas the experimental group additionally engaged in interdisciplinary instruction with nursing educators and participated in simulated laparoscopic surgery exercises. The effectiveness of this interdisciplinary approach was assessed by comparing laparoscopic theory and simulation performance, Objective Structured Assessment of Technical Skills (OSATS) scores in animal-based training, and course satisfaction between the groups. Moreover, the impact on interdisciplinary collaborative competencies was measured through pre- and post-training self-evaluations using the Interprofessional Collaborative Competency Attainment Survey (ICCAS) in the experimental group.
Results:
The experimental group demonstrated superior performance in laparoscopic theory and simulation, as well as higher OSATS scores, compared with the control group. Satisfaction ratings regarding the skills practice mode, effects, and instructional quality were also significantly better in the experimental group (P < .05, P < .01). Furthermore, participants in the experimental group reported significant pre-to-post training enhancements in interprofessional communication, team collaboration, role perception, conflict management, and learning and feedback marked by statistically significant differences (P < .05, P < .01).
Conclusion:
The introduction of an IPE framework significantly boosts laparoscopic training efficiency and promotes team collaboration awareness. This model effectively bridges gaps between disciplines, illustrating substantial applicative value and expansion potential within medical education and skill training arenas.
Introduction
Laparoscopic surgery represents a pivotal innovation in the surgical domain, establishing itself as the technique of choice for an array of surgical interventions. This method is distinguished by several advantages, including diminished postoperative discomfort, expedited patient recovery, and a reduction in perioperative complications and mortality rates.1–2 The efficacy of laparoscopic procedures is intricately linked to the proficiency and experience of the leading surgeon, underscored by the synergistic cooperation within the surgical team.3–4 Given the inherent complexities and steep learning trajectory associated with laparoscopic technology, the imperative for specialized training is pronounced. 5 Nonetheless, prevailing training frameworks tend to emphasize technical skill acquisition, often overlooking the criticality of integrating and applying interdisciplinary knowledge. This oversight underscores the need for a more holistic and refined approach to training paradigms.
In China, since the first successful laparoscopic cholecystectomy in 1987, there has been a marked transition from open to minimally invasive surgeries, echoing the global trend. 6 However, traditional training in China has often relied on an “apprenticeship” model, which may not adequately prepare surgeons with the interdisciplinary knowledge necessary for mastering advanced laparoscopic skills.7–8 This study proposes a holistic training approach, hypothesizing that the integration of interprofessional education (IPE) into laparoscopic training will enhance not only the technical skills of surgical residents but also their collaborative competencies. We anticipate that IPE will improve skill acquisition and instill a collaborative spirit in line with international standards like the Fundamentals of Laparoscopic Surgery program. 9 Standardized modules for surgical-nursing collaboration represent a huge step toward establishing a more systematic and interdisciplinary training approach in China. The approach yielded positive outcomes, as detailed herein.
Materials and Methods
Participant selection and baseline characteristics
In a randomized controlled trial conducted from May to October 2023 at Shanghai Changhai Hospital, 36 third-year surgical residents undergoing standardized residency training and with no prior laparoscopic training were enrolled. The participants included 30 males and 6 females with an average age of 28.78 ± 1.94 years. These participants were randomly divided into two groups—experimental (n = 18) and control (n = 18)—based on their gender, using computer-generated allocation. Prior to the study, a prestudy survey was administered to collect demographic details, including gender, educational background, the number of laparoscopic surgeries previously participated in, and overall surgical experience, after obtaining informed consent from all participants.
Baseline assessment of theoretical knowledge and practical skills in laparoscopy was conducted on two groups of trainees before the training. Practical skills assessment included hand–eye coordination, cutting skills, instrument handling, directional training, and suturing techniques, encompassing five specific skills (Table 1), as well as overall proficiency and time taken for completion, as measured by two comprehensive evaluations.
Laparoscopic Practical Skills Assessment
Educational protocol
Phase1 IPE faculty team formation
To establish an interdisciplinary faculty, we selected six clinical surgical instructors and two nursing professionals, all with significant expertise and senior qualifications. These instructors completed a rigorous certification process, earning the “Shanghai Standardized Resident Physician Training Certificate.” As per the Chinese Medical Doctor Association’s “Guidelines for Teaching Activities in the Standardized Training of Resident Physicians” (2022 Edition), the training curriculum for standardized resident physicians encompasses a comprehensive range of activities. These include not only intraoperative interactions but also essential preoperative and postoperative educational components, along with fostering professional interactions. 10 Before course launch, the team underwent a week of focused training on interdisciplinary education principles, strategies, and tailored pedagogical methods for clinical and nursing domains. This preparation aimed to optimize the educational framework and effectiveness through strategic interdisciplinary teaching approaches.
Phase 2 course design
The control group engaged in a structured curriculum comprising instructor-led demonstrations and individual operational exercises, covering laparoscopic theory, single-operator simulations, and direct animal surgery practice. In contrast, the experimental group, in addition to the aforementioned foundation, integrated four interdisciplinary educational (IPE) components as follows: Clinical Reasoning, Team Collaboration Simulation Drills, Collaborative Medical and Nursing Animal Surgery Training, and Visualization-Based Evaluation of Laparoscopic Procedures (Fig. 1). The specifics of the interdisciplinary educational program’s implementation are as follows:
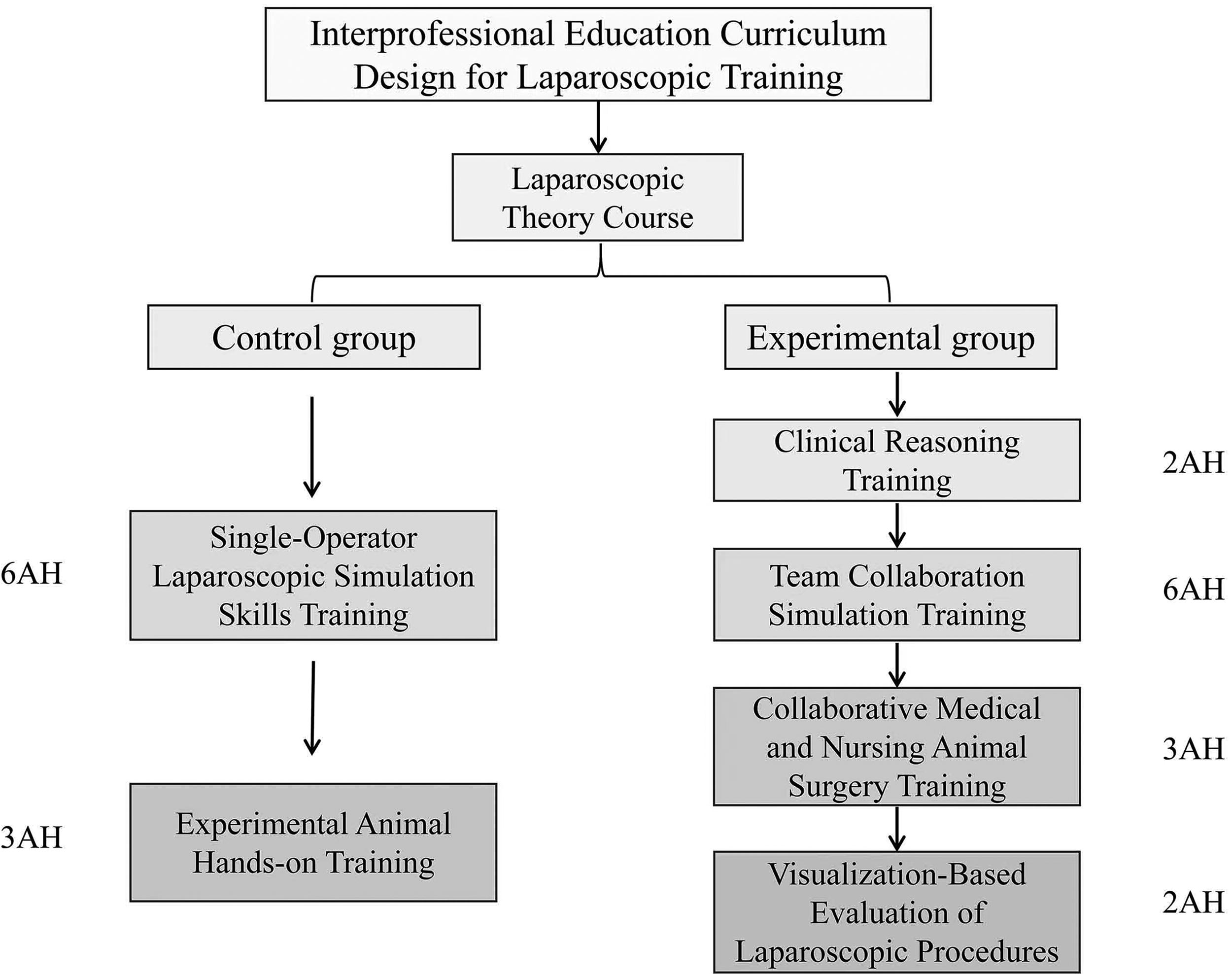
IPE curriculum design for laparoscopic training. 1 AH = 40 minutes. AH, academic hour; IPE, interprofessional education.
Clinical Reasoning Training. Leveraging laparoscopic theory, surgical instructors enriched the curriculum with analyses of surgical techniques, complex operation strategies, case management, and emergency responses. Nursing educators focused on surgical staff’s preoperative and perioperative care. Through simulated surgical teams—assigning roles such as lead surgeon, assistant, and camera operator, alongside nursing positions like circulating and scrub nurse—the program emphasized surgery indications, preparation, instrument selection, and teamwork via case simulations. Emergency protocols and postoperative complication analysis were also developed. Guided by surgical instructors who posed critical questions, the initiative aims to enhance students’ clinical reasoning and emergency handling, ensuring proficiency in surgical environments.
Team Collaboration Simulation Training. Under the guidance of surgical instructors, the surgical simulation team underwent fundamental skills training on a laparoscopic simulator, encompassing camera navigation, instrument handling, orientation, cutting, and suturing with knotting, each participant engaging for 4 AH (academic hours, being 40 minutes). Roles among team members—comprising lead surgeon, assistant, and camera navigator—were rotated to facilitate collaboration with surgical and circulating nurses in advanced tasks, including ex vivo animal organ dissection, electrosurgery, and complex suturing, dedicating two academic hours per person. Instructors offered precise feedback, corrections, and directives to enhance procedural proficiency and teamwork synergy.
Collaborative Medical and Nursing Animal Surgery Training. Guided by nursing educators, the surgical team, including lead surgeons, assistants, and endoscope operators, executed preoperative steps involving animal preparation, medication and equipment verification, and site disinfection. In laparoscopic surgery, tasks included identifying entry points, establishing pneumoperitoneum, and utilizing customized instruments. The lead surgeon performed key procedures like incisions and suturing, with assistants managing tissue. Instrumentation and circulating nurses ensured the availability of tools and compliance with operating room standards. Prior to closure, inventory checks were conducted to prevent discrepancies. Simulated emergencies, such as bleeding, tissue tears, and item count errors, facilitated by surgical instructors, tested the team’s crisis management skills. The process was evaluated through an Objective Structured Assessment of Technical Skills (OSATS) and documented via real-time video for analysis.
Visualization-Based Evaluation of Laparoscopic Procedures. Postoperatively, surgical mentors engage trainees in surgical video reviews, providing an in-depth visual assessment of procedural standardization, tissue protection efficiency, operational timing, team synergy, and the prompt and accurate management of emergencies. This evaluative approach not only enhances trainees’ insight into their surgical proficiency but also, through case analysis, advances their understanding and command of key laparoscopic techniques, thereby establishing a robust foundation for their future clinical endeavors.
Phase 3 post-training assessment
Assessment of Educational Impact: We assessed the educational intervention’s efficacy through comprehensive pre- and post-training evaluations encompassing laparoscopic knowledge, simulator performance, and the OSATS, a robust metric for gauging surgical proficiency, that were applied across 10 domains: aseptic technique, preoperative readiness, tissue handling, time and motion efficiency, instrument proficiency, teamwork, procedural knowledge, emergency management, perioperative care, and overall performance.8–9 Scores were assigned on a 10-point scale, with a maximum score of 100.
Course Satisfaction Assessment: Participant satisfaction was evaluated using a tailored survey with a 1 to 5 rating scale, where a higher score reflected greater contentment with the course curriculum and delivery.
Interprofessional Collaborative Competency Attainment Survey (ICCAS): This instrument, adapted from Archibald et al.’s scale, captures changes in interprofessional communication, team collaboration, role perception, conflict management, surgical strategy, and learning feedback. 11 Self-assessments were conducted using a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree), to precisely evaluate participants’ agreement on key dimensions.
Statistical analyses
Statistical analyses were conducted using SPSS 26.0 software. Data normality was assessed using the Shapiro–Wilk test. Normally distributed metrics were expressed as mean ± standard deviation (SD) and compared between groups using independent samples t-tests and within groups using paired samples t-tests. Categorical data were analyzed using the chi-square (χ2) test. Non-normally distributed metrics were presented as median and interquartile range, with group comparisons made using the Wilcoxon rank-sum test. A P value <.05 was considered statistically significant.
Results
Comparison of assessment scores between two groups of students
There were no significant differences between the two groups of trainees in demographic characteristics and previous laparoscopic surgery experience. Baseline scores for theoretical and practical skills before laparoscopy training showed no significant differences between the groups, indicating their comparability (Table 2).
Participants’ Characteristics
Ctrl. group, control group; exp. group, experimental group; SD, standard deviation.
Following the training, both experimental and control groups underwent reassessment of laparoscopic theory and practical skills. The outcomes revealed significant improvements in both theoretical knowledge and practical abilities across all participants compared with their pretraining performance, indicating statistical significance. Notably, the experimental group demonstrated significantly superior practical skills post-training compared with the control group, with this difference also being statistically significant (P < .01), as shown in Figure 2.

Pre- and post-training assessment score dynamics among trainees.
Comparative analysis of OSATS in animal training operations between two student groups
In animal-based surgical training, a comparative analysis of OSATS scores between training groups demonstrated that the experimental group’s performance was statistically significantly superior to that of the control group (Table 3). Particularly in teamwork, the experimental group scored an absolute difference of 1.06 points higher than the control group. Similarly, in perioperative care, the experimental group’s score was 1.11 points higher. When evaluating the total aggregate score, the experimental group’s average was 8.5 points higher compared with the control group, with the aforementioned differences being statistically significant (P < .01).
Mean Differences in Objective Structured Assessment of Technical Skills Scores Among Participants
P < .05.
P < .01.
SD, standard deviation.
Comparative analysis of course satisfaction scores between two student groups
Following the course, statistical analyses of student revealed positive evaluations in course structure, skill practice efficacy, and teaching quality. Notably, the experimental group reported significantly higher satisfaction in skill practice and teaching quality compared with the control group, with statistical significance observed (P < .01), as detailed in Table 4.
Evaluation of Course Satisfaction Scores Among Participants
SD, standard deviation.
Pre- versus Post-Training ICCAS Self-Assessment scores in the experimental group
Utilizing the ICCAS for self-evaluation, experimental group participants demonstrated significant improvements in IPE outcomes, as shown in Table 5. Post-IPE, substantial gains were observed in “interprofessional communication,” “team collaboration,” “role perceptions,” “conflict management,” and “learning feedback” (P < .01). However, the rise in “surgical strategy” scores, although present, did not achieve statistical significance (P > .05).
Self-Assessment of Interprofessional Collaborative Competency Attainment Survey Among Experimental Group Participants
IQR, interquartile range.
Discussion
Over the last 30 years, laparoscopic surgery has become the technique of choice for a wide range of surgical interventions due to its enhanced outcomes for patients. 3 Nonetheless, the procedure’s technical complexity surpasses that of conventional open surgeries, requiring surgeons to attain a greater level of proficiency to reduce complication risks effectively. 12
In the context of restricted work hours and increased administrative burdens, young surgeons face significant limitations in operating room exposure.13–14 Coupled with escalating surgical complexity and evolving patient expectations, the traditional “see one, do one, teach one” apprenticeship model is insufficient for 21st-century surgical training, especially with the growing complexity of laparoscopic procedures necessitating extracurricular training opportunities. 15 Systematic laboratory training is a critical component of effective laparoscopic training, mitigating the learning curve and facilitating the transition of acquired skills into clinical practice.16–17 However, it is important to recognize that proficiency in laparoscopy requires a comprehensive approach, including but not limited to laboratory training. This approach should encompass a variety of educational strategies, such as theoretical instruction, simulation-based exercises, and clinical experience, to ensure a well-rounded skill set and patient safety.16–18 Our research indicates that participants, across both control and experimental groups, demonstrated significant improvements in theoretical knowledge and practical skills following laparoscopic training.
With the popularization of medical and team-based care models, strengthening interprofessional collaboration in health care has become an inevitable trend. 17 The International Education Committee has emphasized the importance of IPE development in 21st-century medical education. 19 In laparoscopic surgery, different professions have different responsibilities, but the current global training of laparoscopic surgical talent primarily focuses on the perspective of doctors, leading to students lacking interdisciplinary knowledge and a comprehensive understanding of the roles of various professions in the health care system.20–22 Therefore, in the implementation of IPE, the key is to cultivate students’ autonomy and collaborative abilities, guided by clinical needs.
In this study, the laparoscopic training experimental group introduced nursing faculty for instruction, established interdisciplinary simulated laparoscopic surgery groups for practical training, broke down disciplinary barriers, transformed medical-nursing collaboration from passive to interactive, provided higher quality services, and benefited patient health, and the results showed significant advantages in skill performance, surgical quality assessment, and course satisfaction in the experimental group. These findings emphasize the effectiveness of incorporating IPE into laparoscopic skills training, leading to improved student skills and satisfaction. Currently, the IPE theory has been practically applied in wide range of medical practice, such as the multidisciplinary team approach in oncology. 23 By integrating diverse expertise, IPE enhances patient outcomes and promotes effective communication across specialties. Moreover, it supports technological innovations in diagnostics, improving the accuracy and efficiency of medical care. 24 We advocate for IPE to be an integral part of health care education, equipping professionals to provide comprehensive, high-quality care and emphasizing its necessity for fostering interdisciplinary collaboration in modern medicine.
Limitations
Our study was confined to a simulated setting and did not evaluate the influence of the IPE program on actual clinical practice and patient care. The limitation to students from a single medical school and the use of self-assessment scales could introduce biases, potentially impacting the generalizability of our results. Future studies should involve a broader range of institutions, incorporate objective assessment methods, and track participants in clinical environments to assess the long-term impact of IPE on patient communication and clinical outcomes.
Conclusion
The integration of IPE into laparoscopic skills training shows great promise. This approach not only enhances the educational experience and learning outcomes of participants but also promotes teamwork and improves the quality of patient-centered medical care. Our research strongly supports the incorporation of IPE into existing laparoscopic skills training programs.
Footnotes
Acknowledgments
The authors express their sincere gratitude to Professor He Qian from the Department of Military Health Statistics, Naval Medical University, for her invaluable assistance in the application of statistical methods and data review for this study. The authors also thank all colleagues who participated in discussions and provided feedback.
Authors’ Contributions
Y.L. and J.Z. contributed equally to this work as co-first authors. Y.L.: Conceptualization, methodology, writing—original draft preparation. J.Z.: Conceptualization, methodology, writing—review and editing, visualization. L.C.: Investigation, funding acquisition.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This study was supported by