
Abstract
Background:
Lung cancer is a leading cause of cancer deaths in the United States. An increasing understanding of relevant non-small cell lung cancer (NSCLC) biomarkers has led to the recent development of molecular-targeted therapies and immune checkpoint inhibitors that have revolutionized treatment for patients with advanced and metastatic disease. The purpose of this review is to provide surgeons with a state-of-the-art understanding of the current medical and surgical treatment trends and their implications in the future of management of NSCLC.
Materials and Methods:
A systematic search of PubMed was conducted to identify English language articles published between January 2010 and March 2024 focusing on molecular markers, tumor targeting, and immunotherapy in the diagnosis and treatment of NSCLC. Case series, observational studies, randomized trials, guidelines, narrative reviews, systematic reviews, and meta-analyses were included.
Results:
There is now increasing data to suggest that molecular-targeted therapies and immune therapies have a role in the neoadjuvant setting. Advances in intraoperative imaging allow surgeons to perform increasingly parenchymal-sparing lung resections without compromising tumor margins. Liquid biopsies can noninvasively detect targetable mutations in cancer cells and DNA from a blood draw, potentially allowing for earlier diagnosis, personalized therapy, and long-term monitoring for disease recurrence.
Conclusions:
The management of NSCLC has advanced dramatically in recent years fueled by a growing understanding of the cancer biology of NSCLC. Advances in medical therapies, surgical techniques, and diagnostic and surveillance modalities continue to evolve but have already impacted current treatment strategies for NSCLC, which are encompassed in this review.
Introduction
In 2022, lung cancer remained the leading cause of cancer death in the United States and worldwide. 1 Approximately, 85% of newly diagnosed cases of lung cancer are non-small cell lung cancer (NSCLC), which includes adenocarcinoma and squamous cell carcinoma histology. 2 Historically, long-term survival after NSCLC diagnosis is poor. Twenty years ago, standard of care for those diagnosed early in the course of their disease involved anatomical lung resection with the selective use of adjuvant platinum-based chemotherapy. 3 Despite this, even early-stage patients could expect a >50% risk of recurrence and relatively low 5-year survival rates. Most patients are diagnosed with late-stage or metastatic disease and rarely survive more than 1 year after diagnosis.
However, in the past two decades, there has been dramatic growth in our understanding of the cellular and molecular underpinnings of NSCLC. This has resulted in new targeted therapies and immune checkpoint inhibitors (ICIs) that can be matched to the genetic profile of patients’ specific tumors, enabling patients to live longer with more tolerable side effects. Trials of neoadjuvant chemoimmunotherapy show that surgery after immune checkpoint inhibition is safe and holds promise in improving recurrence rates and progression-free survival.4–6 “Liquid biopsies” can noninvasively detect targetable mutations in cancer cells and DNA from a blood draw, potentially allowing for earlier diagnosis, personalized therapy, and long-term monitoring for disease recurrence. 7 Advances in intraoperative imaging allow for parenchymal-sparing lung resections without compromising margins.8,9 The purpose of this narrative review is to provide a brief overview of the targetable genetic mutations involved in NSCLC and an up-to-date summary of the evolving therapies and practices in the treatment of NSCLC.
Methods
A systematic search was performed in PubMed using the Medical Subject Heading (MeSH) terms “carcinoma,” “non-small-cell lung cancer,” “molecular targeting,” and “immunotherapy.” English language articles from January 2010 to March 2024 were included, encompassing case series, observational studies, randomized controlled trials, guidelines, narrative reviews, systematic reviews, and meta-analyses. This search yielded 471 articles. The search was then constrained to articles focused on molecular markers, tumor targeting, and immunotherapy in the diagnosis and treatment of NSCLC. The authors then reviewed article abstracts and content to identify those studies judged to be of particularly high relevance and quality. Older studies were also reviewed and included if deemed having high historical importance as referenced in more recent articles. This review did not involve human or animal subjects or data from human participants, and accordingly was waived from approval by the medical center’s Institutional Review Board.
Biomarker-Driven Treatments in NSCLC
There has been significant growth in the understanding of the genetic alterations in NSCLC, which has in turn driven drug development. These therapies broadly fall into two categories: molecular-targeted therapies and ICIs. Targeted therapies directly inhibit tumorigenesis and proliferation by selectively binding cancer cell receptors with specific genetic mutations. ICIs instead enable the body’s immune system to selectively target and destroy developing cancer cells.
Molecular-targeted therapies
Approximately, 25% of patients with NSCLC harbor an actionable genetic mutation (see Table 1). For this subset of patients, many new treatments have shown durable efficacy and improved patient survival. 10 These targeted therapies directly inhibit tumor signaling and proliferation by binding to receptors with specific genetic mutations. To date, some targeted therapies are now standard of care, whereas others are currently being evaluated in clinical trials for a host of mutations associated with NSCLC. 11 These therapies are most often used in addition to traditional platinum-based chemotherapy either as adjuvant treatment after resection or as primary treatment in those with unresectable or metastatic disease.
List of Targetable Mutations and Treatment Recommendations for Locally Advanced or Metastatic Non-Small Cell Lung Cancer, According to National Comprehensive Cancer Network, Non-Small Cell Lung Cancer (Version 3.2024) (2024)
The epidermal growth factor receptor (EGFR) is a receptor tyrosine kinase that activates downstream pathways involved in cell proliferation and angiogenesis. 12 EGFR is mutated in approximately 10% of lung adenocarcinoma and more frequently in younger female never-smokers. 13 In the 1990s, the oral first-generation EGFR inhibitor gefitinib was given along with cytotoxic chemotherapy to an unselected cohort of patients with NSCLC. When only 10% of the patients exhibited a positive response to treatment, it was retrospectively determined that the responders all had a mutation in the EGFR receptor.14–17 This confirmed the efficacy of targeted therapies acting against a specific genetic mutation. Today, third-generation EGFR inhibitor osimertinib has proven effective against EGFR-positive NSCLC resistant to earlier-generation EGFR inhibitors and demonstrates significantly improved overall and disease-free survival compared with platinum-based chemotherapy alone.18,19 Given its superiority in the ADAURA and FLAURA trials over other EGFR inhibitors, osimertinib has since become the first-line standard of care for both resected and unresectable EGFR-positive NSCLC.20–22
Anaplastic lymphoma kinase (ALK) is targetable genetic mutation seen in about 2%–7% of lung adenocarcinoma.23–25 Crizotinib was the first ALK inhibitor shown to be effective against NSCLC in 2010, demonstrating significantly improved survival in ALK-positive NSCLC over chemotherapy alone.26–28 Subsequent studies have shown increased efficacy and improved survival of second-generation ALK inhibitors alectinib, brigatinib, ceritinib, and lorlatinib, which are all now first-line therapies for ALK-positive NSCLC.22,29–32
Further targetable mutations in NSCLC include ROS1, rearranged during transfection (RET), and mesenchymal epithelial transition (MET). Although alterations in these receptor tyrosine kinases are seen in only a small percentage of lung adenocarcinoma, trials investigating new or existing targeted therapies have demonstrated positive outcomes. ROS1 has a similar molecular structure to ALK, and subsequent studies have shown that ALK inhibitors, crizotinib, ceritinib, lorlatinib, as well as ROS1-specific entrectinib, have all demonstrated activity against ROS1-positive NSCLC.33–36 A host of multi-targeted tyrosine kinase inhibitors (TKIs) are being studied for RET fusion-positive NSCLC, and to date, selpercatinib has demonstrated efficacy and prolonged survival in advanced disease. 37 MET is a receptor tyrosine kinase that may be overexpressed, amplified, or activated in NSCLC. 38 Patients with MET mutations or high levels of MET amplification (∼4% of adenocarcinoma and ∼1% squamous cell carcinoma) may benefit from MET inhibitors, crizotinib, capmatinib, or tepotinib.39–41
Human epidermal growth factor receptor-2 (HER2) is a receptor tyrosine kinase within the EGFR family and is found to be mutated in 2%–4% of NSCLC. 42 Similar to EGFR, HER2 mutations are mostly seen in female never-smokers with adenocarcinoma. Although trastuzumab, a HER2 monoclonal antibody, has revolutionized treatment of HER2-positive breast cancer, trials of trastuzumab and chemotherapy for treatment of NSCLC had disappointing results. 43 However, trastuzumab–deruxtecan, an antibody-drug conjugate in which the anti-HER2 monoclonal antibody delivers a topoisomerase I inhibitor directly to cancer cells, has produced durable responses to HER2-positive NSCLC. 44
BRAF is a protein kinase found to be mutated in about 3%–5% of NSCLC, more frequently in smokers with adenocarcinoma.45,46 Approximately, half of patients with a BRAF mutation have an activating Val600Glu (V600) mutation. Both vemurafenib and dabrafenib, two selective inhibitors of BRAF (V600), have shown improved survival in patients with BRAF (V600)-mutated melanoma and were subsequently shown to have activity and improved survival in BRAF (V600)-mutated NSCLC.47,48 A subsequent study demonstrated an even higher response rate when dabrafenib was combined with the MEK inhibitor trametinib. 49
KRAS is a GTPase that helps regulate the cell cycle and is found to be mutated in 25%–30% of lung adenocarcinomas and about 5% of squamous cell carcinomas, with mutations more frequently seen in smokers. 50 Until recently, KRAS had few viable treatment options. However, in the past 2–3 years, sotorasib and adagrasib have emerged as treatment for KRAS-mutated NSCLC. Both are small molecule inhibitors that selectively and irreversibly bind KRAS in its inactive state and have been shown to have durable clinical benefit for patients who have failed initial treatment.51,52
Finally, mutations in the tumor suppressor gene TP53 (tumor protein 53) are seen in about 46% of lung adenocarcinoma and almost 90% of lung squamous cell carcinoma. 53 The presence of a TP53 mutation is associated with worsening histological grade, hinting at the gene’s role in tumor progression, and is associated with significantly worse outcomes compared with NSCLC without a TP53 mutation. 54 Unfortunately, despite the significant fraction of NSCLC that harbors a TP53 mutation, there is currently no effective targeted therapy for TP53, and this remains a frontier of active exploration.
Molecular-targeted therapy holds enormous potential for those with targetable genetic mutations. This has been reflected in National Comprehensive Cancer Network (NCCN) recommendations, which strongly advise testing for EGFR and ALK in all patients before initiation of neoadjuvant or adjuvant chemotherapy. 22 However, only about 25% of NSCLC harbors a targetable genetic mutation. Very few patients with squamous cell carcinoma are candidates for targeted therapy. Furthermore, although many patients may show a striking initial response to targeted therapy and increased survival compared with traditional chemotherapy alone, resistance to targeted therapy develops almost universally.
Immune checkpoint inhibition
In parallel to the development of molecular-targeted therapies, great strides have been made in the development of therapies that allow the body’s own immune system to identify and destroy cancer cells. During tumorigenesis, abnormally high expression of programmed death-ligand 1 (PD-L1) on cancer cell membranes leads to binding with the programmed death-1 (PD-1) receptors of T-lymphocytes. This bond leads to downstream inhibition of T-lymphocyte activation, allowing tumor cells to grow and metastasize unchecked by the host immune system.55,56 Immune ICIs prevent the tumor from inactivating the host immune response, allowing T-cells to target growing cancer cells (see Fig. 1). 57 The identification of these pathways and the development of ICIs has ushered in the modern era of immunotherapy in the treatment of cancer. To date, antibody-mediated therapies which aim to disrupt the binding of PD-1 to PD-L1 have demonstrated striking success in a variety of different cancers.58–60 Nivolumab, a human IgG anti-PD-1 monoclonal antibody, was the first such therapy used in NSCLC, which resulted in increased survival in both lung squamous cell carcinoma and adenocarcinoma that had failed first-line cytotoxic chemotherapy treatment.61,62 Shortly thereafter, pembrolizumab (humanized anti-PD-1 IgG), atezolizumab (humanized anti-PD-L1), and durvalumab (human IgG anti-PD-L1) demonstrated similar success.63–65
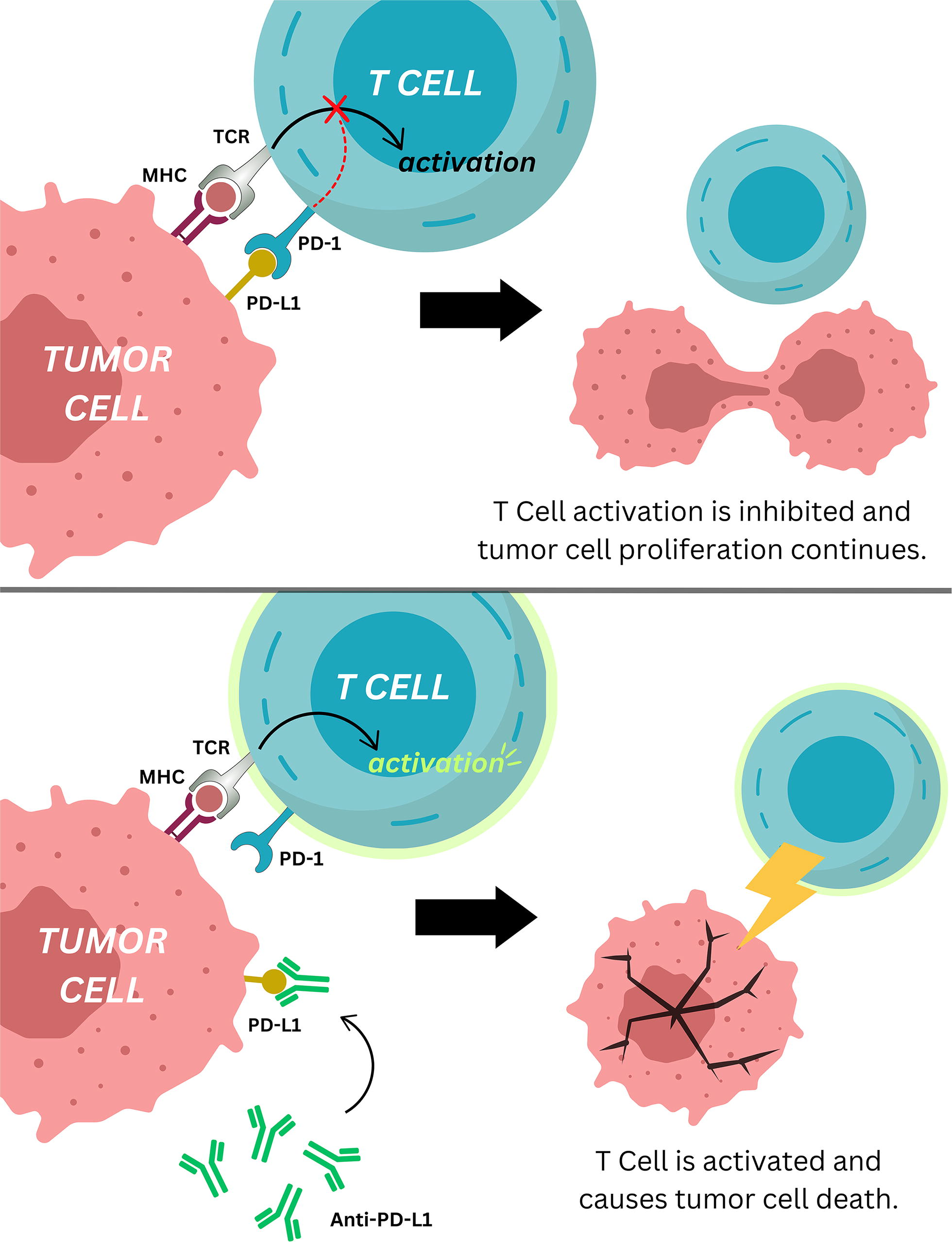
Representation of the mechanism of action of anti-PD-L1, an immune checkpoint inhibitor. MHC, major histocompatibility complex; PD-L1, programmed death-ligand 1; TCR, T cell receptor.
Pembrolizumab was then investigated as a first-line treatment. In patients whose tumors exhibited >50% PD-L1 expression, survival was significantly longer when treated with pembrolizumab when compared with traditional platinum-based chemotherapy. 66 Tumors with lesser degrees of PD-L1 expression still demonstrated a positive effect with ICI; however, this was not necessarily better than traditional chemotherapy. 67 High tumor mutational burden (TMB) came to be recognized as a marker indicative of positive response to ICI, as tumors with more mutations produce more neoantigens that can be recognized by the host immune system. 68 This theory was supported by improved survival in a subset of patients with PD-L1 expression >50% and high TMB with first-line nivolumab compared with chemotherapy, even while those with lower PD-L1 expression did not derive a similar survival benefit. 67
A host of recent trials have subsequently examined the effect of ICI in combination with cytotoxic chemotherapy, with significantly improved outcomes.65,69–76 The impact of these trials is reflected in the NCCN guidelines, which encourage testing for tumor PD-L1 status in all patients before initiation of neoadjuvant or adjuvant chemotherapy and strongly recommend ICI in addition to chemotherapy for all eligible patients. 22 Although most of these trials and guidelines pertain to patients with advanced or metastatic NSCLC, there is also promising work investigating the utility of ICI in the neoadjuvant setting.
It is important to note that, despite promising results, NSCLC eventually develops resistance to ICI. 77 The mechanisms by which resistance develops and the development of drugs to circumnavigate them remain an area of active investigation.
Neoadjuvant Therapy
For patients with resectable NSCLC, the long-standing paradigm has been to proceed directly to surgery with postoperative adjuvant chemotherapy. However, this paradigm is changing. When used in the preoperative setting, chemotherapy may be able to downstage tumors and target early micrometastatic disease.78,79 In addition, complete pathological response to neoadjuvant therapy serves as a potent indicator of favorable prognosis. 80 NCCN guidelines now recommend evaluation for neoadjuvant therapy in locally advanced disease. 22 However, the overall magnitude of benefit for neoadjuvant chemotherapy is small, demonstrating only 5%–6% increase in overall survival at 5 years. 79 However, as ICIs and targeted therapies have demonstrated efficacy in certain populations of patients with NSCLC, there have been numerous recent trials with positive results exploring these therapies in the neoadjuvant setting.
It is hypothesized that preoperative immune checkpoint inhibition allows for the immune system to recognize a greater number of tumor neoantigens, increasing the efficacy of the immune system’s ability to attack tumor cells. 81 A series of early heterogenous trials investigating the neoadjuvant use of various ICIs, both with and without neoadjuvant chemotherapy, demonstrated mixed results when comparing progression-free and overall survival. However, a significant fraction of patients in each trial demonstrated major pathological response to neoadjuvant ICI on final analysis of resected cancers.6,82–86 To this end, there have been several phase III randomized controlled trials investigating the use of neoadjuvant immune checkpoint inhibition.
The CheckMate 816 trial, published in April 2022, studied the use of three cycles of neoadjuvant nivolumab (anti-PD-1 antibody) plus chemotherapy compared with three cycles of neoadjuvant chemotherapy alone before surgical resection for patients with stage IB to IIIA NSCLC. Almost 360 patients were randomized. There was found to be a significantly longer event-free survival in patients who received neoadjuvant nivolumab (>30 months, compared with about 20 months). It also found that 24% of patients who received nivolumab experienced a pathological complete response, with no evidence of tumor in the resected specimen, compared with 2.2% in the chemotherapy-alone group. 87
The KEYNOTE-671 trial was run simultaneously to CheckMate 816 and published in June 2023. This trial was larger, with just under 800 patients randomized. In contrast to the Checkmate 816 trial, KEYNOTE-671 administered pembrolizumab (anti-PD-1 antibody) with chemotherapy preoperatively and then administered adjuvant pembrolizumab for nine months postoperatively. Similar to CheckMate 816, the arm receiving perioperative ICI and neoadjuvant chemotherapy demonstrated improved event-free survival, major pathological response, and pathological complete response compared with the neoadjuvant chemotherapy-alone arm. The hazard ratio (HR) for event-free survival in KEYNOTE-671 was 0.69, which, when compared with CheckMate 816’s HR of 0.84, cautiously supports the assertion that the addition of adjuvant ICI to neoadjuvant ICI may lead to longer event-free survival. 88
The AEGEAN trial, published in October 2023, studied the use of perioperative durvalumab (anti-PD-L1 antibody) in combination with neoadjuvant chemotherapy. This trial was similar in size (about 800 patients enrolled) and study design to KEYNOTE-671, with largely similar findings. There was again seen a significant event-free survival benefit, as well as a significantly larger proportion of patients who had a major pathological response and complete pathological response with ICI when compared with patients who received neoadjuvant chemotherapy alone. The event-free survival HR in AEGEAN was 0.68, comparable with the HR of 0.69 seen in KEYNOTE-671. 89 Finally, we are awaiting the results of the ongoing IMpower030 trial, investigating the use of neoadjuvant atezolizumab (anti-PD-L1 antibody) plus chemotherapy in NSCLC. 90 Taken together, these trials support the use of perioperative immune checkpoint inhibition in the treatment of resectable NSCLC, and the NCCN now recommends that all patients diagnosed with resectable NSCLC be tested for PD-L1 status and be evaluated for potential neoadjuvant therapy. 22
As neoadjuvant ICIs have become increasingly common, a new challenge arises when evaluating the effect of neoadjuvant immune therapy before resection. Restaging CT scans frequently demonstrate persistent or enlarged tumor mass after immune checkpoint inhibition. 81 PET scans may even indicate persistent hypermetabolic tumor activity. 91 However, once resected, many of these tumors were indeed found to have had a major pathological response to ICI, and several with no evidence of residual tumor. 82 The persistent or enlarged tumor size on imaging after neoadjuvant ICI is thought to reflect an initial tumor expansion secondary to T-cell infiltration in response to immune activation, termed a “tumor flare.” 92 Similarly, the radiographic appearance of worsening lymph node involvement after ICI has been called a “nodal immune flare.” 93 As neoadjuvant ICI becomes increasingly common, new algorithms will be required to accurately restage patients before undergoing surgical resection.
The optimal timing of surgery following neoadjuvant ICI is not yet clear. Broadly, it is recommended that patients treated with neoadjuvant platinum-based chemotherapy or chemoradiotherapy undergo resection within 6–8 weeks of the completion of therapy to avoid potential fibrosis and to minimize the risk of potential disease progression.94,95 However, in the CheckMate 816 trial, surgery was performed within 6 weeks of neoadjuvant treatment, whereas the KEYNOTE-671 trial performed surgery no later than 20 weeks after the first dose of neoadjuvant therapy. One small retrospective study suggested that the time interval between completion of neoadjuvant ICI and surgery did not affect the duration of surgery, extent of bleeding, length of hospital stay, or rate of complete pathological response. 96
As surgeons see more patients who have received immune therapy before anatomical resection, it is important to understand the potential effects of these treatments on intraoperative findings. Most reports suggest comparable complication rates between patients receiving neoadjuvant ICI and those receiving upfront chemotherapy or chemoradiotherapy. However, some surgeons have observed increased inflammatory changes around lymph nodes after immunotherapy, at times associated with fibrotic adhesions or hypervascularity, which may be particularly significant at the pulmonary hilum. As such, several initial reports of surgery after ICI suggest a significantly higher rate of conversion from minimally invasive resection to thoracotomy. 6
The use of neoadjuvant molecular-targeted therapy is still in its infancy. However, early reports suggest that TKIs, such as third-generation EGFR inhibitor osimertinib, may be useful in the neoadjuvant setting. In the ADAURA trial, osimertinib was given with chemotherapy as adjuvant treatment and showed a significant reduction in the risk of disease recurrence or death for resected, EGFR-mutated NSCLC. 20 This prompted the ongoing NeoADAURA trial, a phase III multicenter randomized clinical trial that aims to evaluate the efficacy of neoadjuvant osimertinib. It has three arms: one utilizing neoadjuvant osimertinib as monotherapy, one with neoadjuvant osimertinib in combination with neoadjuvant chemotherapy, and a control group of neoadjuvant chemotherapy alone in patients with resectable, EGFR-mutated NSCLC. All patients can then proceed to surgery and receive optimal adjuvant treatment (including adjuvant osimertinib). 97 Although the use of TKIs is not yet broadly approved in the neoadjuvant setting, they may hold significant promise for patients with EGFR mutations in the treatment of NSCLC.
Current studies are investigating the effects of combining platinum-based cytotoxic chemotherapy with concurrent ICI/TKI therapy to determine whether these combinations may lead to better outcomes than the use of either therapy alone. 98 Further trials will elucidate whether combined therapy has the potential to improve therapeutic response through multiple synergistic mechanisms.
Adjuvant Immune Checkpoint Inhibition
Following resection, adjuvant therapy should be considered for all patients with pathological evidence of lymph node metastasis and for those with a larger primary tumor, with the primary objectives being mitigation of micrometastatic disease and limiting the risk of recurrence. The Lung Adjuvant Cisplatin Evaluation meta-analysis suggested that adjuvant cisplatin-based chemotherapy after complete resection was associated with a 5.4% overall survival benefit for those who receive adjuvant chemotherapy, with the effects being statistically significant in patients with lymph node metastasis. 3 However, these data date back to 2004, and until the advent of ICI, there had been relatively little progress in systemic therapy for NSCLC. The results of the MAGE-A3 Trial, a randomized and double-blinded study comparing adjuvant immune therapy after complete resection to placebo, were reported in 2016. This study did not demonstrate benefit in either disease-free or overall survival with adjuvant immunotherapy. 99 However, the advent of ICIs represents a significant evolution in the adjuvant management of NSCLC. ICIs have been studied as single agents and in concert with platinum-based therapy. 100 When initially studied in metastatic and locally advanced NSCLC, there was a benefit in both overall and progression-free survival.
The Impower010 trial is a randomized, multicenter, phase III trial that included patients with resected stage 1B (tumor >4 cm) to IIIA NSCLC. 101 Just over 1000 individuals met inclusion criteria, with 507 randomized to receive the PD-L1 inhibitor atezolizumab. In patients with tumors with >1% PD-L1 expression, atezolizumab was associated with a significant improvement in disease-free survival when compared with supportive care (HR 0.66, 95% confidence interval [CI] 0.5 to 0.88, P = .004). This was followed by an American Society of Clinical Oncology update that recommended adjuvant systemic atezolizumab for patients with a PD-L1 >1% without an EGFR mutation following cisplatin-based chemotherapy. 102 This was subsequently supported by Food and Drug Administration (FDA) approval of atezolizumab as an adjuvant treatment for NSCLC.
A number of studies examining checkpoint inhibitors are actively ongoing. Pembrolizumab, a PD-1 inhibitor, was compared in the adjuvant setting in individuals with stage IB/II-IIIA following complete resection in the KEYNOTE-091 trial. 103 This demonstrated that disease-free survival was improved in the pembrolizumab cohort relative to those who received a placebo (median 53.6 months vs. 42.0 months) with a HR of 0.76. 103 Nivolumab, another PD-1 inhibitor, is being examined in the ANVIL study to evaluate impact on overall and disease-free survival in patients with stage IB-IIIA NSCLC. 104
Immune Checkpoint Inhibition in Recurrent NSCLC
NSCLC may progress or recur despite initial management with chemotherapy, targeted therapy, immune therapy, or surgery. In this setting, management has historically relied upon platinum-based cytotoxic chemotherapy, with median survival (MS) of around 1 year. 105 In 2012, a phase I study evaluating nivolumab in individuals with recurrent or advanced NSCLC found that it was safe and potentially effective. 57 This was followed by data from the phase II CheckMate 063 trial, in which 117 participants with advanced NSCLC were treated with nivolumab. This study demonstrated that 14.5% of patients demonstrated an objective response with 26% of patients having stability of disease. 106 In comparison of nivolumab with docetaxel, the CheckMate 057 randomized, phase III study resulted in an increase in MS (9.2 vs. 6.0 months) but found that PD-L1 expression did not appear to have either a predictive or prognostic benefit. 62 Finally, the phase III CheckPoint 017 trial was able to demonstrate that in the setting of stage IIIB/IV NSCLC that progressed despite chemotherapy, MS in the nivolumab group was 12.2 months compared with 9.4 with docetaxel, and evaluation of progression-free survival remains ongoing. 107 In addition, CheckPoint 017 demonstrated that the degree of PD-L1 in tumor cells does correlate with increased efficacy of nivolumab across all categories when compared with docetaxel. Nivolumab also had a treatment-related adverse event (AE) rate of 10% in comparison with 54% with docetaxel. 107
The safety and efficacy of pembrolizumab were assessed in the phase I KEYNOTE-001 study, released in 2019. This evaluated pembrolizumab in 1260 individuals with either advanced stage or previously treated and recurrent NSCLC. It was found to demonstrate that a dose of 2 mg/kg of pembrolizumab resulted in an overall risk reduction of 15% in patients with previously treated and advanced NSCLC. 108 This was followed by the KEYNOTE-010 trial of 1034 patients that compared pembrolizumab to docetaxel in patients with previously treated and advanced NSCLC, with a PD-L1 expression rate of at least 1%. MS was improved compared with docetaxel with a HR of 0.71, but there was no statistically significant difference in progression-free survival compared with docetaxel. However, in individuals who expressed at least 50% PD-L1, pembrolizumab was found to result in a statistically significant difference in progression-free survival. 63 Pembrolizumab was subsequently approved by the FDA for use in individuals with advanced or recurrent PD-L1-positive NSCLC with worsening disease following chemotherapy. In the phase III KEYNOTE-024 trial, pembrolizumab was found to result in improved progression-free survival compared with chemotherapy (10.3 vs. 6.0 months, HR 0.50) and overall survival (HR 0.60). 66 The pembrolizumab group also demonstrated a 44.8% response rate in contrast to 27.8% in those receiving chemotherapy. 66 AEs were found to occur ∼30% less frequently with pembrolizumab and resulted in FDA approval of pembrolizumab as a first-line treatment in advanced or recurrent NSCLC. 66
In patients who were previously treated with chemotherapy, atezolizumab-based immune therapy improved overall survival compared with docetaxel (12.6 versus 9.7 months, HR 0.73) in the POPLAR phase II trial. Atezolizumab was also found to have a 28% reduction in AEs associated with treatment. This resulted in FDA approval of atezolizumab in management of advanced or recurrent NSCLC in individuals previously treated with chemotherapy and with PD-L1 positive tumors. Moving forward, a discussion regarding the indication and role of immune therapy in the specifically recurrent NSCLC population is warranted.
Tumor-Targeting Guidance
Notwithstanding the major advancements in the development of novel medical therapies in recent years, surgery remains the cornerstone of treatment in NSCLC. Surgical resection is not only offered upfront as definitive treatment for early-stage disease but also has a role in specific cases of advanced disease. 22 However, surgical resection has significant risks, and postoperative long-term recurrence rates after lung cancer surgery remain high. Two large-scale studies have reported recurrence rates as high as 36% and 41.5% for patients undergoing curative-intent surgery for NSCLC, though the exact reason for recurrence is not fully understood. The main goal of curative-intent surgery is to achieve an “R0” resection, the resection of the entirety of diseased tissue with margins that are free of disease. This can be challenging for surgeons relying on preoperative imaging and visual or tactile cues to identify lesions intraoperatively to determine appropriate resection margins. This becomes an almost impossible task in cases of nonpalpable, small or deep tumors.
Operative adjuncts that aid in localizing tumors intraoperatively have been developed to help surgeons achieve R0 resections, including preoperative wire localization and injection of dyes or radioisotopes. However, these procedures impose additional risks to patients, they are limited by tumor location and size, and they have high failure rates. Furthermore, these techniques do not provide benefit in identifying microscopic disease in resection margins in real time. This has significant implications in operative outcomes, as patients whose resected tissue is later found during pathological evaluation to have microscopic disease in the margins, deemed an “R1” resection, have 5-year survival rates that can be as low as 14%. Thus, there has been a recent drive to develop intraoperative tools to help achieve R0 resections and improve on these surgical shortcomings. One of the tools that has seen significant growth fueled by advancements in tumor-targeting is intraoperative molecular imaging (IMI).
IMI involves the intravenous administration of a fluorescent contrast dye that accumulates in malignant tissue and is then detected by wavelength-specific cameras intraoperatively. Initially, this intraoperative imaging guidance was limited to nontargeted dyes such as indocyanine green or methylene blue, which accumulate within tumors given the increased vascularity and permeability of malignant tissues, lending the name often used to refer to this modality as “structural” or “functional” fluorescent imaging. However, with the advent of tumor-targeting techniques, new dyes that bind to specific membrane receptors on tumor cells have been developed. This is achieved by conjugating a tumor-targeting molecule with a fluorophore.
The dyes are injected preoperatively, anywhere from 30 minutes to several days before surgery, and as the unbound dye is cleared from tissues, the remaining dye that is bound to malignant cells will emit wavelength-specific fluorescent light that can be detected intraoperatively by specialized cameras and guide surgeons in their resection real time (see Fig. 2). 8 The targeting molecules bind to receptors that are known to be overexpressed in some lung cancers, such as folate receptor alpha (FRα) and carcinoembryonic antigen (CEA). Some examples of these dyes include folate-fluorescein and pafolacianine, folate-conjugated fluorescent compounds that bind FRα, and anti-CEACAM5-conjugated fluorochrome (SGM-101), which is a chimeric monoclonal antibody against CEA conjugated with a fluorescent compound. 8

Many of these dyes are still in clinical trials, and no large-scale studies have been performed to help guide surgeons in the selection of appropriate dyes for specific patient populations, but studies looking at the efficacy of IMI in aiding identification of tumors and appropriate resection margins are promising. Pilot studies have demonstrated that folate-conjugated dyes have a sensitivity of ∼96% for pulmonary adenocarcinoma and up to 70% in squamous cell carcinoma. IMI also allows surgeons to identify nonpalpable lesions that would otherwise be undetectable via traditional visual and tactile inspection. In these cases, use of IMI can spare patients from conversion to a highly morbid thoracotomy after inability to locate the lesions using minimally invasive techniques. 8 Furthermore, one of the greatest advantages of IMI is the ability to detect subcentimeter synchronous lesions that were not previously detected by PET-CT during initial workup. 8 Once the specimen is excised, IMI can also be used on the back table to look at the resection margins. Using specialized microscopes to evaluate the specimen in real time helps detect any microscopic disease in resection margins or to measure the distance from the malignant tissue to the staple line with great accuracy. In fact, the distance measured from the edge of the fluorescent signal to the staple line by use of IMI has been seen to be nearly identical to the margins reported on final pathology. 8
Though further studies are required before these techniques can be more widely accepted and routinely used in surgical resections, the use of IMI seems to be a promising prospect in optimizing the surgical treatment of NSCLC.
Liquid Biopsy Surveillance
The surest way to improve survival in NSCLC is earlier diagnosis and treatment. Patients diagnosed with stage IA or IB resectable NSCLC have >50% 5-year survival, whereas those diagnosed with stage IIIB disease or worse have <10% 5-year survival. To this end, the U.S. Preventative Services Task Force recommends an annual volume-based low-dose lung CT scan for individuals between ages 50 and 80 with a 20-pack-year smoking history. This recommendation is supported by evidence from the National Lung Screening Trial and the NELSON trial, which found an overall mortality risk reduction between 20% and 25% for high-risk populations screened with low-dose lung CT. However, there are significant limitations to routine use of low-dose lung CT screening. Even in best-case clinical trials, the false positive rate was between 9% and 20%, leading to invasive biopsies for benign lung nodules. It exposes patients to repeated doses of ionizing radiation. Moreover, only about 25% of patients diagnosed with lung cancer every year meet the high-risk screening criteria, leaving a large fraction of the population without any effective screening method.
Liquid biopsy surveillance can help detect lung cancer at an earlier stage and mitigate the shortcomings of CT surveillance. In this technique, a blood sample from the patient can be analyzed for various cancer-associated biomarkers, most commonly circulating tumor DNA (ctDNA). This sample can then be analyzed via polymerase chain reaction or, increasingly, next-generation sequencing, allowing hundreds to thousands of genes to be sequenced in parallel to detect NSCLC-associated genetic mutations. 7
Patients with NSCLC have been found to have significantly higher levels of cell-free DNA in their blood stream compared with cancer-free controls. This is mostly driven by fragments of ctDNA derived from tumor cells, suspected to be released into the bloodstream secondary to tumor necrosis and/or apoptosis. The quantity of ctDNA in the bloodstream correlates with tumor burden. In a small cohort, circulating tumor DNA was detectable in 50% of patients with stage I NSCLC and 100% of patients with stage II-IV NSCLC. In the TRACERx trial, ctDNA could be detected 6–12 months before when a radiographic diagnosis of NSCLC could be made. Although plasma ctDNA is not sensitive enough to make the diagnosis of NCSLC alone, it may have applications in early screening that could prompt further workup. When used in combination with lung CT screening, it can reduce excessive radiation exposure and complications related to the high false-positive rate of lung CT screening. 7
Liquid biopsy has significant potential to help guide personalized NSCLC treatment. Currently, plasma ctDNA analysis is recommended in the NCCN guidelines as a complimentary test, along with tissue biopsy, to help identify targetable genetic mutations. 22 Given the heterogeneity of NSCLC tumors, it can help identify targetable mutations that were not present in a small tissue biopsy sample. It may be used to guide therapy in patients who are medically unfit for an invasive biopsy or for patients whose tumors are in an anatomically high-risk location for biopsy. In patients with early-stage, resected disease, it may help to guide adjuvant treatment. Liquid biopsies can also be used to monitor response to treatment, with decreasing ctDNA burden reflecting positive treatment effect before radiographic changes are observed. Long-term liquid biopsy surveillance for patients who have completed treatment for NSCLC may help to detect tumor recurrence early, allowing patients to initiate second-line treatment before their disease becomes widely metastatic and symptomatic. Finally, disease monitoring with liquid biopsy for patients taking adjuvant targeted therapies may help to identify when their cancer develops resistance, allowing modification of a long-term treatment regimen. Although liquid biopsy surveillance is not yet incorporated into standard treatment guidelines, it has valuable potential as a long-term cancer surveillance tool.
Conclusion
NSCLC remains the leading cause of cancer-related death worldwide and, historically, has had poor overall survival. However, in the past two decades, there has been an explosion in our understanding of the complex cellular and genetic underpinnings of the disease. A recognition of various genetic mutations has allowed for the development of targeted therapies, drugs that directly inhibit tumor growth by binding to mutated tumor receptors. Many of these drugs, especially those that inhibit EGFR and ALK, have become standard of care in the treatment of EGFR- and ALK-positive NSCLC and have demonstrated remarkably improved survival. Simultaneously, ICIs such as nivolumab and pembrolizumab have been shown to successfully interfere with the PD-1/PD-L1 pathway by which NSCLC tumor cells evade the host immune system, allowing the host’s T-cells to attack growing tumor cells. This has repeatedly been shown in trials to significantly prolong patient survival.
The increasing use of these therapies has revolutionized the way we treat NSCLC. Recent trials have shown that immune checkpoint inhibition, and increasingly targeted therapy, can be utilized in the neoadjuvant setting to downstaging tumors and help to control micrometastatic disease early. Their incorporation in the adjuvant setting has also been shown to mitigate micrometastatic disease and improve overall and disease-free survival compared with historical cytotoxic chemotherapy. Patients with recurrent NSCLC now have increased treatment options, with ICIs such as pembrolizumab and nivolumab showing prolonged survival compared with the historical second-line agent docetaxel.
New intraoperative imaging technologies are on the horizon to help surgeons perform increasingly focused minimally invasive resections. IMI uses tumor-binding dyes to allow surgeons to identify lung lesions intraoperatively, affording a greater chance at performing a minimally invasive R0 resection.
The increasing use of liquid biopsies, in which a simple blood draw is analyzed for circulating tumor DNA, is increasingly allowing for early and extensive genetic analysis of patients’ NSCLC. This promising technology has broad future applications, including as an adjunct to lung cancer screening CT scans in high-risk populations and in the earlier diagnosis and treatment of the disease. It also has promising roles in long-term recurrence surveillance and as an early marker of developing resistance in patients taking suppressive maintenance immune therapy.
In summary, recent advances in the understanding of the cellular and genetic underpinnings of NSCLC and the associated advances in therapy highlight the exciting and ever-changing landscape of NSCLC treatment.
Footnotes
Authors’ Contributions
R.W.C.Y.: Investigation; writing—original draft; writing—reviewing and editing; visualization. G.R.R.: Investigation; writing—original draft; writing—reviewing and editing; visualization. J.K.: Investigation; writing—original draft; writing—reviewing and editing; visualization. D.C.: Investigation; writing—original draft; writing—reviewing and editing; visualization. G.D.T.: Conceptualization; supervision; project administration; writing—reviewing and editing. J.L.A.: Conceptualization; investigation; project administration; supervision; writing—original draft; writing—reviewing and editing.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.