
Abstract
Indocyanine green (ICG) is an inert polypeptide that almost totally binds to high molecular weight plasma proteins; it is cleared by the hepatocytes and directly excreted into the bile with a half-life of about 3–5 minutes. Specific systems are required to see fluorescent images. The use of this dye has been reported in different surgical specialties, and the applications in hepatobiliary surgery are widening. Being firstly used to evaluate the preoperative liver function, intra- and postoperative dynamic checking of hepatic activity has been reported and integrated within perioperative protocols allowing a tailored treatment allocation. Intravenous injection (IV) or injection into the gallbladder can ease difficult cholecystectomy. Biliary leakage detection could be enhanced by IV ICG injection. Although with some contrasting results, the use of ICG for both delineating the limits of the resection and tumor-enhanced visualization was demonstrated to improve short- and long-term outcomes. Although the lack of strong evidence still precludes the introduction of this tool in clinical practice, it harbors great potential in liver surgery.
Introduction
Indocyanine green (ICG) is an inert, tricarbocyanine organic anion‐transporting polypeptide. It almost totally binds to high molecular weight plasma proteins, including albumin, alpha 1-, and beta-lipoproteins. The protein structure is not altered, and, consequently, intravenous (IV) toxicity is avoided. Because it contains iodine, ICG administration should be avoided in the presence of thyrotoxicosis or iodine allergy; otherwise, adverse reactions are rare (1 every 40000 people). 1
In the serum, the ICG has excitation and emission wavelengths of 778 and 830 nm, respectively. This wavelength excited by near-infrared (NIR) light is not visible to the human eye; therefore, fluorescence images are obtainable through ICG fluorescence systems equipped with interferential filters.
ICG was approved for medical use by the Food and Drug Administration in 1957, and ICG fluorescence imaging gained great attention in various procedures of different surgical specialties, that is, to detect the lymphatic flow in the extremities, the sentinel lymph nodes in breast or gastrointestinal cancers, to evaluate blood flow during coronary artery bypass grafting, or clipping cerebral artery aneurysms. 2 Since the 1980s, ICG has been used in hepatobiliary operations for several purposes, including perioperative hepatic function assessment or to identify segmental boundaries, bile ducts, and liver cancers, especially in cirrhotic livers. 3 In open surgery, standard lights should be switched off to see the fluorescence, and a NIR camera is needed forcing the surgeon to look away from the operative field and to put down the surgical instruments. In laparoscopic surgery, the NIR camera is integrated in the great majority of the systems providing fluorescence imaging or, in the most recent systems, a superimposed imaging of the fluorescence over the operative field. The FireflyTM camera (Intuitive, Sunnyvale, CA, USA) is integrated into the da Vinci Surgical Systems (Intuitive, Sunnyvale, CA, USA) and can easily be used to intraoperatively visualize ICG accumulation. The simplicity of use of the last two systems caused the great expansion of the use of ICG and the studies behind it.
This review aims to describe the actual state of the art of the use of ICG in hepatobiliary surgery providing practical information for educational purposes or routine daily use in different perioperative steps, laying the foundation for future applications and further developments of this useful tool.
Hepatic Function Assessment
Since posthepatectomy liver failure (PHLF) represents a dreadful event, the preoperative assessment of liver function or the early recognition of this complication is crucial, especially after extended resection or in cirrhotic patients.
The assessment of liver function was the first use of ICG in liver surgery. After IV injection of 0.5 mg/kg of the dye, ICG bound to plasma proteins is cleared by the hepatocytes and directly excreted into the bile having a half-life of about 3–5 minutes. The ICG is not subjected to metabolism or enterohepatic circulation. 1 Consequently, the ICG retention rate after 15 from administration (ICG-R15) and the ICG plasma disappearance rate (ICG-PDR) can reflect liver function.
The introduction of the LiMONTM (Pulsion Medical Systems, Munich, Germany) and the DDG 2001 (Nihon Kohden, Japan) systems, which allow the measure of ICG clearance through pulse spectrophotometry in less than 10 minutes, made this assessment even simpler. 1 Therefore, using the ICG clearance test is still reported in several guidelines recommending patient management, especially in Asian communities.4,5 The Makuuchi algorithm suggests the tolerable extension of the liver resection considering the ICG retention test (Fig. 1). 6

Makuuchi algorithm 6 for the cirrhotic patient decision-making process.
Several authors confirmed the predictive value of this test5,6 and its better performance in prognosticating postoperative liver failure when compared with the Child or MELD score. 7
However, this algorithm was empirically developed almost three decades ago by evaluating only a few patients. 8 Other models have been suggested. 9 For example, the Albumin Indocyanine Green Evaluation (ALICE), further integrated with the measurement of portal hypertension in the subgroup of intermediate-risk patients (ALICE grade 2), has been proposed for patients undergoing surgery for hepatocarcinoma (HCC). 10
The ICG test results corrected for the future liver remnant volume were also proposed.11–14 Kobayashi et al. reported that the ICG clearance of the remnant liver could predict the development of subclinical postoperative liver failure in patients undergoing liver resection for both HCC and metastases with high sensitivity. The authors proposed a cutoff value of 0.05, above which no life-threatening postoperative liver failure was ever seen.13,14 Between 0.05 and 0.10, subclinical postoperative liver failure could be observed, and therefore, corrective measures should be applied. 14 However, this evaluation presumes a similar function within all the liver parenchyma, but cholestasis or portal thrombosis may impair the function of different liver areas. 15
In the field of transplantation surgery, the results of the ICG clearance test of brain dead donors well correlate with graft availability and survival. 16 Asencio et al. recently proposed a cutoff value of 10% for ICG-PDR measured in brain dead donors immediately before organ procurement. This value proved to identify livers that were further discarded. 17 ICG tests also exhibited the capacity to predict the quality of the graft during ex situ normothermic perfusion. 18 Although further studies are needed, this finding may help in reducing unnecessary efforts and costs.
Dynamic intraoperative ICG clearance evaluation is another possibility in predicting PHLF. Although actual data are scarce and probably not sufficient to suggest a modification of the preoperative surgical plans, this assessment may be promising. 19 Thomas et al. performed an intraoperative evaluation of ICG test values before and after selectively clamping the arterial and portal pedicles of the segments to be resected comparing them with those before abdominal closure. The authors found this intraoperative assessment as a feasible and valuable tool in the case of anatomical resections, though with some limits, mostly hyperbilirubinemia and intraoperative fluctuation of liver perfusion. 20 Sato et al. performed a similar study evaluating the concordance between intraoperative ICG-PDR in predicting PHLF, which was .834 and even higher (.923) in the subgroup of patients with preoperative biliary drainage. 21
Finally, some authors reported the usefulness of early postoperative reassessment of ICG clearance in both cirrhotic and noncirrhotic patients and in recipients after transplantation. 1 The ICG test performed on postoperative day (PoD) 1 after resective surgery seems a valuable tool for early detection of PHLF in both Eastern and Western series.22–24 Similarly, from the 90s, several studies suggested the strong early predictive role of the ICG test executed on PoD 1, in prognosticating graft dysfunction/failure and graft/recipient survival, although the optimal cutoff level has not been established yet.1,25–29 Early detection of impaired liver function would allow the introduction of aggressive corrective measures.
The ICG clearance test is feasible, repeatable, quite inexpensive, and scarcely invasive, especially if compared with other functional imaging tools including scintigraphy or functional magnetic resonance. 30 However, the results are strictly related to liver perfusion and may be unreliable with a bilirubin level higher than 3 mg/mL due to the competition for the same hepatocytic carrier between bilirubin and ICG. 1 Furthermore, repetitive assessments should be performed with an interval of at least 30 minutes to avoid misleading results due to the residual of the previous injection. 31
Intraoperative Applications
Cholecystectomy
A lot of anatomical biliary anomalies could be found, and the failure to identify them could cause an iatrogenic injury. With an incidence ranging from 0.15% to 0.6%, iatrogenic biliary lesions remain among the most feared complications during laparoscopic cholecystectomy.32,33
A standard intraoperative cholangiography could be performed to clarify the anatomy of the biliary ducts, but it has some limitations, including prolongation of the operative time, the 2D imaging, and minimal radiation exposure. Since the first intraoperative ICG cholangiography reported in 2009, 34 several studies, including randomized control trials (RCT), have reported ICG as a valid tool to highlight biliary anatomy in both open and laparoscopic procedures.35–37 ICG use could improve the visualization of the critical view of safety (CVS) 38 and provide additional visual information, especially in mini-invasive surgery, because laparoscopy is a two-dimensional surgery and lacks depth perception and haptic feedback. In 2020, the noninferiority of ICG cholangiography compared with the X-ray technique for the visualization of the extrahepatic biliary tree was reported. 39
The FALCON study, an international multicenter RCT, demonstrated a significantly faster recognition of hilar structures using IV ICG injection. 40 On the contrary, the SCOTCH study, a prospective nonrandomized trial on cholecystectomy performed by trainees, did not show a significantly shorter time to achieve the CVS with ICG use but the surgeon’s satisfaction was higher. 41 A huge meta-analysis including 22 studies and 3457 patients showed significantly better results with ICG in terms of better recognition of the cystic duct, reduction of the operative time, and conversion rates. 42
Many studies aimed to identify the correct dose and time of ICG IV injection. 43 In a prospective analysis of 146 patients, Aranda et al. demonstrated the best results with the standard dose of 2.5 mg when compared with the dose of 0.05 mg/Kg. Injection between 2 and 6 hours before the surgery was related to the best visualization of biliary structures, but even the administration of the dye 30 minutes before the intervention significantly improved the CSV visualization. 44 Ladd et al. performed a multicentric RCT to compare ICG IV injection on the day of the operation of low (0.05 mg) or standard dose (2.5 mg) through surgeon-blinded qualitative and quantitative scores. Probably due to the reduction of background fluorescence, significantly better results were found in the low-dose group. 45 Similarly, in a small RCT with 40 patients, Huang et al. achieved the best results with the administration of .1 mg 30 minutes before surgery. 46
On the other hand, Graves et al. in a small single-arm study showed that direct injection into the gallbladder can clearly define the extrahepatic biliary anatomy minimizing bile duct injuries and allowing a better visualization of the dissection plane. With this technique, the cystic artery is not highlighted, but it can be followed through the contrast with the fluorescent gallbladder. 47 Direct injection could be especially useful in cases of severe gallbladder inflammation or obese patients when it is more difficult to identify the correct planes.48,49
In a small prospective study by Castagneto-Gissey et al., IV and intracholecystic (IC) injections were compared. Depending on gallbladder size, an average of 5 mL of the dye, 25 mg/5 mL diluted in 10 mL of distilled water, was used for the IC injection at the beginning of the procedure. The limits of the IC use were hydrops of the gallbladder, significantly higher postoperative pain in case of cholecystic content spillage, the injection into the gallbladder wall causing liver fluorescence, and the presence of stone at the infundibulum requiring their mobilization to allow ICG flow. The IV administration of ICG was performed at the concentration of 0.01 mg/kg 45 minutes before surgery. The images were evaluated independently by two surgeons. The limit of the IV injection was the background liver fluorescence. In conclusion, both methods proved useful in reducing operative time and improving structure visualization. 50
Biliary leak detection
Biliary leak (BL) is still one of the most common complications after hepatectomy with an incidence of about 10%. This condition may be caused by biliary injury, bile oozing from the liver cut surface, or insufficiency of the bilioenteric anastomosis and may be associated with liver failure, sepsis, and consequently, prolonged hospital stays. 51
There are no standard methods for detecting small or occult BLs at the end of the resection. The most used tests are performed with intrabiliary injection (usually through the cystic duct stump) of the nontoxic and low-cost saline solution, air, methylene blue, or the White test using fat emulsion solutions or propofol. The sensitivity to detect microleakage was quite low, and on the other hand, the increased pressure in the biliary system could highlight leakages that may be not clinically significant. 52 Sakaguchi et al. conducted a prospective study comparing intrabiliary injection of 4–8 mL of 0.05 mg/mL ICG or saline solution at the end of hepatic surgery. After analyzing 59 patients, they reported higher but not significant detection rates of bile leaks (30% versus 19%) with the intrabiliary injection of low doses of ICG. 53
There is an ongoing prospective trial evaluating the routine use of systemic administration of ICG after hepatectomy for better BL detection. 54
However, although easily repeatable during the same procedure, this intraoperative test cannot exclude the possibility of postoperative bile leakage because BL could have several causes and, for example, can occur from ducts that are not in communication with the main biliary tree (i.e., orphan duct), or may be the consequence in a few days of ischemic damage.52,53
Finally, as reported for colorectal surgery, 55 ICG could also improve the outcomes of bilio-enteric anastomosis allowing the visualization of both blood perfusion and integrity of the suture. In particular, Ma et al. reported the best results in injecting the dose of 0.25 mg/kg 24 hours before the intervention, thus avoiding a hard-to-see image or excessive fluorescence. 56
Vascular anatomy for anatomical resections
Anatomical liver resections performed after segments and subsegments subdivision are a cornerstone in oncologic liver surgery, mostly in the case of HCC, improving survival and reducing postoperative complications. 57
With the great majority of the evidence coming from case reports or case series from Asian countries, ICG fluorescence can be used as a guide—combined with the usual techniques such as intraoperative ultrasonography (US) and preoperative Computed Tomography (CT) and Magnetic Resonance (MR) images—in parenchymal transection facilitating the identification of hepatic segments, in both open and laparoscopic surgery, improving postoperative outcomes.58,59 Although up to five different staining techniques have been described, 60 simplifying, the injection of the dye can determine a “positive staining” when ICG is injected into the portal pedicles feeding the tumor. Compared with the use of the Vital blue dye, the clamping of the hepatic artery is not necessary, and the color is much more persistent with a clearer demarcation. The “negative staining” is obtained when the fluorescent dye is injected intravenously after clamping the Glissonean pedicle of the hepatic segment involved in the resection through a Glissonean or transfissural approach. 58 Positive staining seems feasible and safe with a reported success rate of about 80% and 26 minutes needed to be performed. 61 According to the experience of Xu et al., it seems to be more useful in performing segmentectomy or subsegmentectomy. 62 However, it requires a high degree of proficiency with IOUS. 63 Negative staining seems easier to perform, avoids portal puncture, and could be used when there is an infiltration of the tumor-bearing portal branch. It is preferable when major resections or resections of left/anterior segments are required.62,64 Time and administration dose should be tailored for each patient. 65
An interesting use was reported by Kogure et al. They injected the ICG into the portal pedicle of the paracaval segment to be preserved during a right hepatectomy. This could be particularly useful when the future liver remnant volume is quite small. 66
Another appealing application was presented by Xie et al. After the “cone units” concept, 67 they performed subsegmental resections of the right posterior segments after transarterial super selective embolization of the feeding artery with lipiodol and ICG before surgery in 13 patients with early-stage HCC. The staining success rate was 85%, an R0 resection was performed in all the patients, and no severe complications occurred. They also analyzed the causes of unsuccess. 68
Liu et al. were the first to analyze both the intraoperative outcomes and the prognostic impact of ICG in anatomical resections for HCC. They performed a 1:1 propensity score-matched analysis including 100 patients comparing conventional laparoscopy and ICG-enhanced procedures (27 patients with tumor fluorescence imaging, 8 with positive staining, and 15 with negative staining). For positive staining, 5–10 mL of 0.025 mg/mL of ICG (25 mg of ICG diluted with 10 mL of sterile water then 1 mL [2.5 mg] of this solution diluted with 100 mL of saline) were used according to the segment volume. For negative staining, 10–20 mL of the same solution was used. With a median follow-up of 34 months, the ICG group showed significantly better results in terms of R0 resections, resection margin distance, blood loss, and DFS (independently associated with R0). 69 Although analyzing together different uses of ICG, they demonstrated that ICG could improve postoperative results in experience centers with no/low adjunctive risks.
However, since no strong evidence is available, Alomari et al. recently proposed a monocentric RTC to compare the results of positive and negative staining in laparoscopic resections. Positive staining will be performed with a slow injection of 1 mL of a 0.025 mg/mL ICG solution in the portal branch feeding the tumor punctured under ultrasound guidance, a dedicated probe is available. Negative staining with IV injection of 0.5 mg/kg after clamping the portal pedicle feeding the tumor. The extrahepatic Glissonean approach will be used. 70 ICG staining will be subjectively scored and compared with three-dimensional preoperative planning, short-term results, and disease-free survival will be also evaluated. The results are expected in the early 2027. 71
However, this modality of the evaluation of the segmental vascularization of the liver presents some difficulties. First, there could be technical difficulties in administering the ICG in the portal branch after exposing and clamping it. Second, negative staining may not work in the presence of vascular anomalies, i.e., the Hyrtl artery or other collateral circulations.62,72
Cancer localizations
After IV injection, the ICG remains fixed to pathological areas of the liver, particularly around nonhepatocellular tumors, where hepatocytes are underactive. 73 Therefore, ICG has emerged as a potentially useful tool for the intraoperative detection of hepatic neoplasms.
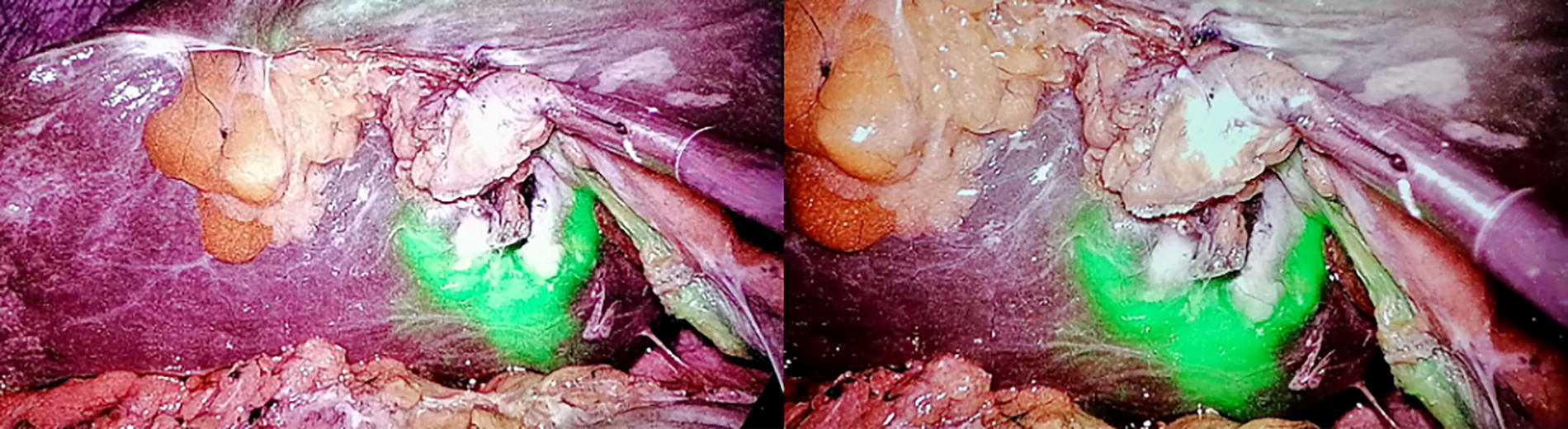
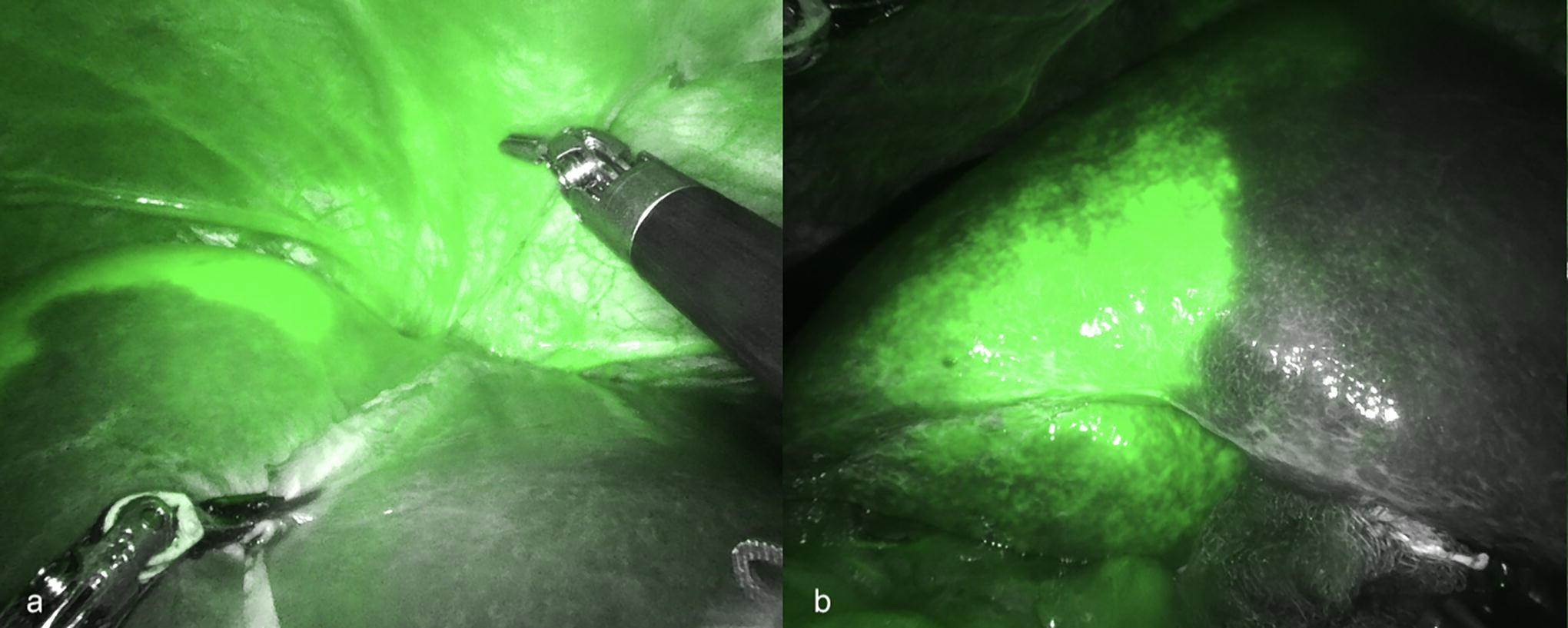
Gotoh et al. first introduced the use of intraoperative fluorescence imaging after the observation of a fluorescence pattern of HCC in patients whose hepatic function has been previously tested with ICG. 74 In parallel, Ishizawa described a fluorescence pattern for colorectal liver metastasis (CRLM). 34 Different hepatic lesions may result in a different fluorescence pattern. HCC presents 3 different types of fluorescence signal: a total fluorescence type (well‐differentiated HCC), a partial fluorescence type (moderately differentiated HCC), and a rim fluorescence type (poorly differentiated HCC). 2 ICG sensitivity in detecting HCC has been reported to reach 99% with a 6% false positive. 75 The incidence of false positives is higher (up to 40%) in patients with atypical nonmalignant lesions, with decreased liver function due to cirrhosis, or preoperative chemotherapy, but this could be reduced by increasing the time between ICG injection and the procedure or adjusting the dose.69,75 Residual cancer or vein tumor thrombus can be detected on the cut surface with ICG. 76 Even unexpected distant HCC metastasis could be detected through the use of ICG. 77 (Fig. 2-3)

Clear visualization of a single Sg6 HCC. HCC, hepatocarcinoma.
Clear visualization of a single Sg3 HCC. HCC, hepatocarcinoma.
CRLM presented with a rim‐type fluorescence signal. This pattern is caused by immature hepatocytes with a decreased bile excretion ability surrounding the tumor. 78 The use of fluorescence may be particularly useful after chemotherapy which can cause a partial/complete regression or necrosis of the lesions which become more difficult to see with the naked eye, especially in laparoscopic surgery. 79 In general, the sensitivity of CRLM identification with ICG ranges from 73% to 100%, and several studies reported a significantly higher detection rate of unexpected lesions compared with conventional resections.64,80–82 In particular, Boogerd et al. compared the sensitivity of different imaging techniques in detecting liver malignancies. Of the 20 patients finally included in the study, 10 of them were affected by CRLM. Sensitivities and positive predictive values of the different techniques were 80% and 71% for CT scan, 84% and 80% for MRI, 88% and 77% for IOUS, and 92% and 75% with ICG. Interestingly, although not statistically significant, the sensitivity of all the traditional imaging techniques markedly decreased with lesions smaller than 10 mm compared with ICG, and the use of fluorescence allowed for the detection of three lesions not identified by other techniques. Furthermore, the combined use of ICG and IOUS allowed the reaching of 100% sensitivity and 70% positive predictive value. 83 Small superficial lesions missed at the intraoperative ultrasound evaluation could be highlighted with ICG and the maintenance of a correct transection plane (and, eventually, an R0 resection) could be improved with ICG while resecting deeper located lesions.64,72,84 However, the fluorescent rim could be smaller than 5 mm, and consequently, an R0 resection could not be assured in every report (due to different R0 definitions) 80 (Fig. 4-5).

Intrahepatic cholangiocarcinoma (ICC) displayed an intermediate fluorescence pattern with the majority showing a rim-staining while a minority presenting with a complete or partial fluorescence. 77
A recently published meta-analysis including 959 laparoscopic resections for liver malignancies (446 patients operated with the aid of ICG and 513 treated without the use of ICG) showed a significantly higher R0 rate, less necessity of intraoperative blood transfusion, and shorter hospital stay with similar postoperative morbidity in the ICG group of patients compared with those treated with conventional surgery. 85 Another meta-analysis reported also a shorter operative time, lower postoperative complications, and a better 1-year disease-free survival rate. 86 Similar results were also reported for the robotic technique.87,88
A limitation of this technique is the depth of tissue penetration of fluorescence signal of less than 8 mm from the hepatic surface. Another limitation is represented by the excessive background fluorescence in case of ICG overdose which cannot be reduced. Indeed, the timing of injection and optimal dosage of ICG are important issues for the success and the standardization of the technique. The optimal dose of ICG is still unknown and may vary according to hepatic function. Several studies reported an IV ICG administration of 0.25–0.5 mg/kg from 12 hours to 14 days before surgery, while others proposed an intraoperative injection.2,65,89
Chen et al. proposed a score based on preoperative blood tests to predict a good or poor hepatic clearance ability to adjust their standard preoperative ICG dose of 5 mg 24 hours before surgery. 90
Other applications
Lymphadenectomy
Survival is highly influenced by node status and that lymphatic outflow may differ in each person; in particular, some main pathways have been identified, namely, the hepato-cholecystic-retropancreatic pathway, the hepato-celiac pathway, the hepato-mesenteric pathway, and the diaphragmatic pathway. 91
Visualization of extrahepatic biliary structures may be helpful during the lymphadenectomy of the porta hepatis, whenever required.
Although within isolated reports, Ruzzenente et al. published the results of a prospective pilot study with 18 patients with ICC evaluating the role of the ICG in highlighting the lymphatic out-flow from the liver and the sentinel lymph node retrieving in hepatobiliary cancers. Emphasizing the importance of a correct but tailored lymphadenectomy, they proposed the peritumoral injection of 1 mL of 25 mg of ICG in 20 mL of water. The lymphatic pathway was visible in 77.8% of the patients within 3 minutes of the injection. The sentinel lymph node was detected in 77.2% of the patients, confirmed by pathological examination in 92.3% of the patients, and resulted positive in a quarter of the patients. 91 Similar results have been previously reported. 92
Transplantation: Living donor
Biliary complications are the most common ones during donor hepatectomy, and they are avoided by the recognition of biliary structures and by optimal bile duct dissection-line of the liver graft. 93 Recently, real-time ICG NIR fluorescence techniques have been used to divide the bile duct during laparoscopic living donor hepatectomy. The amount of IV injected ICG was 2.5 mg/kg 15–30 minutes before hilar plate dissection. 64
The cholangiography using ICG seems superior to conventional cholangiography because it does not involve radiation and it shows a 3D spatial direction and relationships between structures. 93 This is an easy and safe technique that allows intraoperative visualization of biliary anatomy (including aberrant bile ducts), leading to an efficient and rapid dissection of the hilar plate. The amount of intrabiliary injected ICG was 0.05 mg/kg. The limit of this technique is represented by the patients with high body mass index because it cannot easily delineate bile ducts covered with adipose or connective tissue. 93
As reported above, cholangiography can be performed with IV or intrabiliary injection of the ICG. Furthermore, IV ICG injection could be useful in checking vascularization and the integrity of the bile duct anastomosis. 94
Future Prospectives
In recent years, the second NIR window, NIR-II, with a different wavelength of 1000–1700 nm. has been studied. 95 It is not disturbed by the operative room lights, it can reduce photon absorption and scattering effects of deep tissue, allows a deeper view (up to 1 cm), a better spatial resolution, reduces tissue autofluorescence providing a better contrast and, definitively, an upgrade of the tool. 96 A quantitative analysis of the signal-to-background ratio, tumor-to-background ratio, and tumor-to-normal tissue ratio has been performed showing the great superiority of the NIR-II over NIR-I with significantly higher sensitivity and specificity in tumor detection. 95
ICG remains the most used fluorophore, although other dyes are under evaluation.96,97 In particular, fluorophores combined with polyethylene glycol or with cancer antibodies are expected to be further developed for human use allowing better and more precise visualization of tumor margins.98,99
Multimodal imaging systems combining NIR and other imaging techniques are another promising field of study.
Preliminary results of NIR-II and photodynamic therapy integration for HCC on animal models seem promising. 100
Finally, in the era of artificial intelligence and machine learning techniques, Hardy et al. reported their use combined with the ICG fluorescence to improve the R0 resection rate and the intraoperative detection of unexpected CRLM. 101
Conclusion
In conclusion, the simplicity of the use of ICG makes it one of the most used dyes in general surgery. A growing body of literature is demonstrating that this technique is easily reproducible and reliable with relatively low costs and without side effects. Moreover, this method gives the possibility to carry out more clean resections, ensuring a higher rate of disease-free margins. Further improvements in the imaging system and standardization of the ICG usage (dose and timing) are expected, allowing this technique to be a part of the standard clinical practice.
Footnotes
Authors’ Contributions
L.F.: writing—original draft preparation and reviewing. M.R., M.N.R., and A.T.: reviewing and editing. S.B.: reviewing and editing. F.M. and C.A.: writing—original draft preparation. I.B.: conceptualization, writing—original draft preparation, review, and editing. G.L.G.: writing—original draft preparation, reviewing, and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.