
Abstract
Background:
Lumbar hernia is a rare disease with low incidence, and no golden standard surgical procedure has been established for lumbar hernias. The single-incision laparoscopic totally extraperitoneal sublay (SIL-TES) technique became a novel surgical technique for lumbar hernias.
Methods:
This retrospective study included 20 patients who underwent SIL-TES repair for lumbar hernia between April 2020 and March 2024. The baseline patient characteristics, intraoperative data, postoperative data, satisfaction score, and Carolina Comfort Scale scores were collected.
Results:
The results revealed that the SIL-TES technique for lumbar hernia repair is associated with a low complication rate, nonrecurrence, high satisfaction score, and high quality of life after surgery.
Conclusions:
The SIL-TES technique could be a feasible and effective surgical technique for lumbar hernias. A controlled study is needed for further confirmation.
Introduction
Lumbar hernia was first described by Barbette in 1672; however, its first report was written by Garangeot and published in 1731. 1 Lumbar hernia is classified into congenital (20%) and acquired (80%), and the acquired type has been further classified into primary and secondary based on its etiology. 2 Despite reports on the rarity of lumbar hernia, it should be repaired surgically because 25% of lumbar hernias progress to incarceration and 8% become strangulated. 3
Currently, open and laparoscopic repairs are both performed for lumbar hernia, and the laparoscopic type has become popular in recent years. Laparoscopic repair has two approaches, namely, transabdominal and totally extraperitoneal. 4 Recently, the single-incision laparoscopic totally extraperitoneal repair (SIL-TEP) has been gradually accepted by hernia surgeons. It has been applied not only to inguinal hernia but also to ventral hernia, including lumbar hernia. The repair technique for ventral hernia is also called the single-incision laparoscopic totally extraperitoneal sublay (SIL-TES) technique.5,6 However, owing to the difficulty of space establishment and surgical operation under SIL, only a few sporadic cases were reported.
Since 2017, we began to perform SIL-TES repair in various ventral hernias, summarized the early experience of 4 years, and reported our data in 2021. The results of these cases proved its effectiveness as a supplement to routine laparoscopic repair. 7 Herein, we report the outcomes of SIL-TES repair of lumbar hernias.
Materials and Methods
This retrospective study included 20 patients who underwent SIL-TES repair for lumbar hernias between April 2020 and March 2024 from the following three hernia centers: Shanghai General Hospital (n = 6), Shanghai East Hospital (n = 10), and The First Affiliated Hospital of Ningbo University (n = 4).
This study was approved by the Ethics Committee of Shanghai General Hospital (Approval No. 2020-053), and participants provided written informed consent.
The following data were collected: baseline patient characteristics including age, sex, body mass index, American Society of Anesthesiologists classification, type of hernia, and comorbidity; intraoperative data including length of incision, operation time, bleeding volume, hernia defect size, mesh size, conversion status, and intraoperative complications (peritoneum injury, vascular injury, and intestinal injury); and postoperative data including the Visual Analog Scale (VAS) score (6, 24, and 48 hours after the operation) indicating postoperative pain, urinary retention, seroma, hematoma, incision dehiscence, incision infection, intestinal obstruction, pulmonary infection, urinary tract infection, myocardial infarction, heart failure, stroke, length of hospital stay, readmission within 30 days, mesh infection, trocar herniation, and patients’ remark of surgical satisfaction and cosmetic satisfaction. The quality of life (QoL) was assessed using the Carolina Comfort Scale (CCS) before surgery and at 1 week, 1 month, 6 months, and 1 year after surgery. The evaluation of QoL included pain, sensation, and movement limitations on a 0–5 scale, which was conducted face-to-face at the outpatient clinic or by telephonic follow-up.
Surgical technique
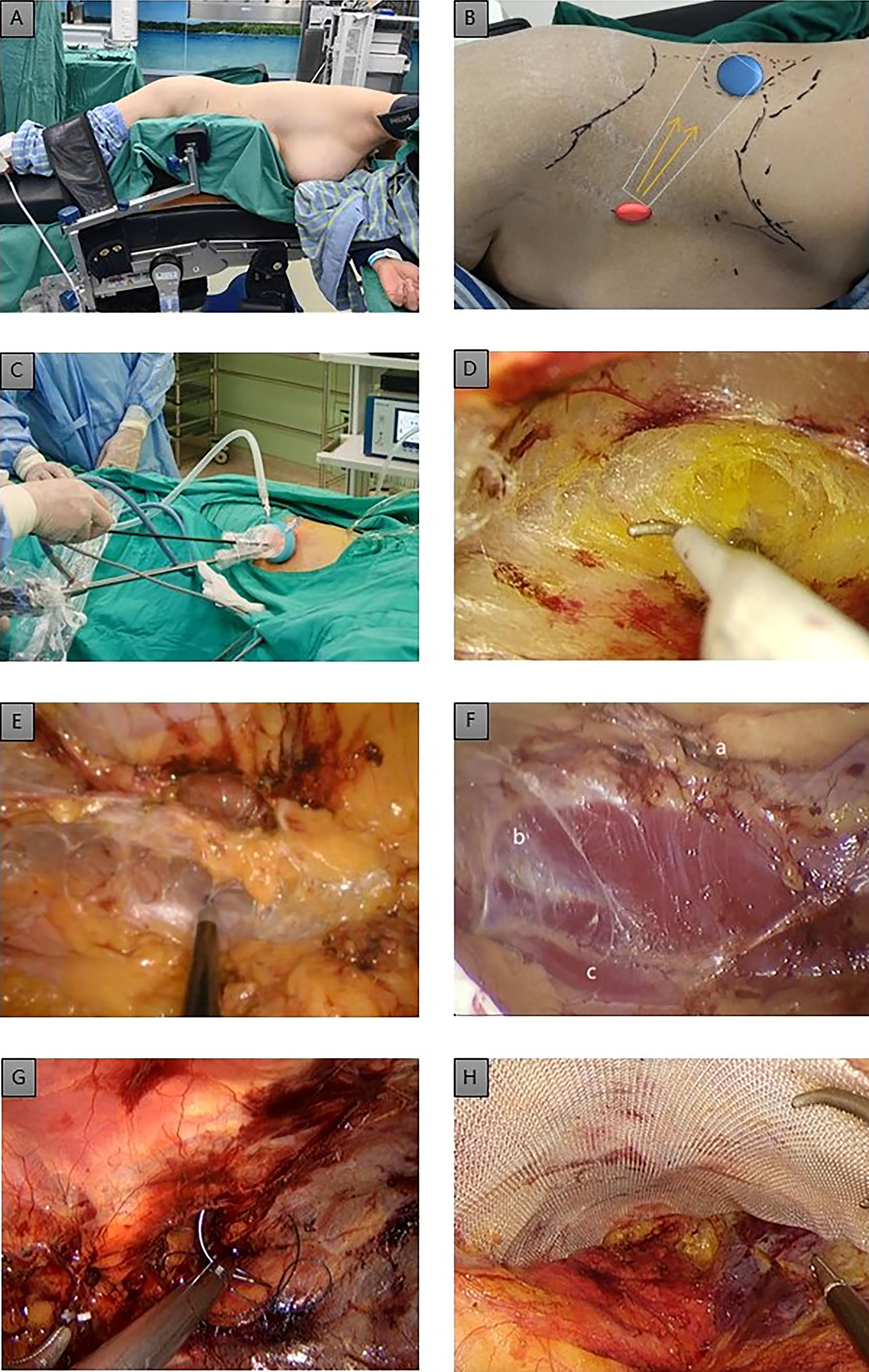
After the induction of general anesthesia, the patient was placed in the lateral decubitus position with a raised waist (Fig. 1A). A single, 2-cm longitudinal incision was made between the 12th rib and the superior anterior iliac spine on the anterior axillary line (Fig. 1B). The external oblique abdominis, internal oblique abdominis, and transversus abdominis were incised to reach the extraperitoneal space. After a Lap-Protector Mini (HangTian KaDi Co., Beijing, China) was placed in the extraperitoneal space, a single port (HangTian KaDi Co.) with three working channels and two gas channels was attached to the Lap-Protector Mini to maintain the inflation of the preperitoneal space with carbon dioxide (Fig. 1C). Thus, the preperitoneal space toward the dorsal side was separated gradually under the camera’s guidance (Fig. 1D). The hernia ring was recognized and dissected, and the hernia contents were reduced from the sac. The separation range was at least 5 cm in longitude and 4 cm in latitude away from the hernia ring (Fig. 1E). The collateral branch of the subcostal nerve, iliohypogastric nerve, and ilioinguinal nerve may be recognized (Fig. 1F). The hernia ring was then closed with barbed sutures (Fig. 1G). If the defect was too large (mostly secondary hernia) to close, the mesh should be large enough with reliable fixation such as sutures and tacks. Then, a polypropylene mesh, which measured from 8 × 13 cm to 15 × 20 cm, was placed in the separated space (Fig. 1H). If the hernia ring is small and is closed properly, mesh fixation can be spared. Then, the retroperitoneal space was deflated slowly and carefully to avoid mesh shifting and rolling. The external oblique abdominis was closed with 1–0 absorbable sutures, and the skin was closed with intradermal sutures.
Statistical analysis
Descriptive statistical analysis was used. Measurement data were expressed as mean (± standard deviation), and counting data were expressed by frequency (percentage). IBM SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA) was used to complete data collation and analysis, and P < .05 was considered statistically significant.
Results
Demographic results
The demographic data of the 20 patients are provided in Table 1. All patients were diagnosed with unilateral lumbar hernia. Ten patients had primary lumbar hernia, and another 10 had secondary lumbar hernia; among them, 9 were caused by surgery incision and 1 by trauma.
Demographic Data
SD, standard deviation; ASA, American Society of Anesthesiologists.
Perioperative outcomes
Perioperative data are shown in Table 2. Given that most of the defect shapes were elliptic or round, the defect size was estimated using an elliptical area formula. The intraoperative investigation concluded that the average hernia defect size was 12.6 ± 16.0 cm2, and the average mesh size was 164.5 ± 38.2 cm2. There are two patients whose defects (40.1 and 37.7 cm2) were too huge to be closed completely. Therefore, we had to transfer to shrink the gap and then put a large bridging mesh with tackers fixation in one patient and sutured the defect margin with the folding hernia sac to flatten the frank wall in another patient. All other patients’ defects were closed completely with barbed sutures. The CCS score data of patients before surgery and at 1 week, 1 month, 6 months, and 1 year after surgery are shown in Table 3.
Perioperative Parameters
SD, standard deviation; VAS, Visual Analog Scale.
Carolina Comfort Scale Score
CCS, Carolina Comfort Scale; SD, standard deviation.
Follow-up results
The duration of follow-up ranged from 1 to 48 (median = 18.5, upper quartile = 41, lower quartile = 5) months, and no patients were lost to follow-up. One patient presented with hematoma and recovered after conservative treatment. Another patient presented with a bulge in the surgical site (patient’s hernia defect size was 40.1 cm2, repaired with mesh bridging), but no defect was confirmed by computed tomography. No urinary retention, symptomatic seroma found by palpation, SSI, bowel obstruction, incisional hernia or recurrent hernia, and other complications were noted during follow-up. Moreover, the CCS scores after surgery were lower than those before surgery. Three patients reported foreign body sensation 1 year after surgery, with an average CCS score of 0.73 ± 1.79, and no patients reported pain and movement limitations 1 year after surgery.
Discussion
Lumbar hernia is a rare disease with low incidence, and most surgeons, even hernia specialists, have insufficient surgical experience.8–11 Consequently, no golden standard surgical procedure has been established for lumbar hernias. Before the development of the laparoscopic technique, open sublay repair was the most frequently used procedure for lumbar hernias. With a small lumbotomy, it appears to have advantages concerning the facility and a direct approach. However, with an incision in the dorsal area, extensive subcutaneous dissection is needed, and the location of the hernia ring is quite difficult for cases with a small defect.
The first laparoscopic repair for lumbar hernias was reported in 1996. 12 Compared with open repair, laparoscopic repair has the remarkable advantages of having lower injury rates, reduced levels of acute and chronic postoperative pain, lower incidence of incision occurrence, and improved esthetics of the incision.13,14 For lumbar hernias, two additional advantages emerge, namely, the precise location of the hernia defect and direct visualization of nerves under the muscles, which help avoid injury.8,15 Initially, all lumber hernia repairs with the laparoscopic technique are performed via the transabdominal approach. However, the defect in lumbar hernias is located in the retroperitoneum. Therefore, in the transabdominal approach, the abdominal cavity must be entered first, dissecting adhesion if needed and then separating the right/left semicolon to expose the hernia defect. After repair, the mesh must be fixed with tacks and the separated semicolon reattached to the peritoneum. We consider this as an indirect approach, and several surgical steps are supplements and should be performed, which may lead to potential complications. For example, adhesion lysis and semicolon separation may lead to a possible inadvertent enterotomy. Meanwhile, if the mesh is covered completely by the semicolon, the sublay repair is similar to the transabdominal preperitoneal repair of inguinal hernias. However, if the mesh cannot be covered completely, the inner part of the mesh must be exploded in the abdominal cavity, a tissue-separating mesh must be used, and such procedure is also called transabdominal partially extraperitoneal repair, which increases the incidence of potential long-term complications such as bowel adhesion and even intestinal fistula/mesh erosion.16,17
Laparoscopic totally extraperitoneal repair, first described by Miserez in 2002 18 and named as enhanced-view totally extraperitoneal or TES by various scholars, is an attractive and developing technique. It demonstrates unique therapeutic effects on ventral hernias on the midline. This novel technique was also introduced to lumbar hernia repair and was first described by Meinke in 2003. 19 The whole procedure is confined in the preperitoneal space. Therefore, it not only allows determining the precise anatomical location of the hernia defect 8 but also avoids interfering with the abdominal cavity and the separation of semicolon, reducing the possibility of inadvertent enterotomy and subsequent intra-abdominal adhesions. After separation, a large flat mesh will be placed in the preperitoneal plane, allowing intra-abdominal pressure to hold it in position and requiring minimal fixation, which results in postoperative pain and faster recovery. The nonuse of tissue-separation mesh and tacks also lowers the treatment cost. Our cases showed that this approach for lumbar hernia repair has low complication rates and low postoperative VAS scores, indicating the safety and effectiveness of the procedure. The low CCS score and high cosmetic satisfaction mean that it can be well tolerated by the patients.
Furthermore, the lateral peritoneum is much thicker than the midline peritoneum, more extraperitoneal fat is present, and the preperitoneal space of the retroperitoneum is much looser than that of the midline. All these factors reduce the difficulty of space separation and the risk of peritoneum damage. Thus, compared with midline ventral hernia, TES for lumbar hernia is relatively easier to perform and the learning curve is shorter. Among 20 cases, only 7 patients experienced peritoneal tears. The effect of the torn peritoneum was minor, and there was no conversion. The operative time appeared shorter than that of the transabdominal approach. Comprehensively, it is a feasible procedure and can be quickly familiarized by surgeons accustomed to TEP.
In the beginning, we performed the procedure with the conventional three-trocar layout. However, the gap between the costal arch and the iliac crest is short; thus, the longitudinal space of the lumbar area is so confined, resulting in the crowding of instruments and the narrow working angle. It appears that the operating difficulty is similar to that of the SIL surgery. Meanwhile, as we obtained more experience in SILS, we attempted SIL-TES on lumbar hernia repair. Unlike the transabdominal approach, the TES technique requires a primary working space. For the conventional three-trocar layout, a primary space can be created only with blunt dissection (telescope push or blind balloon dilatation), which may lead to ripped peritoneum or hemorrhage, making the subsequent procedure difficult and increasing the risk of intraoperative and postoperative complications. SIL-TES allows surgeons to put three instruments together after the first incision, which allows making a sharp dissection under camera guidance at the very beginning when the port is in position, and we call this “hand–eye synchronization.” We consider that it should be safer than blunt dissection under the three-trocar layout. Even if a peritoneal tear is encountered in the early stage, with the help of one instrument, the effect of pneumoperitoneum leakage will be minimized, and space separation can proceed with another instrument. In addition, as the transverse distance from the trocar/port to the defect is also short, the SILS port may save the 2–3 cm distance when compared with that of the trocar. Therefore, according to our experience, SILS should be more suitable than the conventional three-trocar layout for the lumbar hernia repair.
Conclusion
At present, the surgical procedures of lumbar hernia vary, and SIL-TES is a novel technique. According to the results of this series, SIL-TES repair is a feasible and effective procedure for lumbar hernia repair. Compared with open repair, it has the advantages of less trauma, esthetic improvement, and precise determination of the defect location. Compared with the laparoscopic transabdominal approach, SIL-TES requires minimal mesh fixation, prevents the mesh from directly contacting the viscera, and needs no expensive anti-adhesive mesh. Compared with routine three-incision TES, SIL-TES makes the establishment of the initial space easier under direct vision and it appears much more suitable for the short gap in the flank area. A controlled study is needed for further confirmation.
Footnotes
Acknowledgments
The authors would like to thank B. Todd Heniford and his team from the Carolinas Hernia Center, Division of Gastrointestinal and Minimally Invasive Surgery, Carolinas Medical Center, Charlotte, NC. The authors thank them for issuing a license agreement of CCS, by which they performed an effective evaluation of QoL after surgery.
Authors’ Contributions
Y.Z.: Conceptualization (lead) and resources (equal). W.W.: Resources (equal), methodology (lead), funding acquisition (lead), and investigation (equal). T.W.: Formal analysis (lead). X.S.: Investigation (equal). L.H.: Writing—original draft (lead). R.T.: Supervision (lead) and resources (equal). N.L.: Project administration (lead), visualization (lead), and writing—review and editing (lead).
Disclosure Statement
No competing financial interests exist..
Funding Information
This study was supported by the grant from the