
Abstract
Purpose:
This study aims to explore the influence of human immunodeficiency virus (HIV) infection on the prognosis of patients with hepatocellular carcinoma (HCC).
Methods:
According to the search strategy, we searched all relevant articles in the three databases (PubMed, Embase, and the Cochrane Library) up to February 18, 2024. All data available for analysis were extracted. Continuous variables were expressed as mean difference (MD) with standard deviation (SD). The categorical variables were expressed as odds ratio (OR) with 95% confidence intervals (CIs). Forest plots were used to illustrate the analysis results, and funnel plots were used to assess publication bias.
Results:
The study included a total of 4544 subjects. HIV patients were significantly younger compared to those without HIV (MD = −16.13, 95% CI = −17.24 to −15.01, I2 = 91, P < .01), but there were no significant differences in other relevant clinical characteristics between the groups. Survival analysis indicated that HIV patients exhibited a poorer long-term prognosis compared with HIV-negative patients (HR = 0.71, 95% CI = 0.63 to 0.79, I 2 = 29%, P < .01).
Conclusion:
HIV infection, which compromises immune function and liver health, predisposes individuals to earlier onset of HCC and is associated with a poorer prognosis.
Introduction
Primary liver cancer is the fifth most common malignancy worldwide and the third leading cause of cancer-related deaths. 1 Hepatocellular carcinoma (HCC) constitutes approximately 75%–85% of all primary liver cancer cases and is notorious for its dismal overall prognosis.2–3 The main risk factors include hepatitis B virus (HBV) infection or hepatitis C virus (HCV) infection, aflatoxin, heavy alcohol consumption, obesity, and diabetes. In addition, HCC is also one of the predominant non-AIDS-defining cancers among human immunodeficiency virus (HIV)-infected patients.
Since the introduction of highly active antiretroviral therapy (HAART), the lifespan of HIV patients has substantially increased, followed by an increase in non-AIDS-related mortality.4–5 Indeed, the morbidity and mortality from non-AIDS-related cancers now exceed those from AIDS-related cancers, with HCC emerging as a significant cause of death among HIV patients.6–7 According to relevant research, the incidence of HCC is three to seven times higher in HIV patients compared to the general population, and this figure increases to 10 in cases of co-infection with HBV or HCV.8–10
Despite the growing prevalence and mortality of HCC in HIV patients, the specific impact of HIV on the development and prognosis of HCC remains underexplored. Some studies have shown faster HCC progression and higher mortality in HIV patients compared to those without HIV infection.11–12 Conversely, other research has identified no significant differences in survival between these groups. 13
In this study, we divided patients with HCC into HIV-infected and non-infected groups. By comparing the differences in clinical characteristics and survival between the two groups, we aimed to reveal the impact of HIV status on the development and prognosis of HCC, hoping to help make better treatment decisions.
Methods
This study was conducted under the guidance of the 2020 PRISMA guidelines. 14 All the data utilized were sourced from original articles. Ethical approval and informed consent forms were not applicable.
Literature search
We conducted an extensive search in PubMed, Embase, and the Cochrane Library up to February 18, 2024, using a defined search strategy. The two main search terms were “HCC” and “HIV”. For HCC, the search formula was “hepatocellular carcinoma” odds ratio (OR) “hepatocellular carcinomas” OR “hepatic cancer” OR “liver cancer” OR “hepatocellular cancer” OR “hepatic neoplasm” OR “hepatic neoplasm” OR “hepatocellular neoplasm” OR “HCC”. As for HIV, it was searched as “human immunodeficiency virus” OR “human immunodeficiency viruses” OR “HIV” OR “acquired immune deficiency syndrome virus” OR “AIDS” OR “AIDS virus” OR “AIDS viruses” OR “acquired immune deficiency syndrome virus”. The scope of the search was limited to titles and abstracts, and all non-English literature was excluded.
Inclusion and exclusion criteria
The inclusion criteria for articles were as follows: (1) subjects aged ≥ 18 years; (2) patients divided into two groups according to HIV infection status; (3) availability of extractable prognostic data. Exclusion criteria included: (1) non-original articles such as conference abstracts, reviews, letters, comments, case reports, or surveys; (2) studies with duplicate data; 3) studies with inadequate or unextractable data.
Study selection
Two authors independently performed the literature search. Duplicate studies were first removed. Titles and abstracts were then screened to identify relevant articles. Full texts were assessed to confirm eligibility based on the inclusion and exclusion criteria. Disagreements were resolved by consultation with a third author. When the inclusion of an article was disputed, the decision was left to the third author.
Data collection
Data were independently extracted and then cross-checked by two authors to ensure accuracy. Basic data extracted from each article included: name of the first author, time of publication, country of publication, and type of study. Clinical data included age, sex, drinking history, symptoms, Child-Turcotte-Pugh (CTP) classification; Barcelona Clinic Liver Cancer (BCLC) staging, co-infection with HBV, co-infection with HCV, number of tumors, portal vein thrombosis, extrahepatic metastasis, liver transplantation, and prognostic information.
Quality assessment
The quality of the included studies was evaluated using the Newcastle-Ottawa Scale (NOS), 15 focusing on the selection of study groups, comparability, and the assessment of outcomes. Studies were rated on a scale from 0 to 9, with scores of indicating high quality, scores of 7 to 8 indicating moderate quality, and scores below seven indicating low quality.
Statistical analysis
Continuous variables were expressed as mean difference (MD) with standard deviation (SD). The categorical variables were expressed as OR with 95% confidence intervals (CIs). Heterogeneity was assessed using the I2 statistic and the chi-square test. A fixed-effect model was employed for I2 < 50% and a random-effects model was used when I2 > 50%, considering significant heterogeneity. P values < .05 were considered statistically significant for fixed effects, and P < .1 for random effects. Hazard ratios (HRs) and 95% CIs were pooled to compare the effect sizes between HIV-positive status and overall survival. Funnel plots were used to assess possible publication bias. All statistical analyses were performed using Review Manager (V.5.3) software.
Results
Study selection
Through our systematic search strategy, we identified a total of 5211 articles, including 1502 from PubMed, 577 from the Cochrane Library, and 3132 from Embase. After removing 1121 duplicates, we screened the titles and abstracts of the remaining articles, narrowing down to 58 articles for full-text review. Ultimately, 11 articles met our inclusion criteria and were included in this analysis.13,16–25 (Fig. 1)
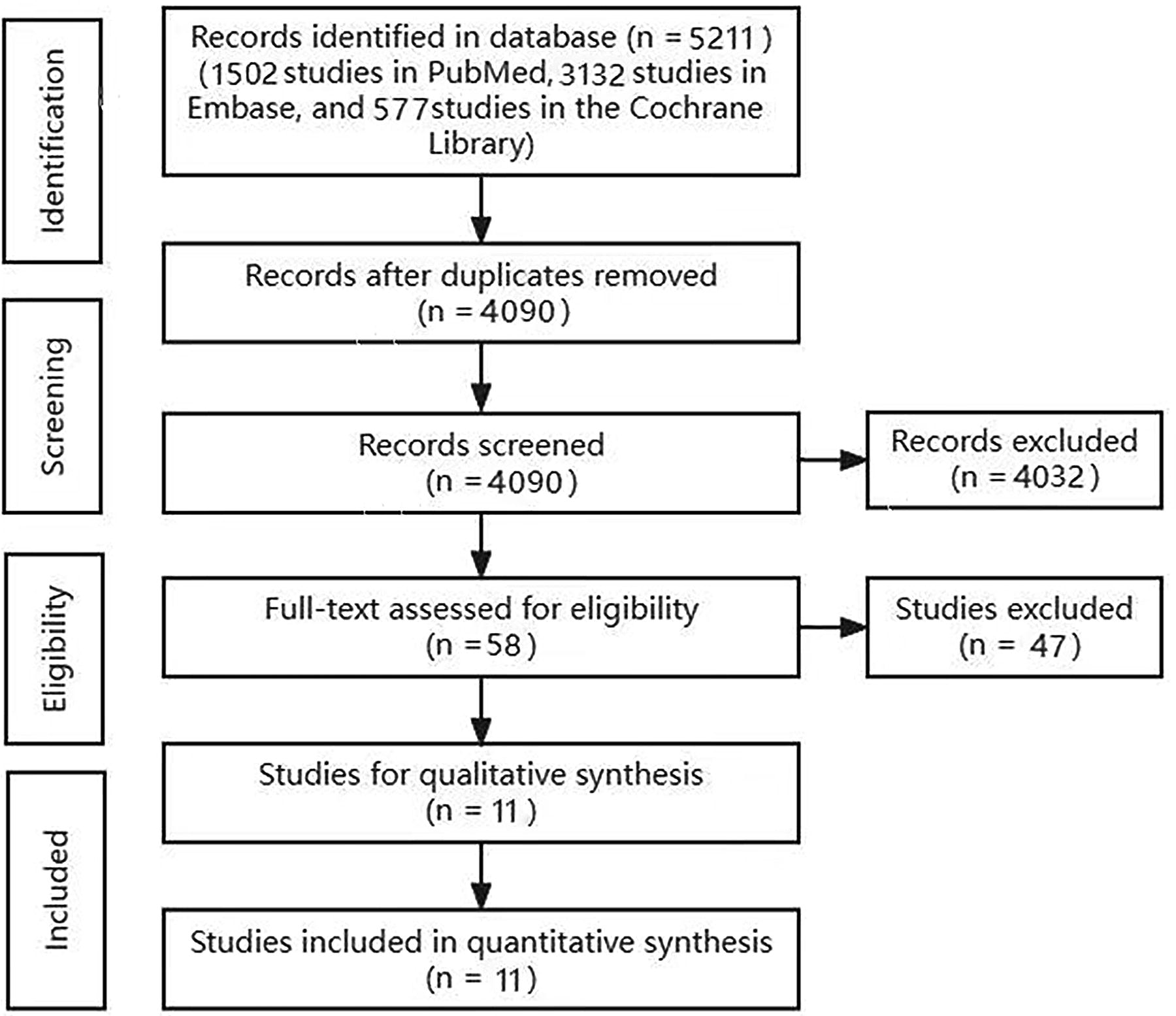
Flowchart of study selection.
Characteristics of included studies
A total of 11 articles from seven different countries were included in this study. Among these, four were prospective studies, and seven were retrospective. Two studies exclusively included patients infected with HCV. Detailed baseline information and NOS scores are presented in Table 1.
Baseline Characteristics of Included Studies
NOS, Newcastle-Ottawa Scales; HIV, human immunodeficiency virus; HCV, hepatitis C virus.
Comparison of basic clinical information between HIV positive group and negative group in patients with HCC
After pooling all extracted data, we found that HIV patients were significantly younger compared to their HIV-negative counterparts in the HCC cohort (MD = −16.13, 95% CI = −17.24 to −15.01, I2 = 91, P < .01). However, no significant differences were observed between the groups in terms of gender, symptoms, BCLC staging, TP classification, or liver transplantation status. Similarly, for pathological features, the two groups did not differ in the number of liver tumors, the incidence of portal vein thrombosis, or the occurrence of extrahepatic metastases (Fig. 2 and Fig. 3).

Comparison of basic clinical information between HIV positive group and negative group in HCC patients.
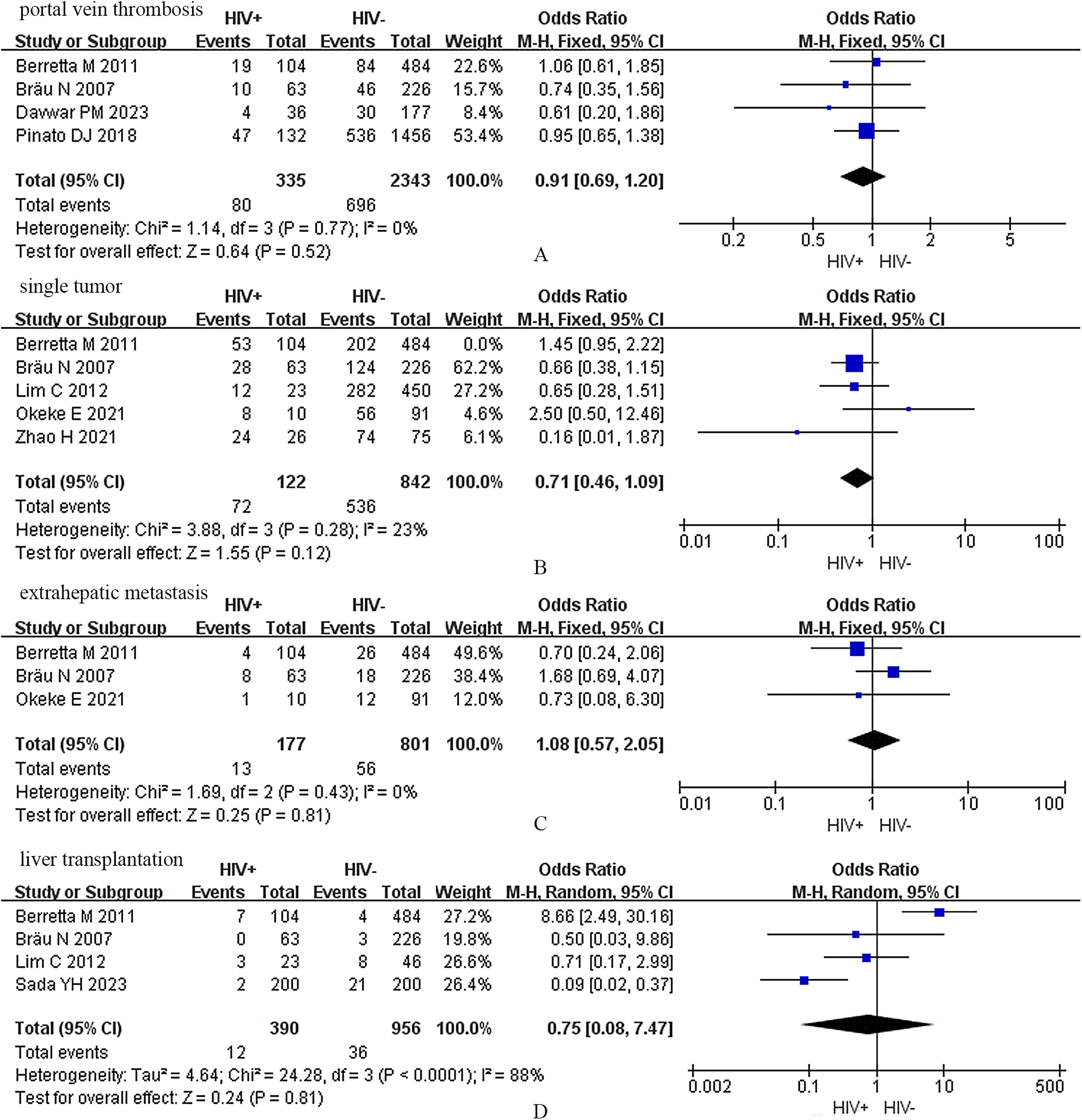
Comparison of pathological features between HIV positive group and negative group in HCC patients.
Co-infection with HBV or HCV
The results showed that HIV patients had a higher HBV infection rate (OR = 2.06, 95% CI = 1.04 to 4.09, I2 = 78%, P = .04). However, no significant difference was observed in the incidence of HCV (OR = 1.09, 95% CI = 0.72 to 1.65, I2 = 54%, P = .69) co-infection between the HIV-Infected and non-HIV-Infected groups. A subgroup analysis of HCV-infected HCC patients was performed next. We found that HIV status did not account for differences in outcomes between the two groups (HR = 0.72, 95% CI = 0.31 to 0.1.67, I2 =85%, P = .44). (Fig. 4)
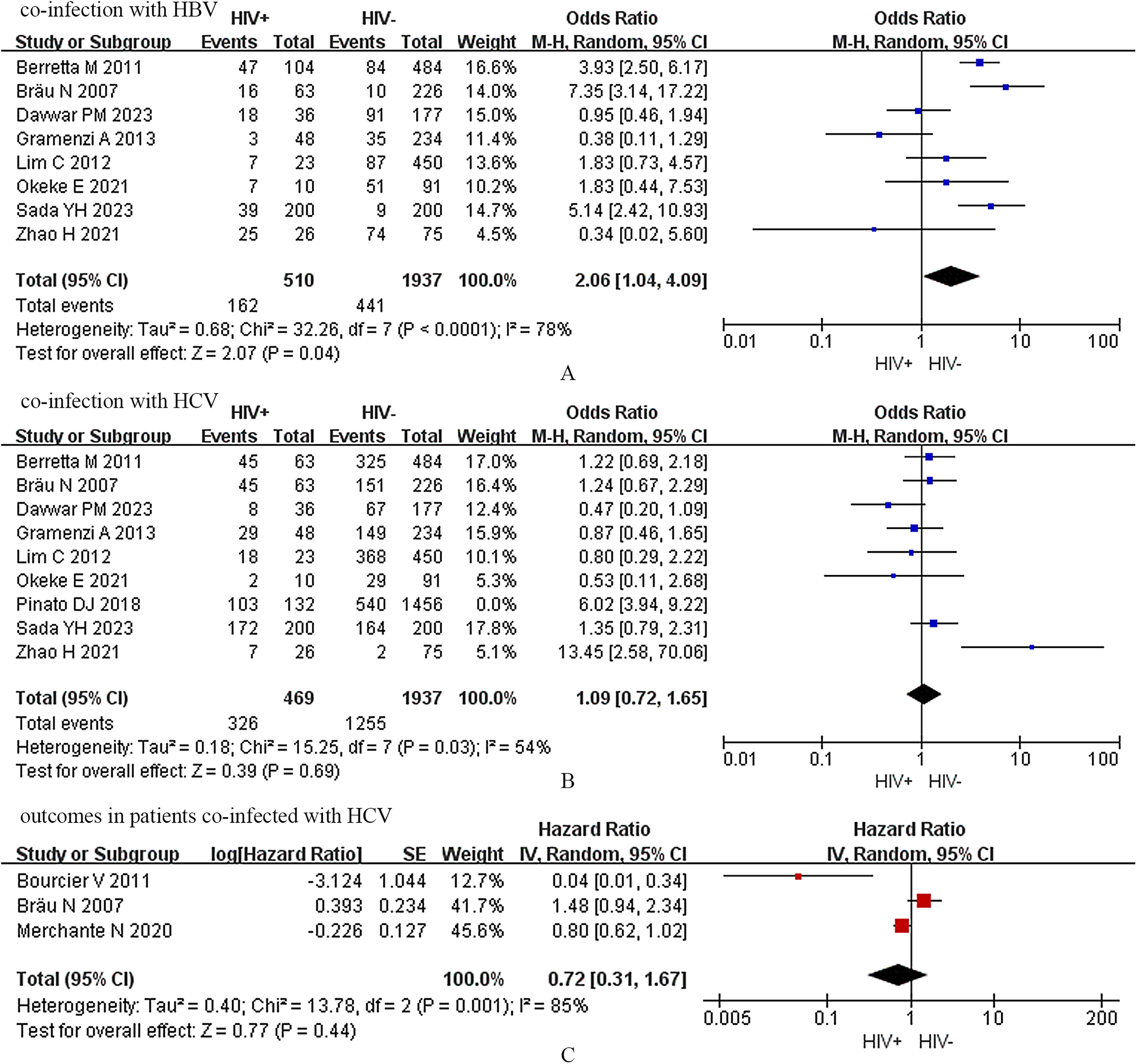
Subgroup analysis of patients co-infected with HCV or HBV.
Prognosis of patients
The final results showed that in the HCC population, the prognosis of HIV-infected patients was significantly worse than that of HIV non-infected patients (HR = 0.71, 95% CI = 0.63 to 0.79, I2 =29%, P < .01). (Fig. 5)

Patient survival.
Publication bias and sensitivity analysis
Funnel plots were used to assess publication bias. Figure 6 showed that the funnel plot showed a roughly symmetrical pattern, indicating that publication bias had a small impact on this study. Sensitivity analyses were performed by repeating the analysis, excluding one study at a time. If the statistical significance was consistent between the results of each analysis, the results were proved to be relatively stable.
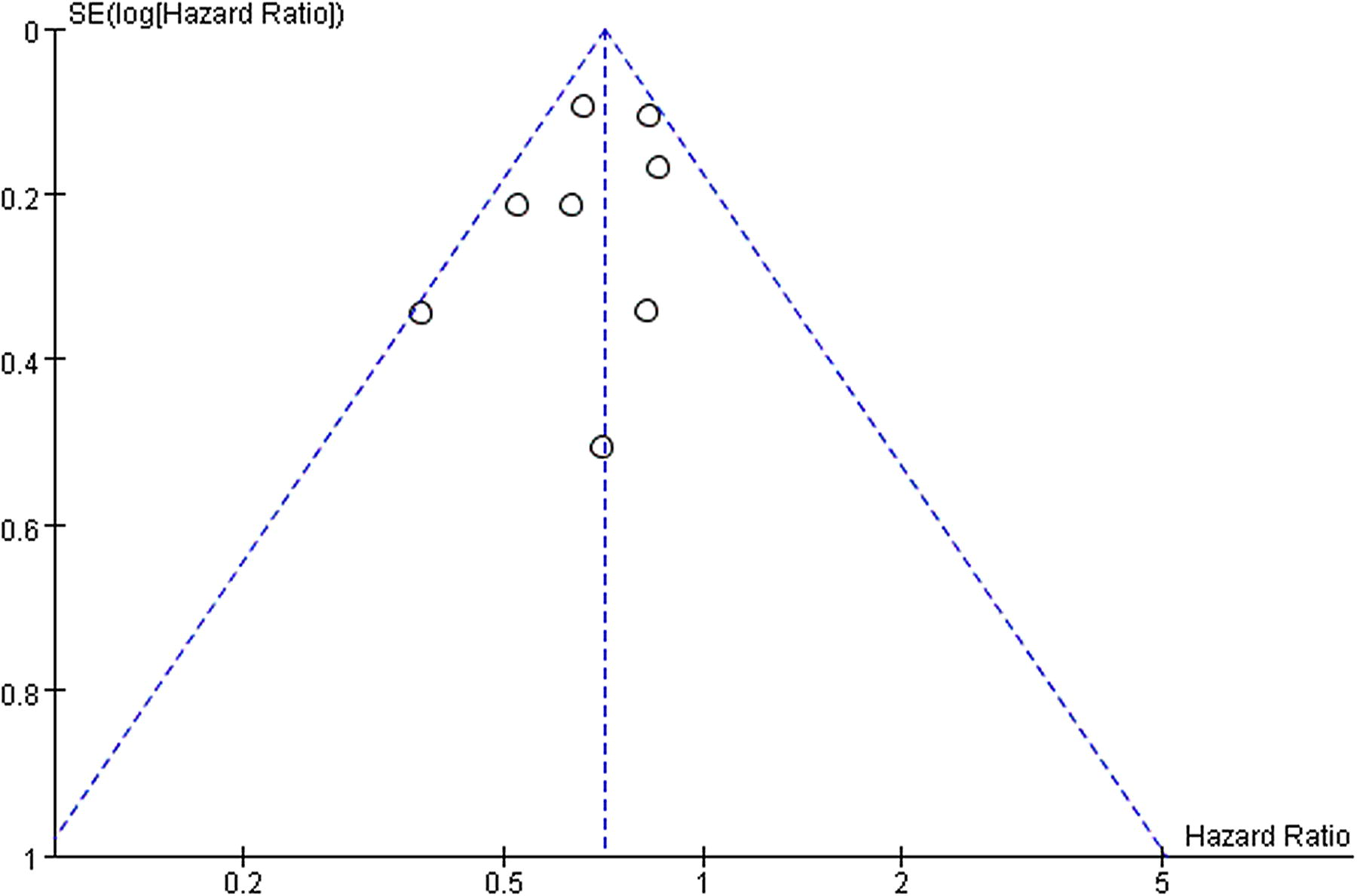
Funnel plot.
Discussion
This study analyzed data from 4544 subjects across seven countries to assess the impact of HIV status on the clinical features and prognosis of HCC. After pooled analyses, we found no significant differences in baseline characteristics between groups, except that HIV patients were generally younger. Further survival analysis showed that the HIV-positive group exhibited a poorer prognosis.
Our study found that HIV-associated HCC patients were younger. Possibly, this was due to the immunomodulatory effect of HIV, which might accelerate the progression of liver fibrosis and reduce the latency period for HCC in HIV patients.26,27 This also supported the observed increase in HCC incidence among HIV-infected individuals. In addition, the long-term dysregulation of the immune system caused by HIV infection also affected the biological behavior of tumors, leading to higher tumor aggressiveness. 28 However, in our study, no correlation was found between HIV infection and portal vein infiltration, multiple tumors in the liver, or extrahepatic metastasis.
HBV is a well-known risk factor for HCC, primarily due to immune-mediated inflammation and genetic instability from the integration of viral DNA into the host genome.29,30 Compared with individuals infected with HIV alone, individuals co-infected with HBV are more likely to develop advanced HCC and have a higher mortality rate.31–33 In HCC patients with HBV infection, combined with anti-HBV therapy has been shown to delay the progression of HCC and the occurrence of decompensated cirrhosis, and therefore improve patient survival. 34 Interestingly, our study noted a marginally significant difference in the rate of HBV infection between the two groups (I2 = 78%, P = .04), which might contribute to the poorer prognosis observed in the HIV-positive group. For HCV, in previous studies, HIV and HCV co-infection was associated with a lower sustained virologic response, a faster progression of cirrhosis, and a higher prevalence of HCC.35–37 In this context, patients with HCC often presented with an invasive growth pattern, which is associated with faster tumor progression and poorer survival outcomes. 12 However, our study did not observe an impact of HIV status on the prognosis in the HCV-infected HCC population.
However, in our study, there were not enough data to support our analysis of whether there were differences in treatment modalities between the two groups. Other related studies have shown that patients without HIV have a higher percentage of optimal supportive care, 38 (60% versus 38%, P = .02). This disparity in treatment access could be a factor influencing outcomes. But at the same time, HIV patients did not translate into better outcomes after improved treatment access, and the survival rate was still lower than that of the control group. 39 At present, the choice of optimal treatment modalities for this population requires further exploration.
In terms of how to improve the prognosis of HIV patients with HCC, HAART appears to be an effective option. The presence of viremia is a significant risk factor for death. 40 Although there is no direct association between CD4+T cell count and outcome in HIV patients with HCC, 17 patients with undetectable levels of HIV RNA in blood have longer median survival compared to those with viremia, 34 emphasizing the necessity of early initiation of HAART. In addition, HAART plays a role in down-regulating liver inflammation and delaying the progression of liver fibrosis in the presence of HBV co-infection.41–43
Our study also had some limitations: First, only 11 studies involving 4544 participants were included. For some of the other things we care about, such as serum liver function-related indicators, alpha-fetoprotein levels, and models for end-stage liver disease scores, there is not enough data available for analysis. Second, the survival analysis in this study only included overall survival and lacked short-term prognostic indicators. Third, there was a lack of sufficient data to support further subgroup analyses. Therefore, it is worthy of further exploration by more comprehensive and high-quality prospective studies.
Overall, HIV patients were younger at initial HCC diagnosis and had worse survival outcomes, potentially due to the effects of HIV infection itself, higher rates of HBV co-infection, and variations in treatment approaches. Therefore, such patients require effective antiviral therapy and carefully selected treatment strategies to improve their prognosis.
Footnotes
Acknowledgment
The authors acknowledge all the authors whose publications are referred to in their article.
Authors’ Contributions
Y.C.: Conception and design, administrative support, Y.H.D. and Y.C.: Provision of study materials or patients. Y.H.D. and F.P.G.: Collection and assembly of data. Y.H.D. and F.P.G.: Data analysis and interpretation. Y.H.D.: First article writing. Y.H.D., F.P.G., and Y.C.: Final approval of the article.
Data Availability Statement
All the data could be found in the included studies.
Disclosure Statement
All authors declare that they have no conflict of interest or financial ties to disclose.
Funding Information
No funding was received for this article.