
Abstract
Background:
Small bowel bleeding (SB) comprises 5%–10% of gastrointestinal (GI) bleeding cases. This article describes the staged retrograde intraoperative enteroscopy (SRIE) surgical technique for the etiological diagnosis and treatment of small bowel bleeding.
Methods:
SRIE was performed on patients with persistent SB at a quaternary university hospital in Brazil from 2020 to 2023. The technique is described in 5 steps, alongside visual aids, including images and a depicting a portion of the procedure. Patients presenting with confirmed coagulopathies, pregnancy, or unwillingness for surgery were excluded. Surgical procedures were performed after informed consent.
Case Series:
Four participants were submitted to SRIE, including 2 females (64 and 83 years old), and 2 males (46 and 57 years old). Three out of four (75%) of the patients received a confirmed diagnosis of GI bleeding, attributed to angioectasia, acquired von Willebrand disease, and vitamin K deficiency. SRIE was conducted via enterotomy, involving a subsequent insufflation-inspection-deflation of 10 to 10 cm segments of the small bowel (Steps 1 to 5). The procedure was successfully executed in all four patients without complications, allowing confirmation of the etiological diagnosis of SB or exclusion of anatomical causes of hemorrhage.
Conclusions:
SRIE is a valuable but invasive tool for assessing SB hemorrhage when conventional imaging falls short. When performed systematically and standardized, it allows accurate visualization of SB using a standard endoscope.
Introduction
Small bowel (SB) bleeding refers to gastrointestinal (GI) bleeding occurring anywhere between the duodenal papilla and the ileocecal valve. 1 Despite improvements in imaging techniques, SB bleeding remains a challenging diagnosis, constituting 5% to 10% of all GI hemorrhage cases.1,2 Diagnosis is considered in patients presenting GI bleeding symptoms, yet no source of hemorrhage is detected following upper endoscopy and colonoscopy.1,2 Angioectasia is the most common lesion identified in SB bleeding cases after extensive investigation, particularly in individuals aged 40 and above.1,3
Evaluation of SB is possible through different diagnostic procedures. These include push enteroscpy, an extended upper endoscopy, and deep enteroscopy, which employs balloon-assisted endoscopic techniques.1,4 Limitations include equipment and personnel availability, image range, and equipment maneuverability. Intraoperative enteroscopy is regarded as the most reliable method, providing precise evaluation of the complete organ. It is an invasive procedure performed during laparotomy. 1 If performed without a systematic approach, it can result in challenges such as reduced sensitivity, attributed to inadequately evaluated areas, and intestinal distension, posing closure difficulties. This study details the utilization of staged retrograde intraoperative enteroscopy (SRIE) for persistent SB bleeding.
Methods
Our study provides a detailed description of the SRIE surgical technique, developed, and performed at the quaternary university hospital from the Federal University of São Paulo (Brazil). Surgeries were performed in operating theaters under aseptic conditions from 2020 to 2023. Before surgery, all patients were given informed consent and received preoperative antibiotic prophylaxis, along with general anesthesia and orotracheal intubation.
Patient selection criteria were established based on high-risk SB bleeding, despite normal findings on endoscopy and colonoscopy, alongside persistent GI bleeding, sustained decline in hemoglobin levels, or compensated hemodynamic instability. The study imposed no age or gender restrictions but excluded individuals with confirmed coagulopathies, pregnant women, and those unwilling to undergo surgical intervention.
Intraoperative enteroscopy was performed with an Olympus® Gastroscope GIF-Q150, partially protected with a sterile polyethylene cover (the same used in the laparoscopic telescope). The technique is described step by step and supplemented with illustrations produced by the researchers and a video recorded during one of the procedures. Adherence to the Surgical Technique Reporting Checklist and Standards guided the report of the surgical technique. 5
Patient selection and preoperative assessment
The study included adult patients of both sexes who were hemodynamically stable, presented with persistent GI bleeding, had normal findings on both endoscopy, colonoscopy, and computed tomography examinations, and were suspected of having small bowel hemorrhage.
Prior to the procedure, the patient must have undergone an upper digestive endoscopy and colonoscopy in the operating room. Informed consent is obtained. Bowel cleansing of the small intestine and colon is achieved using mannitol. No other special equipment is required aside from the endoscopic device and sterile plastic protector.
Intraoperative steps
The SRIE was performed in five steps:
Step 1. The surgical team consists of the surgeon, assistant, endoscopist, anesthesiologist, and scrub nurse. The patient is placed in a supine horizontal position under general anesthesia, with the endoscopist positioned ideally on the patient’s right side. Aseptic measures, including antisepsis and establishment of sterile fields, are carried out. No specific intraoperative monitoring is necessary. A midline supra and infra umbilical incision is made using a scalpel, followed by dissection to the aponeurosis. Careful aponeurosis opening with a scalpel allows access to the peritoneal cavity. Laparoscopic access would be feasible, although extremely complex. A thorough examination of the peritoneal cavity is conducted to identify external hotspots suggesting active bleeding, hematomas, telangiectasias, and neoplasms in the intestinal loop wall. Inspection and measurement of bowel loops are performed from the angle of Treitz to the ileocecal valve. A point for enterotomy in the SB loop is selected at the midpoint (it is advisable to perform two enterotomies in intestines longer than 3 meters to ensure complete visualization). We do not recommend the use of visual intraluminal hematomas to define a point for enterotomy, as blood may flow back and forth depending on peristaltism or mannitol ingestion, and more than one lesion may coexist, thus always necessitating the visualization of the entire intestine lumen.
Step 2. A 1 cm longitudinal antimesenteric enterotomy is performed using a scalpel (Fig. 1), followed by careful introduction of an endoscope to prevent enteric spillage, with external sterile plastic protection for device manipulation. After entering the loop, the entire jejunum is introduced proximally into the device until reaching the angle of Treitz, creating a “telescoped” or “accordion” effect. A careful introduction is performed to prevent mucosal injuries, deserosalization, excessive mesentery traction, or spillage.

Longitudinal enterotomy with scalpel.
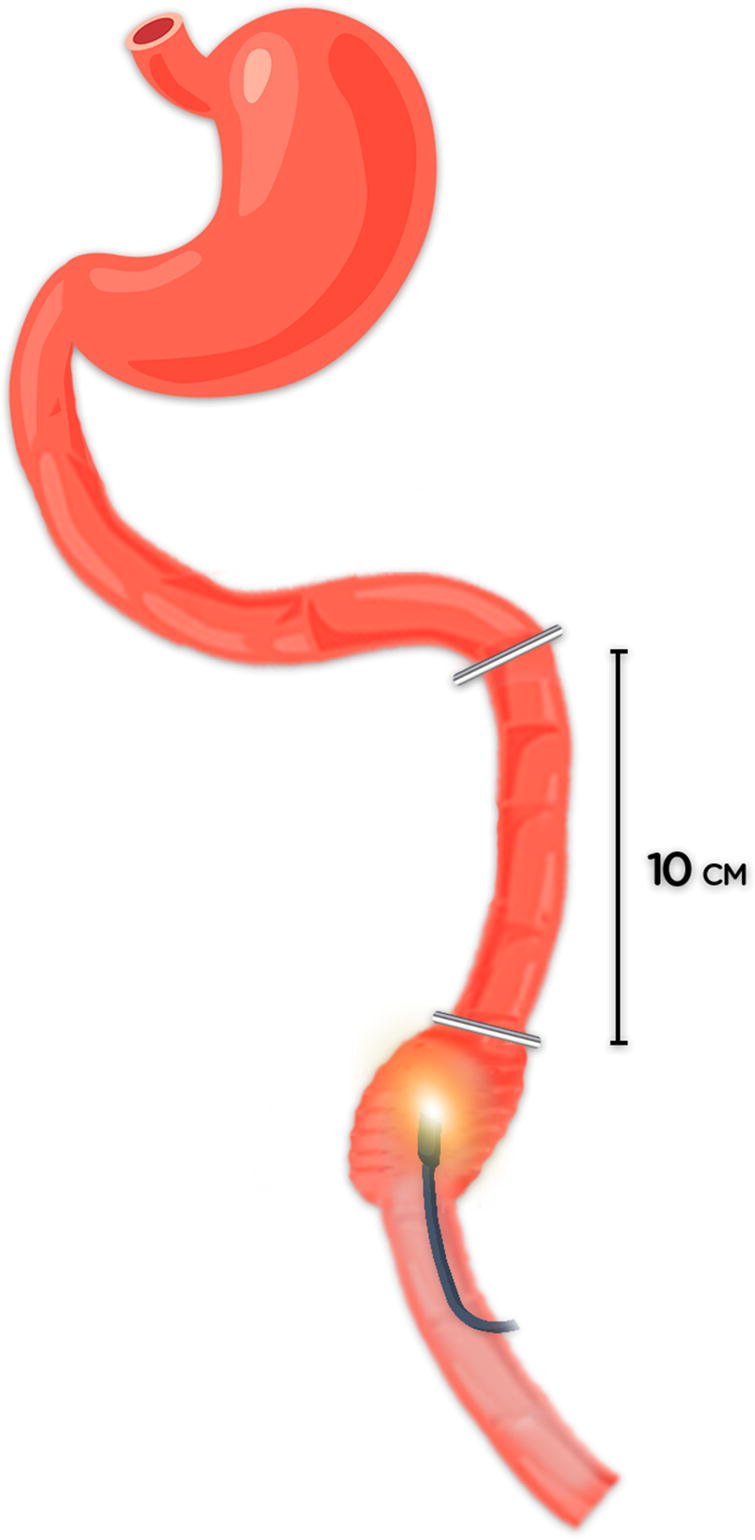
Step 3. After introducing the endoscope into the proximal half of the SB without gas inflating, an intestinal clamp is placed between the angle of Treitz and the tip of the endoscope. The endoscope is pinched with fingers over the intestine, and pulled gently 10 cm from the clamp, followed by gas inflation for complete mucosal visualization of a short bowel segment (Fig. 2). The surgeon and the endoscopist must look at the monitor and confirm whether the evaluated segment has any changes. After deflation, a new intestinal clamp is placed at the distal end of the evaluated segment (Fig. 3), and the process is repeated until complete visualization of the entire half of the SB is achieved (Supplementary Video S1). To ensure surgical quality and consistency, standardized surgical training is advisable, as well as previous multidisciplinary consultations with the endoscopy team.

Pinching of the small bowel 10 cm from the proximal clamp and gas insufflation, allowing for complete mucosal visualization.
After deflation, a new intestinal clamp is placed at the other end of the evaluated segment, and the process is repeated until complete visualization of the entire half of the small intestine is achieved.
Step 4. The same process is repeated in the distal direction (the remaining half of the jejunum and ileum), with the endoscopist changing position to the opposite side of the patient if necessary. The examination starts at the ileocecal valve level, visualizing the entire ileal and distal jejunal mucosa up to the midpoint where the enterotomy was performed. Depending on intraoperative findings, endoscopic or surgical treatment can be done (e.g., argon plasma coagulation or bowel resection).
Step 5. The endoscope is removed, and enterorrhaphy is performed using a continuous 3-0 polydioxanone suture, with careful inspection for signs of stenosis or leakage. Hemostasis is assessed, materials are counted, followed by the closure of the aponeurosis using continuous small bites of polydioxanone 2-0 suture, and the skin with subcuticular monoamide 4-0 stitches. The estimated operative time is 1 hour. This technique is easily reproducible, and allows complete bowel evaluation, both via endoscopy camera and direct visualization by the surgeon, in a detailed, systematic manner and without bowel distention.
Postoperative care
Chosen criteria for success in implementing SRIE encompassed the following: (1) identification of the bleeding source within the SB; (2) accurate localization and treatment of the SB lesion; and (3) exclusion of SB as the source of bleeding when the exam was unremarkable, and an alternative diagnosis better explained the case. Additionally, improvements in recurrence of SB, short-term mortality, and reduction in hospital stay duration were evaluated.
Following the procedure, patients were monitored for a minimum of 24 hours in either the intensive care unit or ward, depending on their hemodynamic stability. Monitoring aimed to detect potential complications arising from the operation, recurrence or persistence of SB bleeding, changes in hematological parameters, enterorrhaphy dehiscence, and potential thrombotic complications. Continuous monitoring of vital signs was conducted, with periodic assessments assisted by the nursing team.
Patients were cleared to start feeding after 24 hours of stable clinical and laboratory conditions. Hematocrit levels were monitored rigorously at 6- or 8-hour intervals, along with other blood parameters. Transfusion support, such as red blood cells, platelets, and cryoprecipitate, was provided based on laboratory assessments and multidisciplinary team consultations. Thrombotic events were prevented with heparin administration starting 12 to 24 hours after surgery.
Although intraoperative enteroscopy carries inherent risks, including reported mortality rates of 17%, 1 none of the 4 patients in our study encountered postoperative complications, including recurrence of bleeding, enterorrhaphy dehiscence, and incisional hernias. Potential concerns include prolonged ileus, serosal damage, and mesenteric vessel avulsion. 1 Patients underwent follow-up visits at 1-week, 1-month, and 6-month intervals after the procedure.
Case series
Four patients, comprising 2 females (64 and 83 years old), and 2 males (46 and 57 years old) were selected for SRIE. Seventy-five percent obtained a definitive etiological after SRIE. Their diagnoses were attributed to angioectasia, acquired von Willebrand disease (AvWD), and vitamin K deficiency. SRIE was successfully conducted in all patients via the 5 Steps procedure: sequential insufflation-inspection—deflation of 10 to 10 cm segments of the SB.
The first procedure, performed on a 64-year-old female with a history of chronic lymphocytic leukemia and recurrent episodes of melaena, resulted in a diagnosis of AvWD after a new and more specific investigation following a normal enteroscopy. Another patient was also later diagnosed with coagulopathy as the cause of hemorrhage: a 57-year-old male with a history of alcoholism and cirrhosis, who had no remarkable findings during the procedure and presented hematomas throughout the small bowel. New exams were conducted and concluded that the SB bleeding was attributed to vitamin K deficiency associated with liver failure, but normal international normalized ratio (INR) values. The third procedure, leading to the confirmation of an etiological diagnosis of SB bleeding, was conducted on a 67-year-old male diagnosed with Kaposi sarcoma. It revealed jejunal angioectasia as the underlying cause of the hemorrhage. In the fourth case, an 83-year-old woman underwent an enteroscopy, which did not reveal any significant findings. Subsequently, she was diagnosed with GI bleeding stemming from diverticular disease. None of the cases reported in this study resulted in mortality. No death resulted from the cases reported in this study.
Conclusion
SRIE in 5 Steps is an invasive yet valuable diagnostic procedure for assessing SB hemorrhage, especially when conventional imaging fails to identify the bleeding source. It is easily reproducible and does not require bowel distension. Providing visualization of the entire small bowel aids in confirming or excluding potential causes of GI bleeding with greater precision than other methods. Therefore, in cases where less invasive endoscopic techniques are unavailable or ineffective, intraoperative enteroscopy should be considered for SB assessment. However, further studies with larger patient cohorts are needed to validate its success or failure rates.
Footnotes
Authors’ Contributions
M.M.N.A.: Conceptualization, methodology, investigation, resources, writing—original draft. D.N.: Visualization, supervision, project administration. A.M.M.F.: Writing—review and editing, visualization. J.D.: Writing—review and editing, visualization. N.A.: Writing—review and editing, visualization. K.R.P.: writing—review and editing, visualization. L.D.G.: Project administration, supervision. D.A.: Project administration, supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.