
Abstract
Background:
The advancement in medical care has led to an increase in patients with acute cholecystitis (AC) and cardiopulmonary comorbidities referred for surgery. Grade II AC, according to Tokyo Guidelines in 2018 (TG18), is characterized by severe local inflammation with no systemic affection. The optimal treatment for patients with high-risk grade II AC has not yet been clearly established, which is still a dilemma. For these patients, laparoscopic cholecystectomy (LC), despite being the only definitive treatment, is still a challenge. The introduction of percutaneous cholecystostomy as a temporary minimally invasive alternative technique allows an immediate gallbladder decompression with a rapid clinical improvement. However, the next step after percutaneous transhepatic gall bladder drainage (PTGBD) in these high-risk patients is still a debate, with no definitive consensus about the ideal treatment of choice as well as its optimal timing. In our study, we followed a treatment algorithm for high-risk patients that involved early gallbladder decompression by PTGBD, followed by LC at different intervals once the patient is considered fit for surgery.
Method:
A retrospective study of 58 patients with high-risk grade II AC with cardiopulmonary comorbidity from our medical records was included. They were managed initially with PTGBD, an LC was then performed either within 7 days after drain insertion (early group, 26 patients), while an LC was performed later for the remaining patients within 6–8 weeks after PTGBD (late group, 32 patients). The results of the two groups were analyzed.
Result:
Procalcitonin and C-reactive protein were significantly higher in the late group. No significant difference was found between both groups with regard to operative time, PTGBD-related complications, and major perioperative complications. Timing after PTGBD did not affect the incidence of operative complications. Total hospital stay was significantly shorter in the early group.
Conclusion:
PTGBD is a safe initial intervention for high-risk patients with AC with a low morbidity and high success rate. Urgent LC after PTGBD can be performed safely for well-selected high-risk patients with the timing of surgery is personalized according to each patient’s clinical situation. Early LC (after PTGBD) has the advantage of shorter hospital stay, low cost, as well as avoiding the risk of biliary complications and mortality if waiting a delayed surgery with no significant difference in morbidity compared with late LC.
Introduction
Although there was initial fear of early laparoscopic cholecystectomy (LC) for acute cholecystitis (AC), surgeons began to recognize its advantages; the edematous plane facilitates easy dissection, single-stage definitive surgery shortens the duration of morbidity, and early surgery prevents recurrent biliary events and prevents local gall bladder complications. 1
The advancement of medical care has led to an increase in patients with AC with multiple comorbidities referred for surgery. Unfortunately, these patients often pose a combined high medical and surgical risk. Previously, this high risk has resulted in most of the patients being managed conservatively but, unfortunately, with high recurrence rates of biliary symptoms and incidence of local complications, which are more hazardous in these high-risk patients. 2
According to the updated version of Tokyo Guidelines in 2018 (TG18), 3 urgent LC is recommended in TG18 for grade II AC with low-risk (Charlson Comorbidity Index (CCI) ≤5 and American Society of Anesthesiologists Physical Status [ASA-PS] ≤2), while the optimal treatment strategy for patients with high-risk grade II AC (CCI ≥6 or ASA-PS ≥3) has not yet been clearly established, which is still a dilemma in these patients. 4 For these patients, LC, despite being the only definitive treatment, is still a challenge. This was overcome by the introduction of percutaneous transhepatic gallbladder drainage (PTGBD).5,6 However, the next step after PTGBD in these high-risk patients is still a debate. 7
Different studies in the literature approached AC management in unfit patients due to different comorbidities with wide variation in the treatment policy regarding choice of treatment strategy—surgery versus PTGBD as well as the timing of surgery whether early or late cholecystectomy. 8 However, there are yet no studies that focus on patients with grade II AC with mainly cardiopulmonary comorbidities. In our study, we evaluated a treatment algorithm that involved initial gallbladder decompression by PTGBD in high-risk cardiopulmonary patients with grade II AC, followed by LC at different intervals. The results were analyzed in this study.
Materials and Methods
Patients’ selection
In this retrospective, data from the AC database of General Surgery Department in Alexandria University Main Hospital and some nongovernmental hospitals were analyzed. The study was approved by the ethics committee and review board at our institute: IRB NO: 00012098.
Between January 2018 and December 2023, all patients diagnosed with AC (according to TG18) and who subsequantly underwent PTGBD followed by LC in different intervals were eligible for the present study. Patients with grade I/III AC, patients with grade II AC treated only with antibiotics and/or PTGBD without subsequent surgery, patients who underwent open cholecystectomy from the beginning, patients with associated Common Bile Duct (CBD) stones, Mirrizi syndrome, biliary pancreatitis, and previous acute attacks were excluded (due to superadded anticipated difficulty). All the available data were retrieved for statistical analysis.
Diagnosis of AC
In our institute, AC is diagnosed and graded mainly using the TG18 criteria. 3 Ultrasound abdomen was the main diagnostic modality. A contrast-enhanced abdominal computed tomography scan was done if the findings on Ultra-Sound (US) examination were inconclusive or a suspected local Gall Bladder (GB) complication was suspected on US basis. Magnetic resonance cholangiopancreatography (MRCP) was ordered in patients with jaundice to exclude CBD stones/Mirrizi syndrome.
Initial management of AC/indication of subsequent LC or PTGBD
Our hospital, being a referral tertiary center, serves a large number of public hospitals. Almost all of our patients with AC started antibiotic treatment as a part of conservative approach, prescribed to them at their local hospitals and clinics. Their referral usually represents failed medical treatment, and consequently, an immediate intervention has to be performed on admission.
For patients with high-risk grade II AC included in the study with associated cardiopulmonary disease, in addition to continuing conservative management including mainly broad spectrum antibiotics, urgent cardiopulmonary and anesthesia consultation were performed on admission for surgical risk assessment. Urgent LC was the rule if the patient can tolerate surgery (excluded from study population); otherwise, initial PTGBD was performed as a preliminary management to relieve/prevent sepsis and to give time for evaluating/optimizing the cardiopulmonary condition according to strict medical recommendations. Later, at least 48 hours after PTGBD, a combined surgical and secondary cardiopulmonary/anesthesia consultation was performed to reassess the patient eligibility for surgery.
According to the policy adopted by our institute consultants, patient fitness after initial PTGBD was defined by the following criteria:
Sepsis resolution depending on triple assessment, clinical examination (resolution of abdominal pain and fever), laboratory workup (declining leukocytosis and C-reactive protein [CRP]), as well as a follow-up US abdomen to assess the drain position and exclude a superadded local complication.9,10 Cardiopulmonary fitness for surgery, which is defined by the cardiopulmonary/anesthesia team in the managing hospital.2,11
LC was then performed for eligible patients in the same hospital admission within 7 days after PTGBD (early group); otherwise unfit patients were discharged (if medically stable) and readmitted within 4–6 weeks later for elective surgery once considered fit (late group). The timing of readmission and subsequent LC was determined individually according to each patient’s condition. The PTGBD tube was kept in place and removed during cholecystectomy. PTGBD was considered the definitive treatment strategy for unfit patients (excluded from study population). 12
PTGBD management
PTGBD was performed, on admission, for patients with high-risk grade II AC who were primarily unfit for emergency LC, in the interventional radiology unit under the ultrasonography guidance and local anesthesia, with or without fluoroscopy. Transhepatic approach was used in most of our cases. The aspirated material was then sent for aerobic and anaerobic culture. At 24–48 hours after placement, a follow-up ultrasound was performed to check the position of the catheter and reassess the GB status.
Preoperative evaluation and preparation
Was of extreme importance to prepare the patient for surgery. Specific cardiopulmonary workup was done as ordered by the cardiopulmonary consultants including mainly resting electrocardiogram, transthoracic echocardiography (for cardiac patients), and pulmonary function tests (for pulmonary patients).
Surgical management (anesthesia/surgical principles)
The technique for AC was the standard four-ports LC with combined epidural/general anesthesia. At least one experienced laparoscopic hepatobiliary expert surgeon participated in every operation. Low-pressure pneumoperitoneum was adopted. Standard/subtotal LC was done according to the operative difficulty. The percutaneous drain was kept in situ to help in GB traction till the end of the operation. Intraoperative cholangiogram (IOC) was available in most cases to visualize the biliary anatomy. The decision to convert to open surgery was taken according to intraoperative difficulties. Abdominal drains were routinely placed in the gallbladder bed. Antibiotic therapy (according to PTGBD culture) was continued postoperatively.
Operative details were recorded with special attention to intraoperative difficulties, operative time, and complications. Follow-up visits in the outpatient clinic were scheduled routinely 3, 7, and 10 days after the patient’s discharge.
Postoperative care
With a cardiopulmonary specialist, respiratory therapist for patients with chronic obstructive pulmonary disease (COPD) was extremely important in our study. Postoperative pain management with epidural analgesia allowed early return of bowel function, early mobilization, and reducing incidence of postoperative nausea.
Outcome measurements and definitions
Basic patient’s characteristics data were recorded upon admission, namely, age, sex, body mass index (BMI), ASA-PS, preoperative comorbidities, AC severity (based on TG18), and laboratory workup were collected. PTGBD-related complications such as drain dislodgment, bile leak, liver hematomas, and intra-abdominal bleeding were analyzed. The degree of operative difficulty was quantified by reviewing the operative time, the need for intraoperative cholangiography, the need to perform a subtotal instead of total cholecystectomy, intraoperative complications, and rate of open conversion. The hospital stay and postoperative results were also analyzed.
Statistical analysis
We used IBM SPSS Statistics for Windows, version 25.0, for statistical analysis. P values <.05 were regarded as statistically significant. Frequencies and percentages were used to summarize the data for categorical variables. If the data for the quantitative variables were normally distributed, they were summarized as mean and standard deviation or, if not, as median and interquartile range. Shapiro–Wilk’s test was used to evaluate normally distributed data (P > .05). An independent samples t-test was used to analyze continuously distributed data; otherwise, the Mann–Whitney U test was employed. For categorical parameters, the Fisher’s exact test is employed.
Results
A total of 306 consecutive patients with diagnosis of AC (according to TG18), between January 2018 and December 2023, were eligible for the study. Fifty-eight patients with high-risk grade II AC with cardiopulmonary comorbidity who were treated initially with PTGBD followed by early LC within 7 days after drain insertion (early group/26 cases) or 4–6 weeks later after drain insertion (late group/32 cases) with overall mean age of 59.9 years and mean BMI of 28.87 kg/m2 were analyzed (Fig. 1).
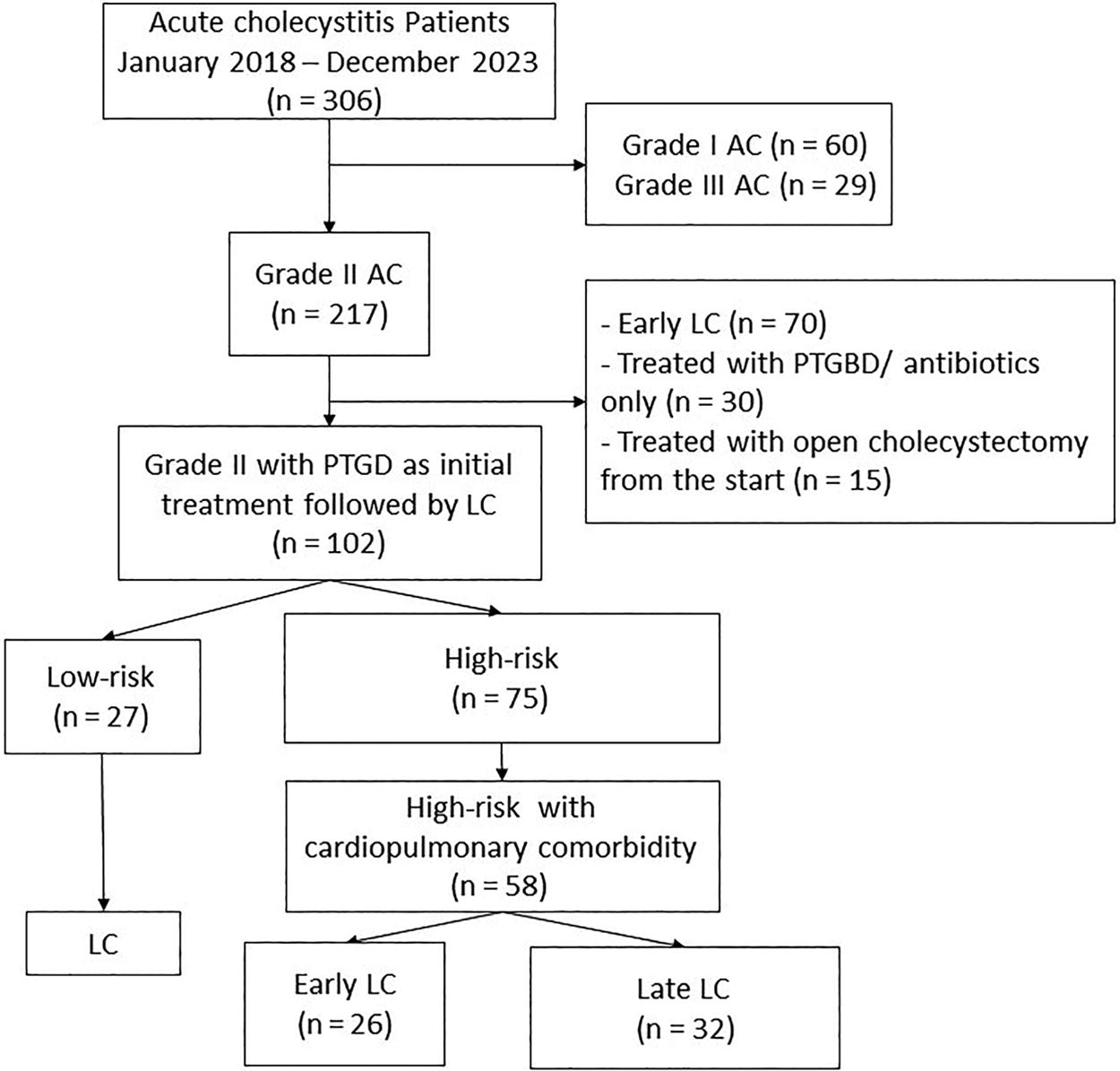
Patient selection flowchart according to the inclusion exclusion criteria.
Patients in both groups had no significant difference in their demographic characteristics as shown in Table 1.
Comparison Between the Two Studied Groups According to the Demographic Data
All values presented in number (percentage) unless indicated otherwise.
Mean ± standard deviation.
BMI, body mass index.
The prevalence of preoperative comorbidities was not significantly different between the early and late groups as shown in Table 2.
Comparison Between the Studied Groups According to Preoperative Comorbidities
All values presented in number (percentage) unless indicated otherwise.
Median (range).
ASA-PS, American Society of Anesthesiologists Physical Status.
A combined secondary assessment 48 hours after PTGBD was the base upon which the surgical decision was taken. On comparing laboratory results 48 hours post PTGBD between both groups, CRP and procalcitonin levels were significantly lower in the early group compared with the late group, while other laboratory workup was comparable (Tables 3, 4). No significant difference was found between the ultrasound findings among both groups (Table 5).
Comparison Between the Studied Groups According to Laboratory Workup
All values presented in median (range).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; INR, international normalized ratio.
Comparison Between the Studied Groups According to Preoperative Sepsis Laboratory Workup
All values presented in mean ± standard deviation.
CRP, C-reactive protein; WBC, white blood cells.
Comparison Between the Studied Groups According to Preoperative Ultrasound Findings
All values presented in number (percentage).
PTGBD-related, surgical, and postoperative outcomes were compared in both groups. With regard to PTGBD-related complications, one patient with atrial fibrillation, in the early group, on drain insertion suffered a subcapsular liver hematoma. Drain dislodgement occurred in one patient in the late group; he was followed clinically on outpatient basis with drain reinsertion on outpatient basis with nonsignificant residual collection. PTGBD-related complications were not significantly different between both groups (Table 6).
Comparison Between the Studied Groups According to PTGBD Complications
All values presented in number (percentage) unless indicated otherwise.
Operative difficulty and intra/postoperative major complications were comparable between the two groups with no statistical difference. Intraoperative difficulty was encountered in 6/26 (23%) patients of the early group with 3 patients of them ended in subtotal cholecystectomy compared with 8/32 (25%) patients in the late group with 5 patients of them ended in subtotal cholecystectomy.
No significant differences were found between the studied groups with regard to intraoperative complications (Table 7). Bile duct injuries occurred in two patients in the early group compared with three patients in the late group. The conversion rate to open surgery was comparable in the two groups; three patients in the early group were converted to open laparotomy (two patients due to bile duct injury, 1 patient with difficult anatomy), while four patients were converted in the late group (three patients due to bile duct injury and one patient due to difficult anatomy making laparoscopy unsafe).
Comparison Between the Studied Groups According to Operative and Postoperative Results
All values presented in number (percentage) unless indicated otherwise.
Mean ± standard deviation.
Bowel injury occurred in one patient only in the late group during dissection of dense adhesions of the gallbladder; this patient was converted to open surgery due to difficult anatomy. Upon conversion and during dissection, a duodenal serosal injury was discovered and required a direct seromuscular suturing.
No significant difference was found between both groups with regard to postoperative complications. One patient was reoperated in the early group due to postoperative bleeding from the liver bed. Postoperative bile leak (diagnosed through the drains placed at surgery) occurred in one patient in the late group. MRCP was done revealing cystic duct stump clip slippage without any biliary track imaging, which was managed by Endoscopic retrograde cholangiopancreatography (ERCP) and stent insertion. Postoperative subhepatic collection occurred in two patients in the early group (managed conservatively) compared with five patients in the late group (two patients required US-guided drainage, while the remaining patients were managed conservatively).
For analytical purpose, the total morbidity time (Table 8) is subdivided into:
Comparison Between the Studied Groups According to Analysis of the Hospital Stay (in Days)
All values presented in mean ± standard deviation unless indicated otherwise.
Median (interquartile range).
AC, acute cholecystitis; PTGBD, percutaneous transhepatic gall bladder drainage.
Time between disease onset of the acute attack till hospital admission.
Time between hospital admission and PTGBD.
Time between PTGBD and clinical improvement.
Time between surgery and discharge (postoperative period).
Cases in the late group presented more significantly late to the ER compared with the early group. The recovery time after PTGBD was significantly longer in the late group compared with the early group. Total hospital stay was significantly longer in the late group more than the early group. The overall treatment period was significantly longer in the late group (including two admissions) compared with the early group.
Discussion
According to TG18, 3 the choice of treatment for grade II AC is individually personalized for each patient. Low-risk patients are offered a LC, while for high-risk patients, the optimal treatment is still not yet clearly established. For high risk patients, the proposed strategy in the TG18 is to perform elective LC after initial PTGBD. 3 However, sometimes still present the situation where a” high-risk” patient is considered fit for early LC. Wide discrepancy is found in managing patients with grade II AC with cardiopulmonary comorbidity owing to several factors: (a) an LC for AC possesses high operative morbidity and sometimes mortality especially in high-risk or critically ill patients 13 ; (b) the conservative approach still has high risk of developing local complications while awaiting an elective surgery 14 ; (c) choosing the appropriate timing of surgery after PTGBD is crucial as it is affected by the patient fitness in different intervals and anticipated operative difficulty 5 ; and (d) hemodynamic effects of pneumoperitoneum are especially accentuated in these patients which may affect their preexisting cardiopulmonary condition, making a laparoscopic surgery a challenge. 15
Several studies addressed patients with low-risk grade II AC with varying results.3,16,17 On the contrary, searching the literature, fewer studies with controversial results addressed high-risk grade II AC. Adopting PTGBD as a definitive treatment for high-risk patients, Cirocchi et al. 7 compared PTGBD as a definitive treatment versus emergency LC and concluded that PTGBD is burdened with a more incidence of complications and longer total hospital stay compared with emergency LC and thus recommended reserving PTGBD for patients with poor general conditions or as a bridge before elective surgery in patients whose general conditions can be improved later. Other studies observed more incidence of recurring biliary complications and even mortality among patients with AC who underwent PTGBD during the follow-up period.18,19 This indicated that LC is still the definitive treatment for gallbladder disease even for patients with acute attacks. Loozen et al. 20 assessed the safety of early LC for grade II AC in high-risk patients compared with elective LC following PTGBD. They concluded that, in well-selected patients with high-risk grade II AC, urgent LC can be performed with equivalent safety to elective LC following PTGBD, while Akyürek et al. 21 compared delayed LC with PTGBD followed by early LC in high-risk patients. The hospital stay as well as the cost was significantly less in the early group with comparable complications.
Recently, the World Society of Emergency Surgery suggested LC to be performed “as soon as possible, within a week from hospital admission and within ten days from the acute attack onset.” 22 Also, the TG18 proposed that early LC is recommended regardless of how much time has passed since onset, once the patient is considered fit for LC. 3 However, for patients with initial PTGBD for AC, there is no definite consensus and great discrepancy in the literature when it comes to the optimal timing of surgery after drain insertion. 5 This reveals that treatment choice for AC patients with intial PTGBD should be tailored individually in each patient according to both; the patient clinical status which is dynamic over time and the degree of surgeon experience to face anticipated operative difficulties. 23
In our hospital, we adopted an alternative algorithm for managing patients with grade II AC with high risk due to a cardiopulmonary comorbidity, in which combined approach was adopted; PTGBD, as an initial intervention for immediate sepsis relieve, is accompanied by parallel medical treatment and cardiopulmonary workup to decide the patient fitness. Once the patient becomes fit, an LC was performed with the drain kept in situ till the operation. PTGBD as an initial intervention was beneficial, allowing (a) alleviating abdominal symptoms with subsequent sepsis relive in a less invasive technique in comparison to emergency cholecystectomy, (b) providing time to optimize and prepare high-risk patients for subsequent surgery, (c) bile cultures withdrawn during percutaneous drain insertion helped us to choose the appropriate antibiotic in case of positive bile culture, and (d) if the cystic duct is patent, cholangiogram performed during drain insertion helped in visualizing the biliary tree. CBD stones discovered by cholangiogram were removed by ERCP.
For special patient populations included in the study who are vulnerable to adverse hemodynamic and ventilatory changes, special precautions were applied (Table 9).
AF, atrial fibrillation; AR, aortic resurge; COPD, chronic obstructive pulmonary diseases; MI, myocardial infarction; MR, mitral resurge, CPAP, Continuous positive airway pressure.
A low-pressure pneumoperitoneum (<12 mmHg) with reduced gas flow was beneficial to minimize hemodynamic changes.26,27
The efficacy of PTGBD in the treatment of critically ill patients with high-risk AC was illustrated in the literature.13,28 Clinical resolution of toxemia after PTGBD reaches 95% in the first 24–48 hours in the literature.29–31 In our study, immediate gallbladder decompression resulted in clinical resolution of toxemia in the included cases. When combined with cardiopulmonary assessment, 44% only were considered fit for early surgery, and other patients were postponed with drain in place till the definitive later LC. In the literature, the reported complications of PTGBD reach 5%–13%, including biliary peritonitis, bowel perforation, sepsis, pneumothorax, catheter dislodgment, and recurrent biliary events.32,33 In our study, comparable results were achieved; one patient suffered drain dislodgment that required drain reinsertion, while one patient suffered a subcapsular liver hematoma with no further sequel. No direct mortality related to PTGBD was encountered, but one case died later due to nonresolving sepsis while waiting delayed LC. There was no significant difference in the incidence of PTGBD-related complications between both groups.
Operative difficulty is a relative controversy that differs according to surgical experience and is a great source of hesitancy among surgeons to perform early surgery for AC. In our study, surgeries were adopted by experienced surgeons. We assessed operative difficulty in terms of operative time, conversion rate to open cholecystectomy, need to use IOC in case of difficult anatomy, ratio of subtotal/total cholecystectomies, and incidence of major operative complications.
Conversion from a laparoscopy to open approach is an important barrier that always makes surgeons hesitate to perform early AC surgeries; however, this is at the expense of the possibility of recurring acute exacerbations, which sometimes can be fatal.18,34,35 In the literature, wide variations are published in the conversion rates starting from <2% reaching up to 35% in complicated cases.36–39 In our study, total conversion rate was 5%, which is comparable with the published data in the literature, with no significant difference between the studied groups.
Wide variation is published in the literature comparing operative time of LC in different time intervals after PTGBD for acute attacks. Shorter operative time among delayed cholecystectomies after PTGBD was reported in many studies.36,40 On the contrary, longer operative time was reported in other publications.41,42 Tsumura et al. 43 found no significant difference in operative time. These variations are attributed mainly to the difference in the degree of gallbladder inflammation among different patients, different timing of surgery after drain insertion, and variable surgical experience. In our study, operative time was shorter in the early group with no significant difference between both groups.
IOC is available in our institute, with its use according to surgeon preference according to the intraoperative situation. Fourteen cases (24%) needed IOC due to difficult dissection aiming at reducing bile duct injuries (BDI). Subtotal cholecystectomy is usually resorted to as a reasonable alternative in difficult gallbladders if unclear biliary anatomy.44,45 In spite of available IOC and experienced surgeons, failure to complete cholecystectomy and perform a subtotal cholecystectomy was found in 8 patients (13.7%) among all included patients in the study. No significant difference was found between the two groups with regard to the need of IOC and subtotal cholecystectomies.
Anatomical difficulties are anticipated in AC. Higher incidences of common BDI are reported with variations, from <1% in surgeries for chronic cholecystitis46,47 to >30% in severely inflamed cases. 48 In the present study, overall incidence of BDI was 8% of all cases, which is comparable with published results in the literature, 49 with no significant difference between both groups (7.7% vs. 9.4%, P = 1). Postoperative bile leak occurred in one case in the late group, due to cystic duct stump slippage, and was managed by ERCP stenting.
The two groups showed comparable wound/port site infection and postoperative ileus. Subhepatic collection (biloma) occurred in seven patients (two vs. five patients, P = .442), and two of them required additional percutaneous ultrasound-guided drainage.
Proper case selection with continuous follow-up and preoperative assessment was crucial in our study. Postoperative morbidity from the medical point of view was satisfactory and comparable between both groups. Two patients of bronchial asthma, one in each group, suffered postoperative attack of wheezy chest, which was responsive to nebulizers with beta2 agonist, inhaled corticosteroids, and small doses of IV magnesium sulfate. Productive cough without fever occurred in one patient with COPD in the early group and was managed by good hydration and oral mucolytic drugs. One patient in the late group exhibited chest pain attack, and diagnosis of muscular noncardiac pain was confirmed and resolved using ketoralac ampule. Two patients suffered stable acute rapid atrial fibrillation (AF) in the early group, which was resolved using intravenous loading then maintenance amiodarone. One patient in the late group with mitral stenosis (MS) suffered attack of dyspnea due to lung congestion, IV diuretics, and noninvasive CPAP improved the condition. One patient with Diabetes mellitus (DM) suffered a hyperosmolar non-ketotic hyperglycemic attack with blood glucose level 408. The attack was resolved with the use of IV fluids and subcutaneous act rapid insulin.
No 30-day mortality was observed in both groups. On follow-up, obstructive jaundice due to CBD stones (diagnosed by MRCP) occurred in one patient 3 months later in the early group. The stone was successfully extracted through ERCP. Four patients died after PTGBD waiting for delayed LC; the first died due to nonresolving sepsis, while the other three patients died due to severe MS with an atrial thrombus, acute unstable AF, and severe obstructive lung disease, respectively. This result is satisfactory and adds more safety to our proposed algorithm in which proper patient selection and continuous assessment are crucial.
The late group had a total hospital stay significantly longer than the early group (7.1 vs. 6.12 days, P = .03). This was attributed mainly to the longer recovery time after PTGBD making those patient unfit for immediate LC. No significant difference was observed between both groups with regard to the postoperative hospital stay (P = .615). When adding the cost of the outpatient treatment and burden of the follow-up visits of the late group until readmission and performing late LC, we concluded that early LC has significantly lower cost in relation to late LC.
Overall results of the included cases were comparable with various studies comparing variable options for patients with high-risk AC.21,50,51 Nevertheless, this study still has some limitations. First, this was a retrospective study with relatively a small sample size, making it difficult to reach definitive treatment consensus. Second, a treatment strategy of high-risk patients differs among different surgical institutions, and lastly, selection bias was likely. Despite these drawbacks, to our knowledge, no previous studies have evaluated the safety and feasibility of urgent LC for grade II AC compared with elective LC after PTGBD with a focus on high-risk patients. Our study dealt only with high-risk patients due to cardiopulmonary cause rather than broadly speaking about high-risk causes in other published studies. To our knowledge, it is the first study to deal with such category.
Conclusion
Proper treatment choice is crucial for high-risk patients. PTGBD is a safe initial intervention for patients with high-risk AC with a low morbidity and high success rate allowing time for assessing the patient surgical risk before subsequent surgery while simultaneously eliminating sepsis in a relatively short time.
High-risk patient category is not an absolute contraindication for surgery. Urgent LC after PTGBD can be performed safely for well-selected high-risk patients with the timing of surgery being personalized according to each patient clinical situation. Early LC (after PTGBD) has the advantage of shorter hospital stay, low cost, as well as avoiding the risk of biliary complications and mortality while awaiting a delayed surgery.
Footnotes
Acknowledgments
The authors would like to acknowledge all Gastrointestinal tract (GIT) and liver surgery unit staff members at General Surgery Department, Alexandria University, Egypt, who managed most of these complex cases.
Authors’ Contributions
Every author contributed to this study. M.W., M.S., M.M., and M.R.E. wrote the article’s first draft. H.A. conducted the data analysis. M.W. and M.R.E. made the necessary changes and corrections. The figures and editing were done by M.W. and H.A. The final article was read and approved by all authors.
Ethics Approval and Consent to Participate
All procedures performed in this study involving human participants were by the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki Declaration and its later amendments or comparable ethical standards (IRB NO: 00012098).
Data Availability Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
Open access funding would be provided by The Science, Technology &Innovation Funding Authority in cooperation with The Egyptian Knowledge Bank.