
Abstract
Background:
Laparoscopic fundoplication is commonly performed in patients with neurological impairment. However, these patients often have spinal deformities that can complicate achieving a clear surgical view. This study aimed to identify factors associated with poor visibility in pediatric laparoscopic fundoplication.
Methods:
Operative videos, medical records, and radiographs of patients who underwent laparoscopic fundoplication between 2015 and 2023 were retrospectively reviewed. The videos were reviewed by two pediatric surgeons and classified into good or poor visibility groups. Age, sex, height, weight, history of abdominal surgery, lordosis, operative time, blood loss, and intraoperative complications were compared between the two groups. Lordosis was evaluated using the sagittal view of computed tomography images, and the anterior vertebral depth and abdominal thickness were measured to calculate the ratio.
Results:
Forty-one patients were included in this study. Based on the video review, the patients were classified into good (20 patients) and poor (21 patients) visibility groups. The median age, height, and weight were 6 years, 110 cm, and 16.1 kg, respectively. In the poor visibility group, 23.8% of patients had a history of abdominal surgery (P = .048). Additionally, the anterior vertebral depth to abdominal thickness ratios at the first and third lumbar vertebrae were significantly lower in the poor visibility group (P = .016 and P = .0018, respectively). There were no significant differences in the operative time, blood loss, or intraoperative complications between the two groups.
Conclusions:
Lordosis and a history of abdominal surgery may be risk factors for poor visibility in pediatric laparoscopic fundoplication.
Introduction
Laparoscopic fundoplication is a minimally invasive surgery that is commonly performed by pediatric surgeons.1–4 This procedure is particularly applicable for patients with neurological impairment who often have spinal deformities, such as scoliosis, which complicate the procedure by limiting the surgical field of view.5,6 Maintaining a clear view is crucial for the safe and smooth progression of laparoscopic surgery,7,8 and a 30° oblique scope is typically used to provide a broad overview. However, in patients with severe spinal deformities, there are frequent difficulties in achieving a bird’s eye view and stereoscopically recognizing the target because of the narrow intraperitoneal space. Despite these difficulties, there is a lack of research on which patient characteristics complicate visibility during laparoscopic surgery and how poor visibility affects surgical outcomes. Thus, this study aimed to identify factors related to poor visibility in the surgical field in pediatric laparoscopic fundoplication and examine their impact on surgical outcomes.
Methods
Patients
The records of all patients who underwent laparoscopic fundoplication at the Department of Pediatric Surgery, University of Tsukuba Hospital, between January 2015 and December 2023 were reviewed retrospectively. We included patients under 16 years of age; however, in cases of patients with neurological impairment, we also included carryover cases older than 16 years. We did not establish any specific exclusion criteria. At our institution, laparoscopic Nissen fundoplication is the primary procedure of choice. However, the final decision on the surgical method was made by the attending surgeon, considering factors such as the feasibility of oral intake by the patient. The endoscopic scope, available in 5- or 10-mm diameter, with a 30° oblique view, was selected based on the surgeon’s preference, and the camera port was always placed at the umbilicus.
A lateral approach is adopted for laparoscopic fundoplication in our institution, and ligation of the short gastric vessels is performed first in the surgical procedure. We extracted scenes involving the dissection of the short gastric vessels from the surgical videos of patients as short-clip videos. The videos were reviewed by two experienced pediatric surgeons, each holding a board certification accredited by the Japanese Society of Pediatric Surgeons, who assessed the visibility of the surgical field. The evaluation criteria for poor visibility included that of the distant view, where the greater curvature of the stomach is generally visible but the gastrosplenic ligament cannot be identified. Additionally, the criteria included instances where the dissection target was not clearly visible or centrally captured on the monitor at close range during the initial dissection of the short gastric vessels (Fig. 1). Cases that met both criteria were categorized as the “poor visibility group”; the others were allocated to the “good visibility group.” In instances in which the two surgeons’ judgments differed, a consensus was reached through discussion.

Intraoperative laparoscopic view of the surgical field in the poor visibility group. (A) In the distant view, the elevated ground prevents distancing from the scope, and the gastrosplenic ligament cannot be properly identified. (B) In the close-up view, the target is visible at a 30° oblique angle, but it cannot be centered on the monitor.
Patient characteristics included sex; age; height; body weight; body mass index (BMI); history of gastrostomy and other abdominal surgeries; presence of congenital heart disease, scoliosis, or Cobb angle; administration of laxatives; and regular use of enemas. The Cobb angle was evaluated using preoperative radiographical images, and scoliosis was defined as a Cobb angle ≥10°. In patients who underwent computed tomography (CT) imaging within six months before or after surgery, the anterior vertebral depth (AVD) to abdominal thickness (AT) ratio and the peritoneum to AVD (PAD) to AT ratio were evaluated based on the sagittal view at the levels of the first lumbar (L1) and third lumbar (L3) vertebrae. AVD was measured as the distance from the skin to the anterior surface of the vertebral body at its center, reflecting the anterior protrusion associated with lordosis. PAD was measured at the same location, providing insight into the spatial relationship between the peritoneum and the vertebral body. AT was defined as the distance from the abdominal wall to the back at the corresponding vertebral level (Fig. 2). These measurements were performed to assess the degree of lordosis at the point where the vertebral body was most prominently anterior. Intraoperative variables included operative time, concurrent gastrostomy, intraoperative blood loss, and intraoperative complications. Operative time was defined as the time from skin incision to wound closure, and intraoperative complications were defined as organ damage requiring additional repair. Furthermore, we investigated the number of surgical experiences that the surgeons had with complex endoscopic surgeries, such as laparoscopic fundoplication, thoracoscopic esophageal atresia repair, choledochal cyst surgery, and thoracoscopic lobectomy.
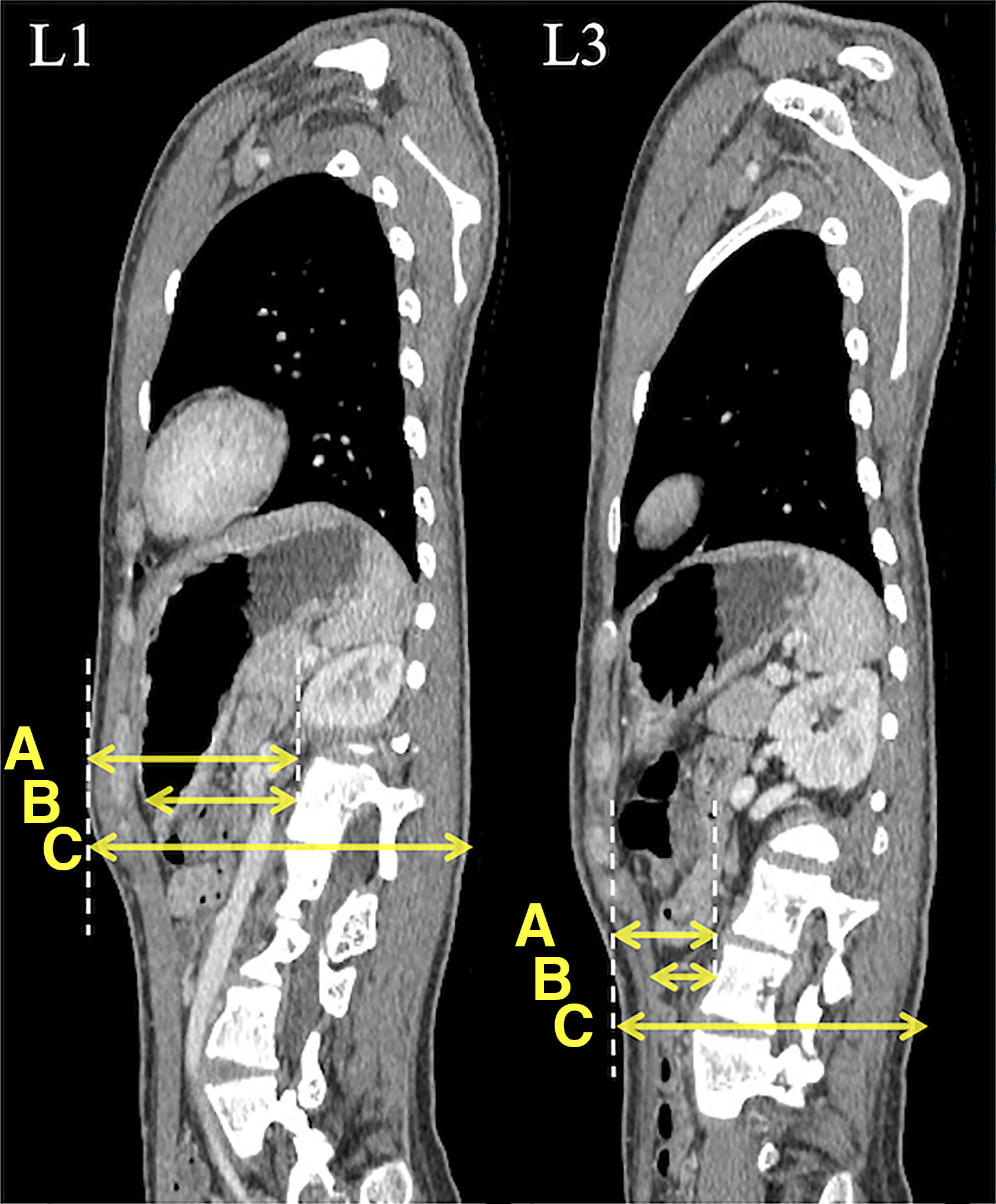
Computed tomography sagittal images of the first lumbar (L1) and third lumbar (L3) vertebrae. (A) Anterior vertebral depth. (B) Peritoneum to anterior vertebral distance. (C) Abdominal thickness.
This retrospective study was conducted according to the principles of the Declaration of Helsinki, as revised in 2013. This study was approved by the institutional review board of the University of Tsukuba Hospital (approval number R06-32). Written informed consent was obtained from all participants and their guardians for the treatment and the use of clinical data.
Statistical analysis
The results are expressed as medians (interquartile ranges) for continuous variables and as percentages for categorical variables in each group. We compared the data between the good and poor visibility groups using Fisher’s exact test and the Mann–Whitney U test. Furthermore, receiver operating characteristic (ROC) curve analysis was performed to determine the cutoff value for the AVD/AT ratio, indicative of poor visibility in the surgical field. All statistical tests were two-sided and the threshold for statistical significance was set at P = .05. All statistical analyses were conducted using GraphPad Prism (10.2.2) software.
Results
During the study period, 41 laparoscopic fundoplications were performed; all were included in the study. These procedures were performed by five surgeons. Among them, two were experienced surgeons, each with ≥30 cases of complex endoscopic surgeries, including laparoscopic fundoplication, while the remaining three were inexperienced surgeons, each with ≤10 such cases. Of the 41 cases, 38 (92.7%) were performed by the experienced surgeons. The procedure was not converted to open surgery in any of the patients, and approximately 70% underwent simultaneous gastrostomy. This study included 27 male and 14 female patients with a median age of 6 years. The assessment of visibility in the surgical field was initially different in the two patients; this led to further discussions and a final judgment from the evaluators. Finally, 21 and 20 patients were assigned to the good and poor visibility groups, respectively. No significant differences were noted in age, sex, height, body weight, BMI, associated congenital heart disease, history of gastrostomy, administration of laxatives, or regular use of enemas. Twenty-one patients were diagnosed with scoliosis, and there were no significant differences in the prevalence thereof, or the Cobb angle, between the two groups. Five patients had a history of abdominal surgery (one with surgery for intestinal atresia repair and four with ventriculoperitoneal shunt placement); they were all in the poor visibility group (P = .048). Additionally, there were no differences in the operative time or intraoperative blood loss between the two groups. However, there were two cases of gastric wall injury, both of which occurred in the poor visibility group (Table 1). CT imaging was performed within 6 months before or after surgery in 22 patients, mostly for the evaluation of associated pneumonia. In those 22 patients, evaluation of AVD/AT and PAD/AT was performed at both the L1 and L3 levels. L3 was not included in the imaging range for one patient. At L1, the AVD/AT and PAD/AT ratios were significantly higher in the good visibility group (n = 14), with median values of 0.653 and 0.575, respectively, compared with 0.559 and 0.433 in the poor visibility group (n = 8), respectively (P = .016 and P = .022, respectively) (Table 2). Similarly, at L3, the AVD/AT and PAD/AT ratios were significantly higher in the good visibility group (n = 14), with median values of 0.577 and 0.476, respectively, compared with 0.492 and 0.358 in the poor visibility group (n = 7), respectively (P = .0018 and P = .0083, respectively) (Table 3). In the ROC curve analysis of the AVD/AT ratio at L1 and L3, the area under the curve (AUC) values were 0.750 and 0.888, respectively, with P-values of .056 for L1 and .0046 for L3. The analysis identified an optimal cutoff value of 0.538 for the L3 AVD/AT ratio, which achieved a sensitivity and specificity of 85.7% for predicting poor visibility in the surgical field (Fig. 3).

Receiver operating characteristic (ROC) curve for anterior vertebral depth/abdominal thickness (AVD/AT) ratio at the first and the third lumbar (L1 and L3) vertebrae. This ROC curve assesses the ability to differentiate between good visibility and poor visibility. The area under the curve (AUC) for the ADV/AT ratio at L3 is 0.888, reflecting diagnostic accuracy.
Characteristics of Patients and Surgeons, Along with Operative Variables
BMI, body mass index; IQR, interquartile range.
Relationship Between Lordosis of the First Lumbar Vertebra and Visibility of the Surgical Field
AVD/AT, anterior vertebral depth to abdominal thickness; L1, first lumbar vertebra; PAD/AT, peritoneum to anterior vertebral depth to abdominal thickness.
Relationship Between Lordosis at the Third Lumbar Vertebra and Visibility in the Surgical Field
AVD/AT, anterior vertebral depth to abdominal thickness; L3, third lumbar vertebra; PAD/AT, peritoneum to anterior vertebral depth to abdominal thickness.
Discussion
In this study, we classified the visibility of the surgical field during laparoscopic Nissen fundoplication in pediatric patients based on actual surgical videos and identified patient factors associated with poor visibility. The Cobb angle, which is commonly used to diagnose and assess the severity of scoliosis, did not affect the visibility of the surgical field. The results of our study indicate that lordosis and a history of abdominal surgery are significantly associated with poor visibility in the surgical field.
Even when muscle relaxants are optimally used and the pneumoperitoneum pressure is precisely set, maintaining an expansive abdominal cavity during surgery can be challenging. This often restricts a surgeon’s ability to achieve a comprehensive overview of the surgical field, thereby compromising visibility. Bektaş et al. identified an intriguing correlation between the exacerbation of lumbar lordosis and the proximity of laparoscopic port entry points at the umbilicus to critical retroperitoneal structures, such as the aorta and inferior vena cava. 9 This association is primarily due to the anterior curvature of the lumbar spine pushing the abdominal and retroperitoneal organs forward, thereby diminishing the available space within the abdominal cavity. Regarding this point, Nagaya et al. reported that in pediatric patients with giant omphaloceles, there is a gradual increase in the abdominal cavity volume after surgery; this is related to an improvement in lumbar lordosis. From this clinical experience, they hypothesized that the curvature of the lumbar vertebrae significantly influences the volumetric capacity of the abdominal cavity. 10 Furthermore, it has also been suggested that kyphoscoliosis may deepen the position of the esophagogastric junction, potentially increasing the difficulty of surgery.5,11 Similarly, in patients with strong lordosis, the surgical ground on the caudal side is elevated, which may deepen the target surgical field and obstruct visibility during surgery.
Regarding the relationship between a history of abdominal surgery and surgical visibility, it is assumed that past abdominal surgeries are associated with poor visibility in the surgical field owing to the formation of adhesions within the abdominal cavity and reduced organ mobility. In this study, 9.8% of the patients had undergone ventriculoperitoneal shunt placement because of hydrocephalus; all these patients were in the poor visibility group. Indeed, 55% of patients with a ventriculoperitoneal shunt undergoing laparoscopic fundoplication have moderate to severe adhesions, resulting in difficulty in identifying vital organs and contributing to poor visibility in the surgical field. 12 Focusing on adults, there are also reports of patients with ventriculoperitoneal shunts undergoing laparoscopic cholecystectomy, in which 57% required open conversion because of adhesions. 13 Rosenfeld et al. retrospectively examined the surgical outcomes of laparoscopic gastrostomy in patients with ventriculoperitoneal shunts and reported no significant differences in operative time or postoperative complications. 14 This lack of variation can be attributed to the simplicity of gastrostomy. Nonetheless, a history of ventriculoperitoneal shunt placement can impede operability in complex surgeries, such as pediatric laparoscopic fundoplication.
In this study, although no significant differences were found, there was a tendency for an increased intraoperative bleeding amount in the poor visibility group, and both cases of gastric wall damage requiring repair occurred in this group. No studies have directly linked surgical visibility to outcomes; however, similar reports have been published. 5 For example, Ishimaru et al. reported that in children with severe scoliosis (Cobb angle >45°), while the total pneumoperitoneum time for laparoscopic fundoplication was similar to that in children without scoliosis, the amount of intraoperative bleeding was significantly higher. 5 However, their study did not address lordosis, and our results suggest that laparoscopic surgeries performed under poor visibility may lead to increases in both intraoperative complications and bleeding amounts, with a significant possibility that these effects are more pronounced with lordosis than with scoliosis. The difficult visibility associated with lordosis can force inappropriate traction to maintain clear sight, as well as dissection and cutting maneuvers conducted under these conditions.
In the current study, the AVD/AT cutoff value of 0.538 at L3 demonstrated a high AUC of 0.888, suggesting that it could be a useful metric for predicting poor surgical fields preoperatively. Although CT imaging is not mandatory before laparoscopic fundoplication, a contrast study of the upper gastrointestinal tract is commonly performed as a preoperative examination. Therefore, at the time of the contrast study, AVD/AT can be assessed using lateral images. If poor surgical fields can be predicted preoperatively, measures, such as positioning the camera port more cranially and having a 45° oblique-viewing scope on standby, can be implemented, potentially enhancing surgical safety. Additionally, assigning the procedure to a surgeon with sufficient surgical experience could further improve outcomes.
This study had some limitations. First, it was a retrospective study conducted at a single institution and the sample size was relatively small; thus, the results may have been subject to bias. Second, the assessment of visibility in the surgical videos was conducted by two experienced pediatric surgeons; however, the lack of objective criteria means that these evaluations could be subjective. Additionally, the visibility of the surgical field can vary significantly depending on the surgeon’s maneuvers, indicating that the surgeon’s skill level may have influenced visibility. Third, many cases involved concurrent gastrostomy. This concurrent gastrostomy may make it difficult to obtain accurate operative times and the amount of bleeding for fundoplication from the anesthetic record. However, there were no significant differences between the two groups in the proportion of patients in whom gastrostomy was performed simultaneously. Therefore, the effects of adjunctive procedures were minimized. Finally, the evaluation of lumbar lordosis in this study was different from the usual evaluation method. In general, it is typically quantified by measuring the angle between the upper endplate of the L1 vertebra and the lower endplate of the L5 vertebra.15–17 In contrast, in this study, the limited imaging availability of the lower lumbar spine led to the adoption of the AVD/AT and PAD/AT ratios at L1 and L3 as surrogate markers. Given that Nissen fundoplication targets the upper abdomen, these metrics are considered effective indicators of lordosis and, by extension, the dimensions of the abdominal cavity.
Despite these limitations, few studies have evaluated the correlation between lordosis, surgical field visibility, and the outcomes of laparoscopic surgery. We are the first, to the best of our knowledge, to clarify that lumbar lordosis is associated with poor surgical visibility in laparoscopic fundoplication, showing that the AVD/AT ratio at the L3 level can be a highly effective indicator of visibility in the surgical field. If it is possible to predict poor visibility and the difficulty of the surgery during the preoperative examination, advance preparation could be highly beneficial for surgeons, enabling safer laparoscopic procedures.
Footnotes
Authors’ Contributions
Y.S.: Conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, and writing—original draft. Y.G.: Investigation, validation, and writing—review and editing. K.M.: Supervision and writing—review and editing.
Data Availability Statement
The data used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.